Pneumonia in Geriatric Patients and Prediction of Mortality Based on the Pneumonia Severity Index (PSI), CURB-65, Frailty Index (FI), and FI-Lab21 Scores
Firdaus Jabeen, Ajay Mishra, Saboor Mateen, Ankit Maharaj, Rishabh Kapoor, Syed Faraz Abbas, Shahedullah Khan, Abhinaya Gupta

TL;DR
This study finds that the Pneumonia Severity Index (PSI) best predicts mortality in elderly pneumonia patients compared to other scores.
Contribution
The study demonstrates that PSI is more accurate than CURB-65, Frailty Index, and FI-Lab21 in predicting mortality in geriatric pneumonia patients.
Findings
The 30-day mortality rate among elderly CAP patients was 57%.
PSI score and severe frailty were significant independent risk factors for mortality.
PSI had the highest predictive accuracy (92%) with an AUC of 0.952 for mortality prediction.
Abstract
Background Elderly individuals have higher rates of morbidity, death, and financial burden due to community-acquired pneumonia (CAP). Objectives The study aimed to assess the outcomes of geriatric pneumonia patients and the prediction of mortality based on the pneumonia severity index (PSI), CURB-65 (confusion, urea, respiratory rate, blood pressure, and 65-year-old score), frailty index (frailty index), and FI-Lab21 (21-item frailty index based on laboratory) scores. Methods A prospective observational study was conducted on 100 elderly patients (≥ 65 years) with CAP. PSI, CURB-65, FI, and FI-Lab21 scores were determined. The outcome measures were 30-day mortality and the risk factors of mortality. The mortality predictive value of scores were compared. Results The mean age of the study subjects was 72.14 ± 6.1 years. Specifically, 76 (76%) were male, and 24 (24%) were females.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
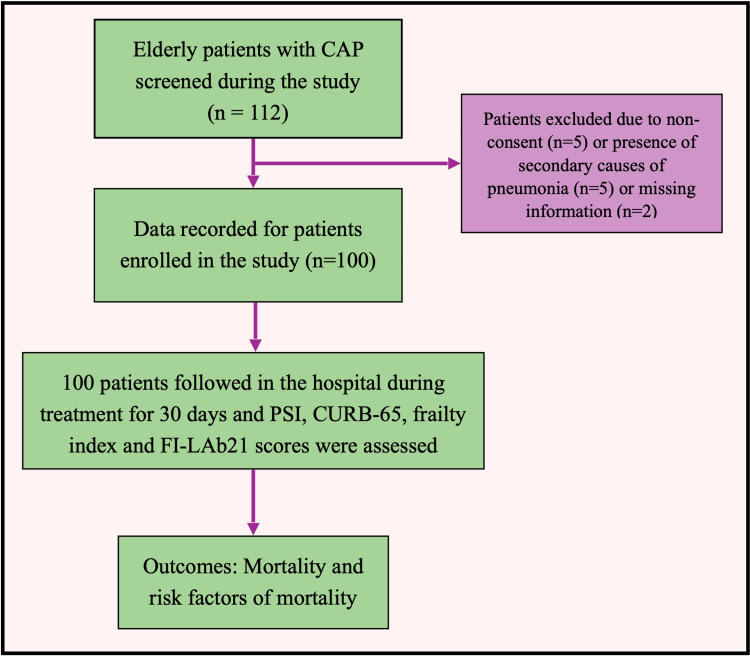 Figure 1
Figure 1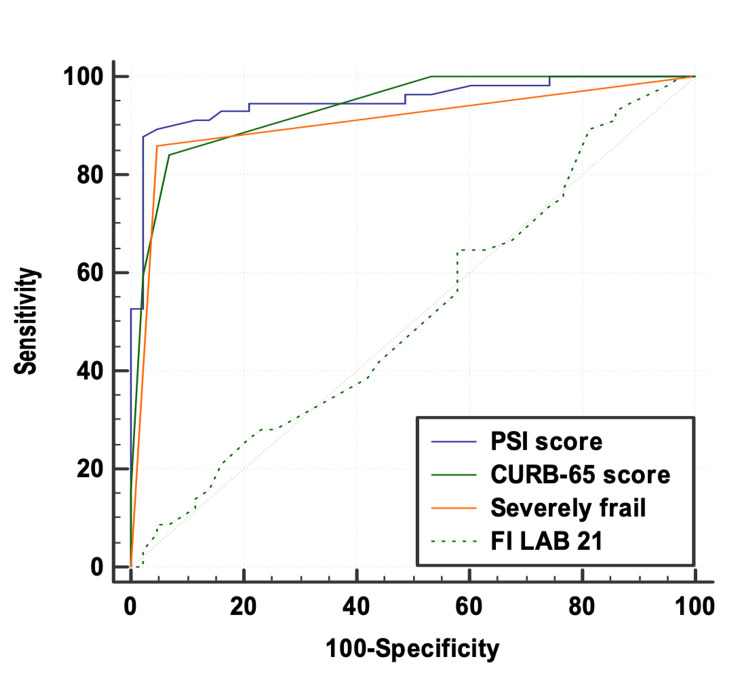 Figure 2
Figure 2| Patient characteristics | Number (Percentage %) | Mean ± SD | Median (25th-75th percentile) | Range |
| Age (years) | N/A | 72.14 ± 6.1 | 70 (67-75) | 65-90 |
| Gender | ||||
| Female | 24 (24%) | N/A | N/A | N/A |
| Male | 76 (76%) | |||
| FI | ||||
| Robust | 20 (20%) | N/A | N/A | N/A |
| Moderate frail | 29 (29%) | |||
| Severely frail | 51 (51%) | |||
| Hypertension | 62 (62%) | N/A | N/A | N/A |
| Type II diabetes mellitus | 55 (55%) | N/A | N/A | N/A |
| History of CHF | 16 (16%) | N/A | N/A | N/A |
| History of cerebrovascular disease | 5 (5%) | N/A | N/A | N/A |
| History of renal disease | 4 (4%) | N/A | N/A | N/A |
| Confusion | 45 (45%) | N/A | N/A | N/A |
| PSI score | N/A | 133.56 ± 41.03 | 126 (99.75-173.5) | 67-235 |
| CURB-65 score | N/A | 2.75 ± 1.29 | 3 (2-4) | 1-5 |
| FI-Lab21 | N/A | 0.4 ± 0.14 | 0.38 (0.31-0.46) | 0.1-0.93 |
| Patient characteristics | Discharged (n=43) | Expired (n=57) | Total | P value |
| Age(years) | 70.09 ± 4.79 | 73.68 ± 6.6 | 72.14 ± 6.13 | 0.002‡ |
