A Rare Case of Trichilemmal Carcinoma of the Scalp
Raymart Macasaet, FNU Arty, Janelle du Toit, Sai Rakshith Gaddameedi, Shazia M Shah

TL;DR
This paper reports a rare case of a large trichilemmal carcinoma on the scalp in an elderly patient, emphasizing the importance of accurate diagnosis and surgical treatment.
Contribution
The paper presents a rare clinical case of a 12-cm trichilemmal carcinoma and discusses its diagnosis, treatment, and management challenges.
Findings
Trichilemmal carcinoma was initially misdiagnosed as a benign sebaceous cyst but was confirmed via histopathology.
The tumor was successfully excised with no recurrence or complications after one year.
The paper highlights the need for further research on treatment margins and chemotherapy for non-metastatic cases.
Abstract
Trichilemmal carcinoma (TC) is a rare, low-grade, malignant adnexal tumor. It is usually less than 3 cm long and arises from the external root sheath of the hair follicle, most commonly in sun-exposed areas of the body. The treatment of choice is wide local excision with tumor-free margins. We present an 88-year-old male patient who presented with an incidental large, dry, fumigating mass on his scalp for a one-year duration requiring surgical excision. The mass, initially thought to be a benign sebaceous cyst, was a 12-cm trichilemmal carcinoma diagnosed based on the histopathologic features of the mass. The specimen was composed of keratinaceous material and necrotic debris. The viable tumor was consistent with atypical squamous proliferation. The mass was fully excised down to the scalp on the first encounter, leaving no further tissue to excise. The patient’s scalp site remained…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1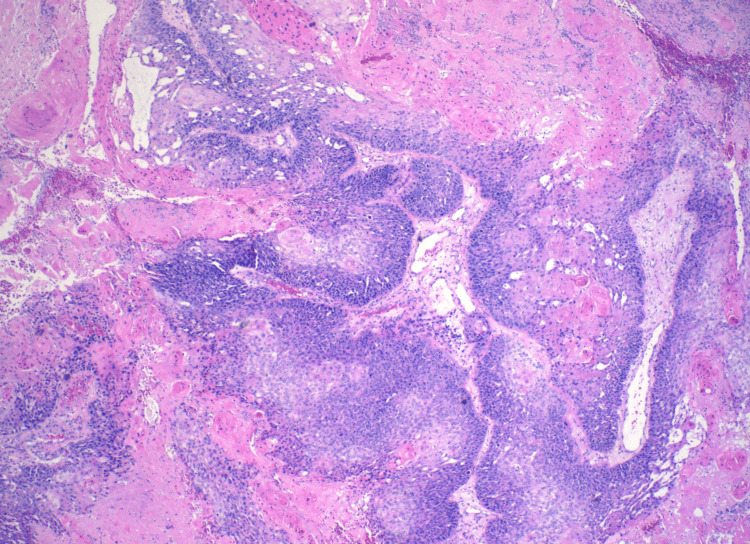 Figure 2
