Reaching the ideal cardiovascular health: is this the key to preventing multiple long-term conditions?
Yogini V. Chudasama, Kamlesh Khunti

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
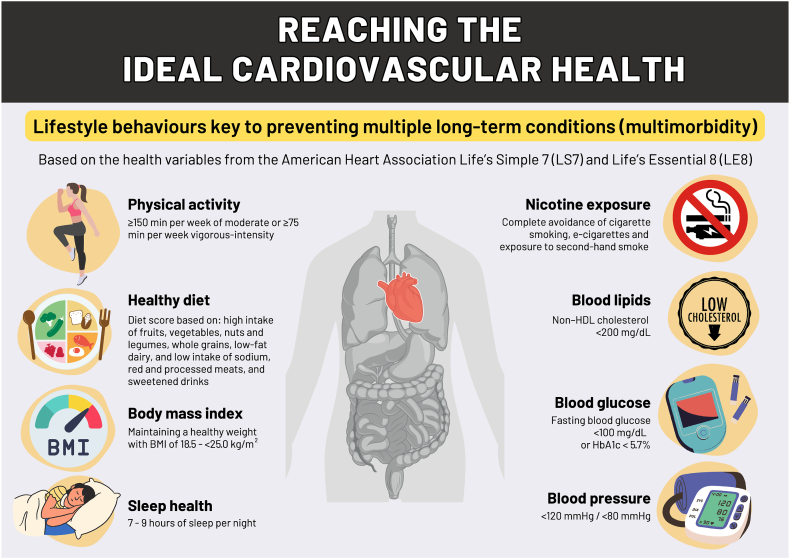 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Health and Risk Factors · Cardiac Health and Mental Health · Health, Environment, Cognitive Aging
Multiple long-term conditions (MLTCs) or multimorbidity, has become a major health problem globally due to an ageing population.1^,^2 However, the increased prevalence of chronic conditions is not only due to an ageing population but also due to a combination of rising prevalence of obesity and a shift to unhealthy lifestyle behaviours in recent decades.3 Therefore, targeting patient lifestyle behaviours could significantly help to prevent and reduce the current epidemic of MLTCs. The American Heart Association launched the concept of the ideal ‘cardiovascular health’ measured using Life's Simple 7 (LS7) and Life's Essential 8 (LE8), Fig. 1.4 Previous studies have demonstrated the associations between higher cardiovascular health and lower risk of single chronic conditions, and MLTCs in two studies.5^,^6 Yet, to date, there has not been a study exploring the association of the change in cardiovascular health and the risk of developing MLTCs.Fig. 1. Summary of the ideal cardiovascular health based on the American Heart Association Life's Simple 7 (LS7) and Life's Essential 8 (LE8). Multiple long-term conditions (multimorbidity), two or more long-term conditions; min, minutes; BMI, body mass index; non-HDL, non-high-density lipoprotein cholesterol; e-cigarettes, electronic cigarettes.Figure 1 was created by YC using Canva. All graphical elements used in the figure are either original or sourced from Canva's licensed library.
In this issue of the Lancet Regional Health–Europe, Prugger and colleagues add an important study to the literature by investigating the relationship between changes in cardiovascular health over time and subsequent MLTC risk using community-based cohorts from the UK and Finland.7 MLTC in the study was defined as 2 or more of 12 chronic conditions. The primary analysis was based on 9715 participants from the Whitehall II multi-wave prospective cohort study in the UK, and the validation cohort of 75,377 participants from the Finnish Public Sector cohort study in Finland. The main finding was that both LS7 and LS8 assessments were associated with a lower risk of incident MLTC. In the UK cohort, the risk of MLTC decreased by 8% (hazard ratio 0·92, 95% confidence interval 0·88–0·96) per one ideal LS7 metric increase over 5 years and by 14% (0·86, 0·80–0·93) per 10-point increase in LE8 score over 10 years. These results were robust to comprehensive sensitivity analyses and confirmed in terms of change in cardiovascular health over 4 years in the validation analysis. For both Whitehall II and Finnish study populations, the population preventable fractions (PPF) indicated that achieving ≥2 ideal LS7 metrics based on the corresponding hazard ratio and prevalence was estimated to prevent 53% of individuals from developing MLTC who initially lacked any LS7 metrics.