| Gender | ||||
| Female | 14 (32.56%) | 13 (22.81%) | 27 (27%) | 0.277† |
| Male | 29 (67.44%) | 44 (77.19%) | 73 (73%) | |
| FI | ||||
| Robust | 20 (46.51%) | 0 (0%) | 20 (20%) | <.0001† |
| Moderate frail | 21 (48.84%) | 8 (14.04%) | 29 (29%) | |
| Severely frail | 2 (4.65%) | 49 (85.96%) | 51 (51%) | |
| Hypertension | 28 (65.12%) | 34 (59.65%) | 62 (62%) | 0.577† |
| Type II diabetes mellitus | 19 (44.19%) | 36 (63.16%) | 55 (55%) | 0.059† |
| History of CHF | 7 (16.28%) | 9 (15.79%) | 16 (16%) | 0.947† |
| History of cerebrovascular disease | 2 (4.65%) | 3 (5.26%) | 5 (5%) | 1* |
| History of renal disease | 1 (2.33%) | 3 (5.26%) | 4 (4%) | 0.632* |
| Confusion | 2 (4.65%) | 43 (75.44%) | 45 (45%) | <.0001* |
| PSI score | 97.58 ± 19.52 | 160.7 ± 30.78 | 133.56 ± 41.03 | <.0001‡ |
| CURB-65 score | 1.63 ± 0.69 | 3.6 ± 0.94 | 2.75 ± 1.29 | <.0001‡ |
| FI-Lab21 | 0.39 ± 0.15 | 0.4 ± 0.13 | 0.4 ± 0.14 | 0.812‡ |
| Variables | Beta coefficient | Standard error | P value | Odds ratio | Odds ratio Lower bound (95%) | Odds ratio upper bound (95%) |
| Age (years) | -0.104 | 0.084 | 0.216 | 0.901 | 0.764 | 1.063 |
| PSI score | 0.045 | 0.018 | 0.014 | 1.046 | 1.009 | 1.085 |
| CURB-65 score | 0.631 | 0.522 | 0.227 | 1.879 | 0.676 | 5.224 |
| Robust/moderate frail/severely frail | ||||||
| Robust | N/A | N/A | N/A | 1.000 | N/A | N/A |
| Moderate frail | 2.026 | 1.606 | 0.207 | 7.582 | 0.326 | 176.618 |
| Severely frail | 3.955 | 1.937 | 0.041 | 52.213 | 1.173 | 2323.655 |
| Confusion | 0.001 | 1.236 | 0.999 | 1.001 | 0.089 | 11.284 |
| Variables | PSI score | CURB-65 score | Severely frail | FI-Lab21 |
| Area under the ROC curve (AUC) | 0.952 | 0.936 | 0.907 | 0.515 |
| Standard error | 0.0215 | 0.0216 | 0.0283 | 0.0591 |
| 95% Confidence interval | 0.910-0.994 | 0.893-0.978 | 0.851-0.962 | 0.400-0.631 |
| P value | <0.0001 | <0.0001 | <0.0001 | 0.7956 |
| Cutoff | >121 | >2 | - | >0.26 |
| Sensitivity (95% CI) | 87.72% (76.3-94.9%) | 84.21% (72.1-92.5%) | 85.96% (74.2-93.7%) | 89.47% (78.5-96.0%) |
| Specificity (95% CI) | 97.67% (87.7-99.9%) | 93.02% (80.9-98.5%) | 95.35% (84.2-99.4%) | 18.6% (8.4-33.4%) |
| PPV (95% CI) | 98% (89.6-100.0%) | 94.1% (83.8-98.8%) | 96.1% (86.5-99.5%) | 59.3% (48.2-69.8%) |
| NPV (95% CI) | 85.7% (72.8-94.1%) | 81.6% (68.0-91.2%) | 83.7% | 57.1% (28.9-82.3%) |
| Diagnostic accuracy | 92% | 88% | 90% | 59% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDutch Social and Cultural Studies
Introduction
Population aging (referring to the demographic shift towards an increasing proportion of older adults) [1] has brought on a range of implications for health [2]. Projections suggest that, by 2050, approximately 21% of the global population will be classified as elderly [3].