Figure 2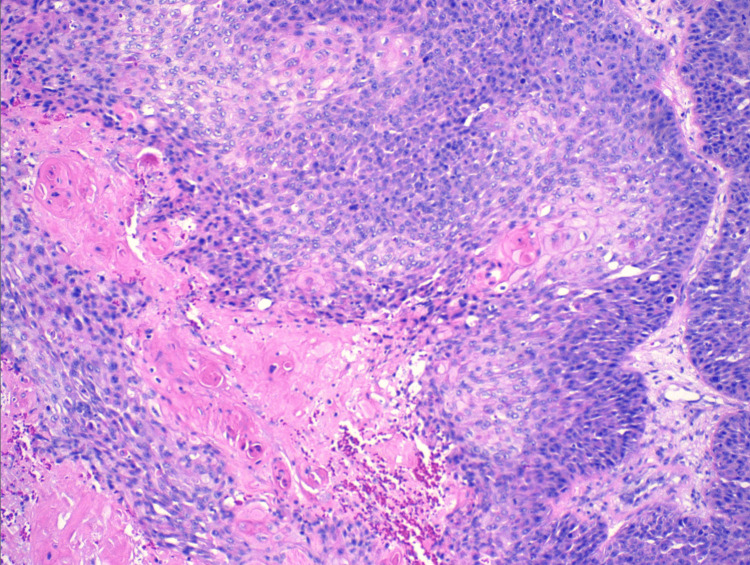 Figure 3
Figure 3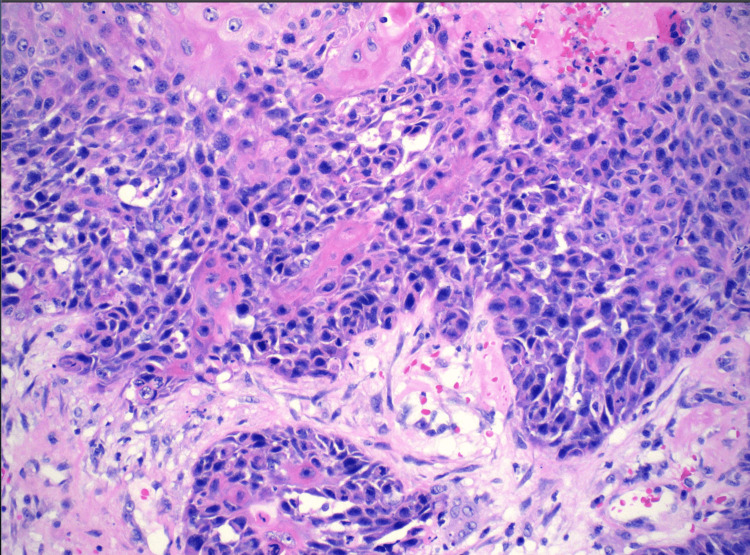 Figure 4
Figure 4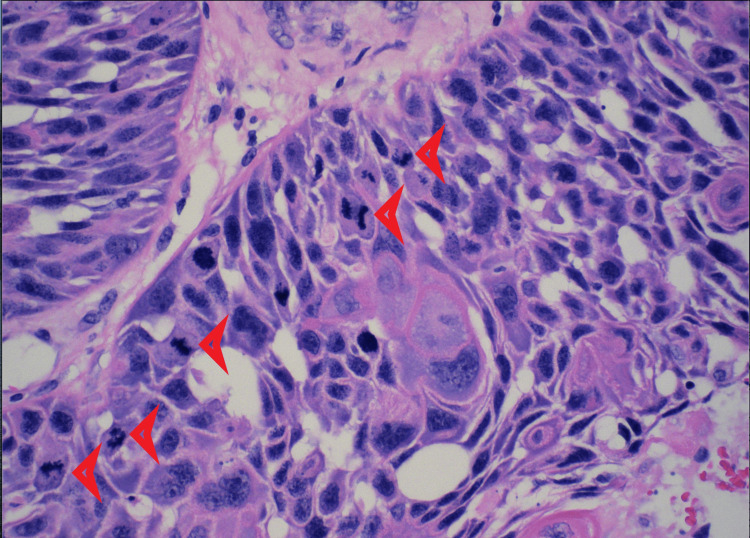 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer and Skin Lesions · Genetic and rare skin diseases. · Nonmelanoma Skin Cancer Studies
Introduction
Trichilemmal carcinoma (TC) is a rare, low-grade, malignant adnexal tumor. It is usually less than 3 cm and arises from the external root sheath of the hair follicle, most commonly in sun-exposed areas of the body [1]. The scalp, neck, and face are the most common sites of involvement. The trunk, back, buttocks, and vulva are occasionally also affected [2]. It was initially identified as tricoleptocarcinoma in 1968 and has an incidence rate of 0.05%. It commonly presents in the elderly population, mainly at the age of 70, with male predominance. The histological similarities to squamous cell carcinoma and the clinical similarity to other benign skin conditions result in delayed diagnosis. Hence, high clinical suspicion and accurate histopathological evaluation are needed for diagnosis confirmation [3]. The absence of a granular layer between the stratum spinosum and stratum corneum in a tumor exhibiting trichilemmal keratinization is the primary histological characteristic that distinguishes a TC from other types of tumors [4]. The treatment of choice is wide local excision with tumor-free margins.
