Pseudomicroangiopathic Thrombotic Syndrome: Unveiling the Vitamin B12 Deficiency Connection
Samia Sabri, Zahida Aqodad, Habiba Alaoui, Houda Bachir, Siham Hamaz, Khalid Serraj

TL;DR
This case report shows how vitamin B12 deficiency can mimic a severe blood disorder and highlights the importance of early diagnosis and treatment.
Contribution
The paper presents a rare case linking vitamin B12 deficiency to TMA-like symptoms, emphasizing the need for clinical awareness.
Findings
A patient with TMA-like symptoms was diagnosed with pernicious anemia due to vitamin B12 deficiency.
Treatment with vitamin B12 supplementation led to rapid clinical improvement.
The case highlights the risk of misdiagnosis without considering vitamin B12 deficiency.
Abstract
Pernicious anemia, a manifestation of vitamin B12 deficiency, can present with a spectrum of hematological abnormalities, sometimes mimicking more severe conditions such as thrombotic microangiopathy (TMA). This case report details a 53-year-old female who presented with significant weight loss, watery diarrhea, and jaundice. Laboratory investigations revealed pancytopenia, hemolysis, and schistocytes, initially suggesting a diagnosis of microangiopathic hemolytic anemia (MAHA). However, significantly low vitamin B12 levels and subsequent bone marrow examination confirmed pernicious anemia with megaloblastic changes. This case underscores the importance of considering vitamin B12 deficiency in the differential diagnosis of patients presenting with TMA-like symptoms. Early recognition and treatment with vitamin B12 supplementation led to rapid clinical improvement and the resolution of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
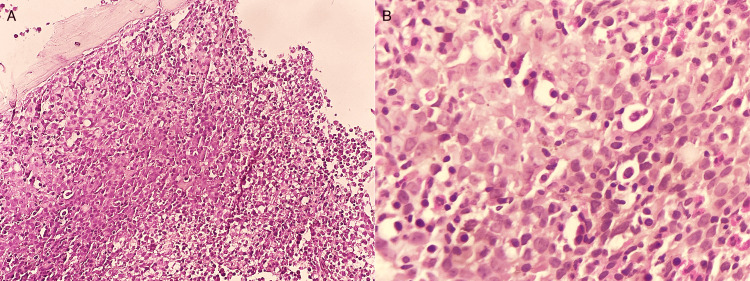 Figure 1
Figure 1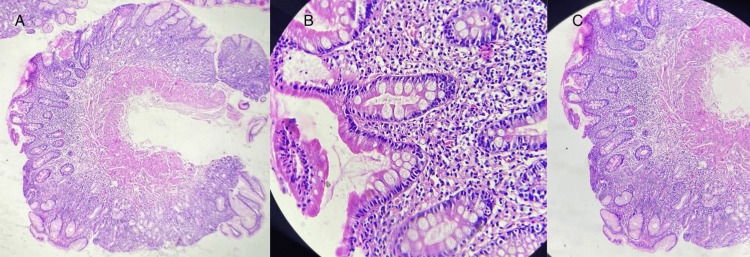 Figure 2
Figure 2| Parameter | Result | Normal Range |
| Hemoglobin (Hb) | 5.1 g/dL | 12-16 g/dL |
| Platelet Count | 62,000/mm³ | 150,000-450,000/mm³ |
| Neutrophil Count | 1,050/mm³ | 1,500-8,000/mm³ |
| Mean Corpuscular Volume (MCV) | 113 fL | 80-100 fL |
| Reticulocyte Count | 92,000/mm³ | >120,000/mm³ |
| Prothrombin Time (PT) | 44% | 70-100% |
| Renal Function | Normal | Normal |
| Haptoglobin | Decreased | 30-200 mg/dL |
| Free Bilirubin | 31 mmol/L | 0-20 mmol/L |
| Lactate Dehydrogenase (LDH) | 1,466 IU/L | 120-240 IU/L |
| Schistocytes | 2.3% | 0% |
| Direct Coombs Test | Positive (IgG) | Negative |
| Vitamin B12 | 50 pg/mL | 200-900 pg/mL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFolate and B Vitamins Research · Neurological and metabolic disorders · Metabolism and Genetic Disorders
Introduction
Vitamin B12 deficiency is a common and potentially serious condition. Clinical manifestations are often initially subtle and develop insidiously [1-4]. These manifestations include sensory polyneuropathy, isolated hematologic abnormalities such as macrocytosis or hypersegmentation of neutrophils, and potentially severe conditions such as combined spinal cord degeneration or hemolytic anemia. In extreme cases, patients may present with pancytopenia and pseudo-thrombotic microangiopathy (TMA) [1,5].
Case presentation
A 53-year-old female with no significant past medical history was admitted to the emergency department with complaints of significant weight loss and watery diarrhea lasting for 10 days. On physical examination, the patient had stable hemodynamics, presented with asthenia, and had non-bloody, non-mucoid liquid diarrhea. Additionally, she exhibited noticeable jaundice without tumor syndrome or hemorrhage.
Laboratory investigations revealed the following results (Table 1).