As individuals age, their risk of developing community-acquired pneumonia (CAP) rises, significantly affecting morbidity and mortality among the elderly [4]. The reported incidence rates of CAP in different populations vary between 1.3 and 11.6 cases per 1,000 inhabitant-years, with the highest rates in elderly adults (13-15 cases per 1,000 inhabitant-years) [5].
Unlike in younger adults, pneumonia in older adults presents with unclear onset, atypical clinical signs, numerous complications, and a complex underlying cause due to age-related changes and existing medical conditions. These factors contribute to delays in diagnosis and treatment, ultimately leading to higher short-term and long-term mortality rates in this population [6].
Since the elderly population is frail, defined by a decline in biological reserves, the breakdown of homeostatic mechanisms, and heightened susceptibility to various challenges or adversities, the prognosis among them remains adverse in relation to the severity of the disease. Predicting mortality risk among them becomes crucial for risk stratification and improving outcomes [7,8].
Common tools such as the pneumonia severity index (PSI), frailty index (FI) [9,10], 21-item FI based on laboratory (FI-Lab21) values, and CURB-65 (confusion, urea, respiratory rate, blood pressure, and 65-year-old score) [8] are frequently utilized for this purpose. However, these tools may have limitations when applied to older patients due to factors such as comorbidities, age-related physiological changes, and practical application difficulties [7,8].
Studies remain sparse in assessing which of these scores holds superiority over another for predicting mortality risk in elderly patients with pneumonia. Thus, we conducted this study wherein all scores were included, and we assessed the outcomes in terms of these scores among aged patients presenting with pneumonia.
Materials and methods
A prospective observational study was conducted on 100 elderly patients who presented to the OPD with CAP. Ethical committee clearance was obtained before initiating the study, and informed consent was obtained from the patients before they were enrolled. The study was conducted over a period of 24 months from April 2022 to March 2024. The sample size calculation was based on the study by Zan et al. [9]. In their research, they found that the AUC values for FI-Lab, PSI, and CURB-65 in predicting mortality were 0.783, 0.812, and 0.799, respectively. With that reference value, along with a significance level of 5% and a specified δ of 0.065, the calculated sample size was 99 patients.
Selection criteria
Patients aged ≥65 years hospitalized with CAP during the study period were included. The exclusion criteria were secondary causes of pneumonia, such as active tuberculosis, bronchiectasis, cystic pulmonary fibrosis, lung abscesses, Pneumocystis carinii pneumonia, radiation pneumonia, or patients with incomplete data (including clinical information, auxiliary examination results, etc.).