The main strengths of this paper were specifically the longer length of follow-up (median 31·4 years), observing incidence of MLTCs, using both LS7 and LS8 assessments, validation cohort, and several sensitivity analyses. However, this study is not without limitations; the diet component was missing from the validation Finnish cohort, and no other proxy was used to replace the missing diet variable. Additionally, the Whitehall II cohort was over-represented by people of White ethnicity, men and British civil servants working in London offices, thus the findings limit generalisability to other social and ethnic groups. There has been greater attention on ethnic and social health inequalities due to the higher prevalence of MLTCs in these populations,8 thus further research on cardiovascular health and the risk of MLTC may benefit from larger national datasets with stratified analyses to identify whether the findings differ between patient demographics. The assessment scores could therefore be further developed and tailored to suit these populations as they have different dietary patterns than those in the US, vary in physical activity levels, and the ethnic minority populations differ in body mass index compared to White Caucasians. Lastly, the study focused on the development of 12 chronic conditions over time. We agree with the authors that a larger list of conditions makes the concept meaningless for clinicians and for identifying prevention targets, though, the current literature holds inconsistent definitions and approaches to measuring MLTC.9 For this reason, future studies relating to MTLC would benefit from using the definition of MLTC defined by the Delphi consensus study from a panel of international experts that selected 24 main conditions, to help facilitate consistency and comparison of studies.10 This may also help prevent non-cardiovascular related MLTCs.
MLTCs affect each individual at some point in their life, either personally or through family, friends, or work. It has a major impact on quality of life as it deteriorates over time, leads to poorer health outcomes, and accounts for a higher healthcare workload, costs, and mortality. This new study provides us with evidence indicating that reaching the ideal cardiovascular health could potentially have prevented over half of the participants from developing MLTC. Therefore, we should start focusing on the immediate causes which are obstructing individuals from reaching their ideal cardiovascular health to be able to minimise and prevent future diagnoses of MTLCs.
Contributors
YC–Writing original draft & figure design.
KK–Writing, review & editing.
Declaration of interests
KK is the National Lead for multiple long-term conditions (MLTC) for the National Institute for Health Research Applied Research Collaboration (NIHR ARC), Co-Director of the NIHR Global Centre for MLTC and Co-Chair of the National MLTC Cross NIHR Collaboration.
YC has no competing interests.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Khunti K.Sathanapally H.Mountain P.Multiple long term conditions, multimorbidity, and co-morbidities: we should reconsider the terminology we use BMJ 3832023 p 232710.1136/bmj.p 232737832952 · doi ↗ · pubmed ↗
- 2Khunti K.Chudasama Y.V.Gregg E.W.Diabetes and multiple long-term conditions: a review of our current global health challenge Diabetes Care 46122023209221013801152310.2337/dci 23-0035 PMC 10698221 · doi ↗ · pubmed ↗
- 3The Academy of Medical Sciences April 2018 Multimorbidity: a priority for global health researchhttps://acmedsci.ac.uk/file-download/822225772018
- 4Lloyd-Jones D.M.Allen N.B.Anderson C.A.Life's essential 8: updating and enhancing the American Heart Association's construct of cardiovascular health: a presidential advisory from the American Heart Association Circulation 14652022 e 18e 433576602710.1161/CIR.0000000000001078 PMC 10503546 · doi ↗ · pubmed ↗
- 5Wang X.Ma H.Li X.Association of cardiovascular health with life expectancy free of cardiovascular disease, diabetes, cancer, and dementia in UK adults JAMA Intern Med 183420233403493684812610.1001/jamainternmed.2023.0015 PMC 9972243 · doi ↗ · pubmed ↗
- 6Zhang Y.Sun M.Wang Y.Association of cardiovascular health using Life's Essential 8 with noncommunicable disease multimorbidity Prev Med 174202310760710.1016/j.ypmed.2023.10760737414227 · doi ↗ · pubmed ↗
- 7Prugger C.Perier M.-C.Sabia S.Association between changes in cardiovascular health and the risk of multimorbidity: community-based cohort studies in the UK and Finland Lancet Reg Health Eur 42202410.1016/j.lanepe.2024.100922 PMC 1109895038764806 · doi ↗ · pubmed ↗
- 8Valabhji J.Barron E.Pratt A.Prevalence of multiple long-term conditions (multimorbidity) in England: a whole population study of over 60 million people J R Soc Med 117320241041173790552510.1177/01410768231206033 PMC 11046366 · doi ↗ · pubmed ↗