Case presentation
The patient is an 88-year-old male with a past medical history of hypertension, heart failure with a mildly reduced ejection fraction, post-automated implantable cardioverter-defibrillator insertion, bioprosthetic aortic valve replacement, gout, depression, benign prostatic hyperplasia, and obstructive uropathy with a chronic indwelling Foley catheter, which was found to have an incidental scalp mass. The patient’s family sought medical evaluation for the patient due to persistent mass growth that had been ongoing for one year prior. There were no complaints of associated scalp pruritus, bleeding, or discharge. The examination was significant for a large, dry, fumigating scalp mass without bleeding or drainage (Figure 1).
Posterior scalp wound
A surgical excision revealed a scalp mass of 12 cm and was submitted for pathology evaluation. Initially, the mass was suspected to be a benign sebaceous cyst. Pending pathology results, the patient’s scalp site remained clean and was without bleeding or mass recurrence. The patient’s tissue pathology resulted in a positive for trichilemmal carcinoma. Histologically, the tissue illustrates abrupt trichilemmal keratinization and a lack of granular layer (Figures 2-3). Atypical squamous cells, which distinguish trichilemmal carcinoma from the benign variety, were noted (Figures 4-5). The specimen has features of irregular, polygonal, and hyperchromatic nuclei and marked pleomorphism (Figure 4). Figure 5 shows abnormal mitosis (red arrowheads) with numerous inflammatory infiltrates.
Abrupt trichilemmal keratinization and lack of granular layer
Abrupt trichilemmal keratinization and lack of granular layer (high power magnification)
Irregular, polygonal, and hyperchromatic nuclei and marked pleomorphism
Abnormal mitosis (red arrowheads) with numerous inflammatory infiltrates were seen
However, the majority of specimens were composed of keratinaceous material and necrotic debris. The viable tumor was consistent with atypical squamous proliferation with trichilemmal keratinization. Pathology was unable to define margins due to insufficient specimens for such. The patient was re-evaluated by surgery for another specimen. However, since the mass was fully excised down to the scalp on the first encounter, there was no further tissue to be removed. Given the rare diagnosis, this case was discussed with the pathologist in detail. The diagnosis was made based on the histopathologic features of the mass. Being an incidental finding, the medical team could not test for markers. It was decided by the medical and surgical team that chemotherapy and radiation were not needed because there was no evidence of metastasis and there was no tissue left to remove.
Discussion
Trichilemmal carcinoma is a rare, malignant, cutaneous tumor that has a clinically indolent course [5,6]. There is an increasing incidence of this malignancy [7]. It grows from the outer root sheath of hair follicles and can be solitary or multiple [8]. It occurs in the elderly - men ages 60 to 80 years old and women ages over 80 - with no predilection to either sex [5]. The mean age of diagnosis is 70 years old [5]. It is usually seen in fair-skinned individuals in sun-exposed hair-bearing areas such as the scalp and posterior neck [6].
We report a case of an 88-year-old male who has trichilemmal carcinoma that clinically appeared as a large, dry, fumigating mass on the scalp, which was diagnosed by excision. It was initially thought to be a benign sebaceous cyst. Differential diagnoses for TC are squamous cell carcinoma, basal cell carcinoma, and keratoacanthoma, among others [9].
The pathophysiology of this disease is still unclear. The radiation from the sun is one of the factors that causes the growth of the lesions due to its location and distribution [10]. Trichilemmal cysts can also transform into malignant trichilemmal carcinomas due to p53 deletion [11,12].