Methodology
The data of patients on demographics, comorbidities, and vital signs were collected on a pre-designed questionnaire. Clinical presentation was noted, which included fever, cough with or without sputum production, dyspnea, fatigue, anorexia, chest discomfort, delirium, lethargy, and a history of falls. Pneumonia was diagnosed based on clinical and laboratory findings such as arterial blood gas (ABG), complete blood count (CBC), electrolytes (sodium, potassium, chloride, calcium, magnesium, phosphate), blood urea nitrogen (BUN), procalcitonin (PCT), C-reactive protein (CRP), blood culture, and sputum culture. Chest X-ray was done on all patients.
Standards and criteria
An FI [11] was determined by assessing 50 factors at baseline, including 25 comorbidities, taking more than five prescription drugs, self-reported ability to perform 21 activities, experiencing weight loss of over 5 kg in the past year, having a body mass index (BMI) below 21, and having a serum albumin level below 3.5 g/L. Using the FI scale, which ranges from 0 to 1, patients were categorized as robust (<0.15), pre-frail (range: 0.15-0.24), mildly to moderately frail (range: 0.25-0.44), or severely frail (≥0.45) [12]. Based on admission information, the PSI [13] (range: 0-395) and CURB-65 [12] (range: 0-5) scores were calculated. The PSI is composed of 20 clinical, exploratory, and analytical variables, whereas the CURB-65 assesses the level of consciousness, blood urea, systolic blood pressure, respiratory rate, and age of patients. The FI-Lab21 score, a 21-item FI based on laboratory blood and urine tests, was also assessed [14]. The patients were followed up for discharge and mortality up to 30 days. Any patient discharged before 30 days was followed up telephonically until 30 days. The outcome measures were 30-day mortality and risk factors of mortality.
Statistical analysis
Quantitative data, assuming a normal distribution, were expressed as means with standard deviations, while categorical variables were presented as counts and percentages. Tests included the independent t-test for quantitative variables and the chi-square test (or Fisher’s exact test, if necessary) for qualitative variables. Receiver operating characteristic (ROC) analysis was applied to determine the predictive values for mortality using the PSI score, CURB-65 score, severely frail, and FI-Lab21, with the DeLong test for comparative analysis. Multivariate logistic regression identified significant mortality risk factors. Data were initially entered in Microsoft Excel and analyzed using Statistical Product and Service Solutions (SPSS, version 25.0; IBM SPSS Statistics for Windows, Armonk) software. A p-value of <0.05 indicated statistical significance across all analyses.
Results
During the study period, 112 patients were found eligible, of which five were excluded because of no consent, five were excluded because they had secondary causes of pneumonia, and two were excluded because of missing data. Thus, 100 patients were evaluated for the study (Figure 1).
Study flow diagramCAP: Community-acquired pneumonia; CURB-65: Confusion, urea, respiratory rate, blood pressure, and 65-years-old score; FI-Lab21: Frailty index associated with laboratory values; PSI: Pneumonia severity index
Demographic characteristics
The mean age of the study subjects was 72.14 ± 6.1 years. Specifically, 76 (76%) were male, and 24 (24%) were females. Regarding frailty status, 51% (n=51) of cases were severely frail, 29% (n=29) were moderately frail, and 20% (n=20) were classified as robust. Hypertension was present in 62% (n=62) of cases, type II diabetes mellitus in 55% (n=55), confusion in 45%, a history of congestive heart failure (CHF) in 16%, cerebrovascular history in 5%, and a history of renal disease in 4% patients. The mean values of the PSI score, CURB-65 score, and FI-Lab21 score were 133.56 ± 41.03, 2.75 ± 1.29, and 0.4 ± 0.14, respectively (Table 1).
Outcomes
During the follow-up, there was a 30-day mortality rate of 57%, while 43% of cases were discharged. Compared to survivors, non-survivors were significantly more severely frail (85.96% vs. 4.65%, p<0.0001); had significantly more confusion (75.44% vs. 4.65%, p<0.0001); had significantly higher ages (73.68 ± 6.6 vs. 70.09 ± 4.79 years, p=0.002); had more PSI scores (160.7 ± 30.78 vs. 97.58 ± 19.52, p<0.0001); and had higher CURB-65 scores (3.6 ± 0.94 vs. 1.63 ± 0.69, p<0.0001), but they had similar FI-Lab21 (0.4 ± 0.13 vs. 0.39 ± 0.15, p=0.812) and similar gender distribution and comorbidities (p>0.05, Table 2).