The combination of anemia, thrombocytopenia, and hemolysis with schistocytes raised concerns for a potential diagnosis of microangiopathic hemolytic anemia (MAHA); however, the absence of renal or neurological impairment was atypical. Vitamin B12 levels were found to be significantly low at 50 pg/mL. Given the pancytopenia and atypical hemolytic anemia, a bone marrow examination was performed, revealing megaloblastic changes (Figure 1). Further testing, including anti-parietal cell antibodies and gastroscopy, confirmed the diagnosis of pernicious anemia (Biermer's disease) with fundic atrophy (Figure 2).
Bone marrow examination showed (A) H&E x 100 showing marked hypercellularity with increased erythroblasts and (B) H&E x400 showing megaloblasts with fine chromatin and marked nucleoli.
Histological examination of gastrointestinal endoscopy biopsies showing (A) atrophy of the fundic mucosa and (B-C) intestinal metaplasia.
The patient's clinical course showed significant improvement following vitamin B12 supplementation, with diarrhea resolving by day four and a reticulocyte crisis by day seven, without the need for additional therapeutic interventions.
Discussion
Although typically benign, vitamin B12 deficiency can have severe consequences, particularly because of its potential clinical atypicality, which threatens prognosis and can lead to significant diagnostic delays. These delays sometimes result in dramatic and irreversible neurological manifestations and/or lesions [4]. Our case underscores this point and adds to the body of literature documenting atypical presentations of cobalamin deficiency.
The classic clinical presentation of vitamin B12 deficiency is macrocytic, nonregenerative anemia. However, more severe presentations, including pancytopenia with signs of hemolysis, can occur in cases of profound deficiency, mimicking TMA. In such cases, it is crucial to rule out thrombotic thrombocytopenic purpura (TTP), a condition associated with high mortality. The use of the PLASMIC score helps stratify the risk of ADAMTS13 (disintegrin and metalloproteinase with thrombospondin motifs 13) deficiency and decide between plasma exchange therapy and simple vitamin B12 supplementation [4,6].
Given the low risk of TTP in our patient (PLASMIC score of 4, the PLASMIC score stands for platelet count/lactate dehydrogenase (LDH) level/acute kidney injury/schistocytes/mean corpuscular volume (MCV)/international normalized ratio (INR)/clinical history of cancer or solid organ transplant, we opted for vitamin B12 supplementation without resorting to plasma exchange therapy. In the study by Federici et al., vitamin B12 deficiency was revealed by pseudo-TMA in 2.5% of cases and by hemolytic anemia in 1.5% of cases [6].
A regenerative hemolytic syndrome can be observed in cases of bone marrow failure (e.g., vitamin deficiency, myelodysplastic syndrome) and chronic hemolysis with folate deficiency. The positivity of the direct Coombs test for IgG is notable. This positivity does not necessarily indicate reduced erythrocyte survival and can result from technical errors, nonspecific binding, hypergammaglobulinemia, or administration of intravenous immunoglobulins (IVIG). Several studies in the literature have found an association between pernicious anemia and a positive Coombs test. The positivity of this test could support the hypothesis of a dysimmune etiology in this vitamin deficiency [7].
Conclusions
In summary, this case underscores the importance of considering atypical presentations of pernicious anemia, which can mimic severe hematological conditions. Prompt recognition and treatment with vitamin B12 supplementation are crucial for preventing complications and improving patient outcomes. Heightened clinical suspicion and timely intervention are essential in managing such cases effectively and mitigating the risk of irreversible neurological damage.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vitamin B 12 (cobalamin) deficiency in elderly patients CMAJ Andrès E Loukili NH Noel E 25125917120041528942510.1503/cmaj.1031155 PMC 490077 · doi ↗ · pubmed ↗
- 2Clinical aspects of cobalamin deficiency in elderly patients. Epidemiology, causes, clinical manifestations, and treatment with special focus on oral cobalamin therapy Eur J Intern Med Andrès E Vidal-Alaball J Federici L Loukili NH Zimmer J Kaltenbach G 4564621820071782265610.1016/j.ejim.2007.02.013 · doi ↗ · pubmed ↗
- 3Neuropsychiatric disorders caused by cobalamin deficiency in the absence of anemia or macrocytosis N Engl J Med Lindenbaum J Healton EB Savage DG 172017283181988337454410.1056/NEJM 198806303182604 · doi ↗ · pubmed ↗
- 4[Signs and symptoms of vitamin B 12 deficiency: critical review of the literature]Med Thérap Serraj K Mecili M Andrès E 1320162010
- 5Hematological findings in patients with food-cobalamin malabsorption Am J Med Andrès E Noel E Maloisel F 592115200310.1016/s 0002-9343(03)00451-014599650 · doi ↗ · pubmed ↗
- 6[Update of clinical findings in cobalamin deficiency: personal data and review of the literature]Rev Med Interne Federici L Henoun Loukili N Zimmer J Affenberger S Maloisel F Andrès E 2252312820071714137710.1016/j.revmed.2006.10.319 · doi ↗ · pubmed ↗
- 7Pernicious anemia with autoimmune hemolytic anemia: a case report and literature review Case Rep Hematol Yeruva SL Manchandani RP Oneal P 2016201610.1155/2016/7231503 PMC 498339327559485 · doi ↗ · pubmed ↗