TC has a non-aggressive course [13], despite its aggressive histology. The prognosis is generally good as it has low metastatic potential, similar to cutaneous squamous-cell carcinoma (SCC) [8,10]. However, TC with metastasis has a poor prognosis, and there is no consensus yet on treatment [8]. A study by Hayashi et al. used the CAV chemotherapy treatment (cisplatin, adriamycin, and vindesine), which is the regimen for highly advanced cases of SCC [14,15]. Yi et al. reported a case of a 60-year-old woman with malignant TC who underwent four cycles of cisplatin and cyclophosphamide treatment but only achieved a partial remission [16]. The patient eventually died.
For non-metastatic TC, simple surgical excision with an adequate (0.5-1 cm) margin is an effective treatment [8,12]. It is low-cost and safe [7,8]. Mohs micrographic surgery is also an option and has been used as a treatment in several case reports [17,18]. There are also patients with trichilemmal carcinoma treated with 5% topical Imiquimod cream [18,19]. The patient in this case report was treated with surgical excision, and there was no recurrence noted after two months. At present, there are no established follow-up guidelines for patients with TC after surgical excision. It is important to monitor patients to catch early recurrence and metastasis. In a 14-year study by Xu et al., they reported a median follow-up of 63.8 months in patients with trichilemmal carcinoma [20].
Conclusions
Trichilemmal carcinoma has been increasing in incidence. It is a rare adnexal tumor of low metastatic potential that can safely be treated with simple excision. We report a rare case of non-metastatic trichilemmal carcinoma that was treated safely and effectively by simple excision. Different studies use different margins, and there is no consensus on the measurement for margin excision. The patient was followed up after two months, and regular follow-up is recommended. However, further studies regarding the follow-up schedule are needed. In addition, in cases of malignant TC, treatment with chemotherapy is commonly used, but there are only limited studies investigating this. The patient did not undergo chemotherapy and radiation as there was no evidence of metastasis, and the mass was fully excised. More research to address the knowledge gap in malignant TC management is highly recommended, given the increasing incidence of the disease.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Trichilemmal carcinoma: review of 8 cases J Cutan Pathol Reis JP Tellechea O Cunha MF Baptista AP 4449201993846841610.1111/j.1600-0560.1993.tb 01248.x · doi ↗ · pubmed ↗
- 2Proliferating epithelial cysts. Clinicopathological analysis of 96 cases J Cutan Pathol Sau P Graham JH Helwig EB 394406221995859407110.1111/j.1600-0560.1995.tb 00754.x · doi ↗ · pubmed ↗
- 3Proliferating trichilemmal cyst: a simulant of squamous cell carcinoma Cancer Brownstein MH Arluk DJ 12071214481981626828010.1002/1097-0142(19810901)48:5<1207::aid-cncr 2820480526>3.0.co;2-1 · doi ↗ · pubmed ↗
- 4Eyelid trichilemmal carcinoma Saudi J Ophthalmol Chai MK Tenzel P Iacob C Jordan A Reddy HS 1831853120172886092010.1016/j.sjopt.2017.05.002PMC 5569329 · doi ↗ · pubmed ↗
- 5Systematic analysis and case series of the diagnosis and management of trichilemmal carcinoma Front Oncol Sun J Zhang L Xiao M Li S Chen R Li Y Yang Y 10782721220223672705610.3389/fonc.2022.1078272 PMC 9886092 · doi ↗ · pubmed ↗
- 6Trichilemmal carcinoma from proliferating trichilemmal cyst on the posterior neck Arch Craniofac Surg Kim UG Kook DB Kim TH Kim CH 50531820172891330410.7181/acfs.2017.18.1.50PMC 5556745 · doi ↗ · pubmed ↗
- 7Trichilemmal carcinoma--a rare tumor: case report Acta Dermatovenerol Croat PeryassúBC PeryassúRC PeryassúMA Maceira JP Ramos-E-Silva M 2830162008 https://pubmed.ncbi.nlm.nih.gov/18358106/18358106 · pubmed ↗
- 8Survival study and clinicopathological evaluation of trichilemmal carcinoma Mol Clin Oncol Zhuang SM Zhang GH Chen WK Chen SW Wang LP Li H Song M 499502120132464919910.3892/mco.2013.74PMC 3915649 · doi ↗ · pubmed ↗