Risk factors of mortality
On performing multivariate regression, the PSI score and severely frail were significant independent risk factors of mortality, with odds ratios of 1.046 and 52.213, respectively, after adjusting for confounding factors (Table 3).
Mortality prediction of scores
ROC curves above the diagonal line are considered to have a reasonable discriminating ability to predict mortality. Interpretation of the AUC showed that the performance of the PSI score (AUC: 0.952; 95% CI: 0.910-0.994), CURB-65 score (AUC: 0.936; 95% CI: 0.893-0.978), and severely frail (AUC: 0.907; 95% CI: 0.851-0.962) was outstanding. On the other hand, the discriminatory power of FI-Lab21 (AUC: 0.515; 95% CI: 0.400-0.631) was non-significant. FI-Lab21 had a sensitivity of 89.47%, followed by the PSI score (87.72%), severely frail (85.96%), and CURB-65 score (84.21%) for predicting mortality. The PSI score had a specificity of 97.67%, followed by severely frail (95.35%), CURB-65 score (93.02%), and FI-Lab21 (18.60%) for predicting mortality. Among all the parameters, the PSI score was the best predictor of mortality at cutoff points of >121 with an AUC of 0.952 for correctly predicting mortality (Table 4).
No significant difference was seen in the AUC of the PSI score, CURB-65 score, and severely frail for predicting mortality. However, FI-Lab21 had a significantly lower AUC as compared to the PSI score, CURB-65 score, and severely frail for predicting mortality (p<0.0001; Figure 2).
Comparison of the area under the curve of the PSI score, CURB-65 score, severely frail, and FI-Lab21 for predicting mortality (DeLong test)PSI: Pneumonia severity index; FI-Lab21: Frailty index associated with laboratory values; CURB-65: confusion, urea, respiratory rate, blood pressure, and 65 years old score
Discussion
The lethality of pneumonia tends to increase with age, especially in patients over 65 years. Specifically, age ≥ 90 years is reported to be markedly associated with mortality due to pneumonia [15,16]. Our study observed a high mortality rate in elderly CAP patients, wherein 57% of patients died and 43% survived. In comparison, Nascè et al. [17] found that, out of 200 suspected pneumonia patients, 60 died, resulting in a mortality rate of 30%. In the study by Zan et al. [9], out of 495 participants, 74 (15%) died and 421 (85%) survived. In Park et al. [18], out of 190 patients, 53 (27.9%) died and 137 (72.1%) survived. Baek et al. [19] reported that, out of 160 patients with severe pneumonia, 40 (25%) died. In a study by Ilg et al. [20], on 2,322 patients suspected of pneumonia, 97 (4.2%) died in hospital. Overall, the mortality rate has been lower in previous studies compared to our study. These values may differ based on the populations studied, hospital facilities, and the severity of the disease. Such a high mortality rate in the elderly can be attributed to frailty or various comorbidities, such as hypertension, diabetes mellitus, CHF, cerebrovascular disease, and renal disease, as observed in our study. Studies have consistently shown the association of factors such as age (p<0.01), being critically ill (p<0.01), and the presence of comorbidities (p<0.01) with mortality [9,17]. Studies have also found lower BMI and hypoalbuminemia as independent prognostic factors associated with five-year mortality [18,21], though these factors were not assessed in the present study.
Similarly, when we compared the factors among those who died and those who survived, we found that higher age and severe frailty were significantly associated with mortality. However, after adjusting for confounding factors, multivariate logistic regression showed that age, gender, and comorbidities were not significantly associated with mortality. However, patients who were severely frail showed poor outcomes, with an odds ratio of 52.213 (p=0.041), which was in line with the studies by Zan et al. [9] and Park et al. [18]. Among the various scores assessed, only the PSI score was found to be a significant independent risk factor for mortality, with an odds ratio of 1.046 (95% CI: 1.009-1.085, p=0.014). In terms of predicting mortality, the PSI score showed the highest accuracy in predicting mortality (92% at a cutoff of >121). In comparison, CURB-65 had an accuracy of 88% at a cutoff of >2, severe frailty had a diagnostic accuracy of 90%, and the FI-Lab21 index had a 59.6% accuracy for predicting mortality with a cutoff value of >0.296.
This was in accordance with the findings by Zan et al. [9], who found that the diagnostic accuracy in predicting 30-day mortality was highest for PSI (AUC: 0.812), followed by FI-Lab21 (AUC: 0.783) and CURB-65 (AUC: 0.799, p<0.01). Similarly, Park et al. [18] found that PSI had the highest accuracy in predicting six-month mortality, followed by FI-Lab21 and CURB-65. The C-statistics for the PSI score was 0.71, for FI-Lab21 was 0.69, and for CURB-65 was 0.62. In contrast, Nascè et al. [17] did not find PSI or CURB-65 scores to be significant predictors of mortality. Rather, they found higher age, lower BMI, and scores assessing comorbidities and malnutrition to be important predictors of one-year mortality. Similarly, Baek et al. [19] found that the CURB-65 and PSI scores did not perform well in predicting outcomes for older patients with pneumonia, as the AUC for predicting mortality in pneumonia was 0.61 for the CURB-65 score and 0.52 for the PSI score. The reasons attributed were a higher proportion of comorbidities in the patients, more nursing home patients included who may have compromised immunity, different exposure to microbiological organisms, and outcome measures of only in-hospital mortality rather than 30-day mortality.
Overall, the scores remain useful for predicting mortality, and the PSI was found to be superior to others. This may be because the PSI has been developed using large datasets from diverse patient populations, which enhances its generalizability. However, it must be stressed that, while the PSI is effective in predicting outcomes, its comprehensive assessment often requires various diagnostic tests such as chest radiographs and arterial blood gas analysis. In resource-poor settings, obtaining these tests can be challenging, leading to potential limitations in using the PSI for prognostication in such contexts [9]. In those cases, other scores such as CURB-65 and FI may become handy, as they carry statistically comparable diagnostic accuracy to the PSI. A recent study by Zan et al. [9] has further shown that the FI-Lab21 score can be judiciously used by combining it with the PSI and CURB-65, which may increase its AUC from 0.812 to 0.85 and from 0.799 to 0.839, respectively.
Conclusions
To conclude, the PSI, along with CURB-65 and FI-Lab21, scores exhibited correlations with 30-day in-hospital mortality among elderly patients with CAP. The PSI score demonstrated better predictive ability than those of CURB-65 and FI-Lab21 in predicting mortality. It appears to be a simple, efficient, easily accessible, and objective tool that can assist clinicians in promptly stratifying older CAP patients. Identifying the risk of mortality in elderly patients with CAP early upon admission would enable clinicians to intervene promptly during the hospital stay. This can help prevent functional decline and allow for the development of a suitable rehabilitation plan to restore function after discharge.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Identifying strategies for dealing with the aging population from the perspective of health system experts: a qualitative study J Educ Health Promot Samouei R Keyvanara M 2101120223600323310.4103/jehp.jehp_1213_21PMC 9393960 · doi ↗ · pubmed ↗
- 2Perspectives on aging and quality of life Healthcare (Basel) Noto S 21311120233757037210.3390/healthcare 11152131 PMC 10418952 · doi ↗ · pubmed ↗
- 3The trend of population aging and planning of health services for the elderly: a review study J Torbat Heydariyeh Univ Med Sci Khodamoradi A Hassanipour S Khotbesara RD Ahmadi B 819562018 https://jms.thums.ac.ir/article-1-544-en.html
- 4The relative burden of community-acquired pneumonia hospitalizations in older adults: a retrospective observational study in the United States BMC Geriatr Brown JD Harnett J Chambers R Sato R 921820182966113510.1186/s 12877-018-0787-2PMC 5902892 · doi ↗ · pubmed ↗
- 5A study of community-acquired pneumonias in elderly individuals in Bijapur, India Int Schol Res Notices Abdullah BB Zoheb M Ashraf SM Ali S Nausheen N 92012
- 6Comparison of clinical characteristics and performance of pneumonia severity score and CURB-65 among younger adults, elderly and very old subjects Thorax Chen JH Chang SS Liu JJ 9719776520102096593410.1136/thx.2009.129627 · doi ↗ · pubmed ↗
- 7The prognostic performance of q SOFA for community-acquired pneumonia J Intensive Care Tokioka F Okamoto H Yamazaki A Itou A Ishida T 46620183011653210.1186/s 40560-018-0307-7PMC 6083584 · doi ↗ · pubmed ↗
- 8Community-acquired pneumonia in critically ill very old patients: a growing problem Eur Respir Rev Cillóniz C DominedòC Pericàs JM Rodriguez-Hurtado D Torres A 1901262920203207585810.1183/16000617.0126-2019 PMC 9488936 · doi ↗ · pubmed ↗