A Superior Squeeze: Superior Vena Cava Syndrome Secondary to Small Cell Lung Cancer
Anvit D Reddy, Oshin Rai, Natalie Shaykh, Falguni Patel, Niyati Patel, Ghania Masri

TL;DR
A 59-year-old woman with facial and arm swelling was found to have a severe case of superior vena cava syndrome caused by undiagnosed small cell lung cancer.
Contribution
This case report highlights a rare and severe presentation of SVC syndrome due to previously undetected small cell lung cancer.
Findings
A right suprahilar mass was found to compress the SVC and a branch of the right pulmonary artery.
Immunostaining confirmed the mass to be small cell lung cancer.
The patient had bilateral pulmonary emboli in addition to SVC compression.
Abstract
Superior vena cava (SVC) syndrome is an uncommon yet potentially fatal syndrome occurring after intrinsic or extrinsic compression to the SVC. While there are multiple emerging etiologies for this phenomenon, malignancy remains the most common. It is characterized by several symptoms including facial swelling, extremity swelling, shortness of breath, and headaches. We present the case of a 59-year-old female with a past medical history of cocaine abuse who was admitted for upper extremity swelling and facial edema. Imaging revealed a right suprahilar mass compressing a branch of the right pulmonary artery and SVC, in addition to bilateral segmental and subsegmental pulmonary emboli. She underwent an emergent biopsy and SVC stenting, with immunostaining revealing small cell lung cancer (SCLC). This case highlights a severe presentation of SVC syndrome caused by previously undetected SCLC.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2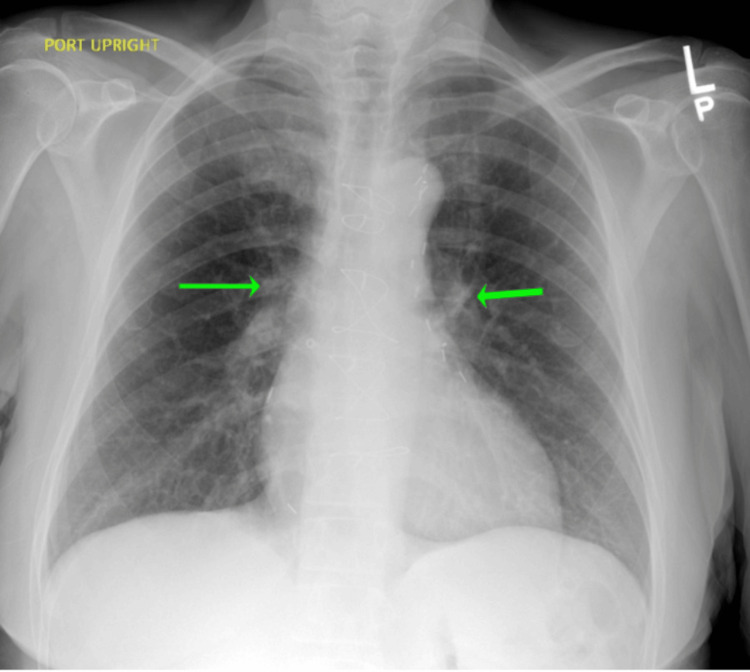 Figure 3
Figure 3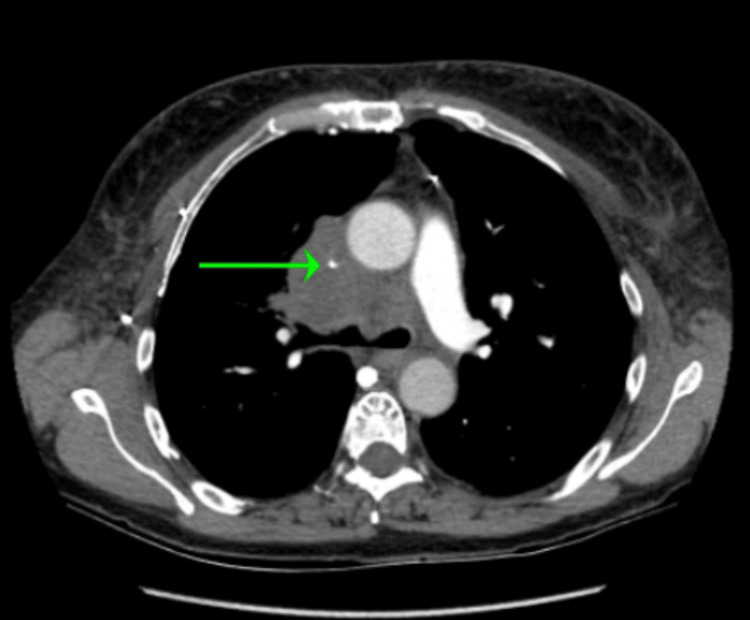 Figure 4
Figure 4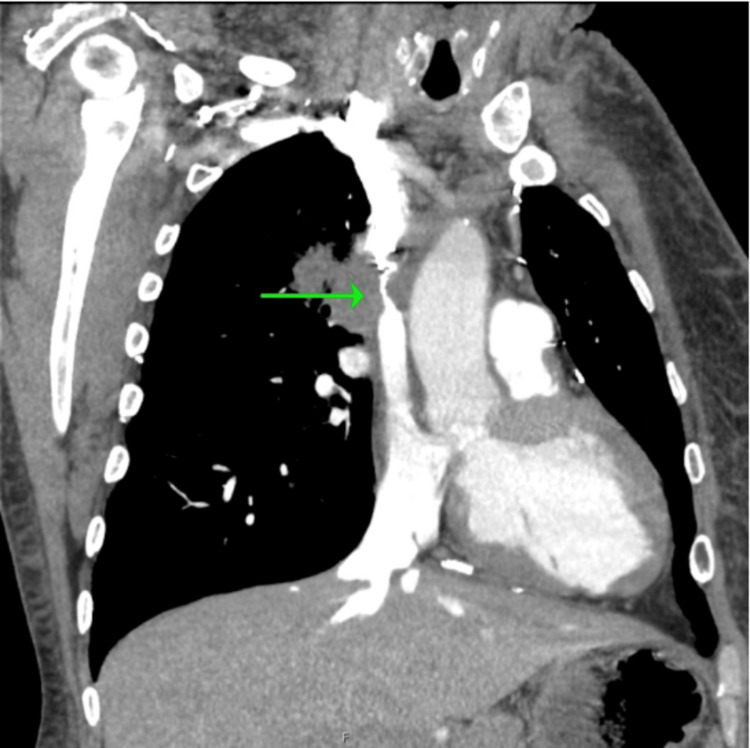 Figure 5
Figure 5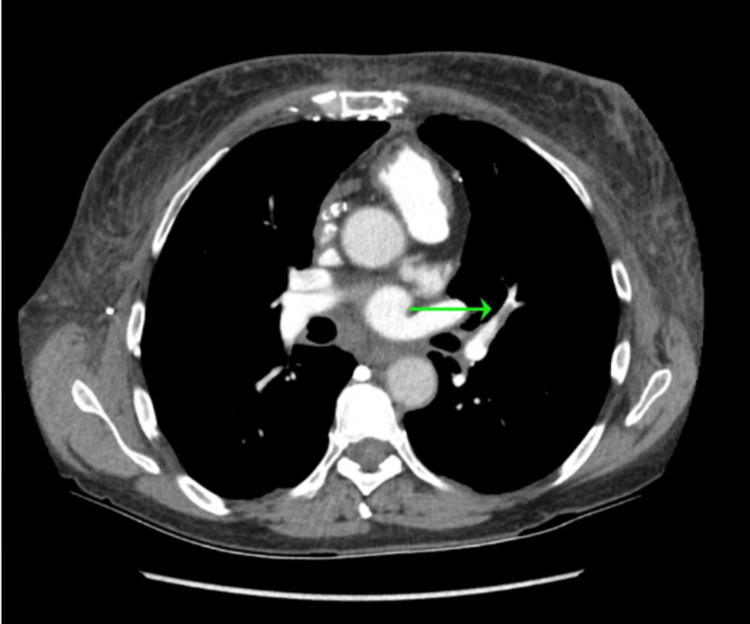 Figure 6
Figure 6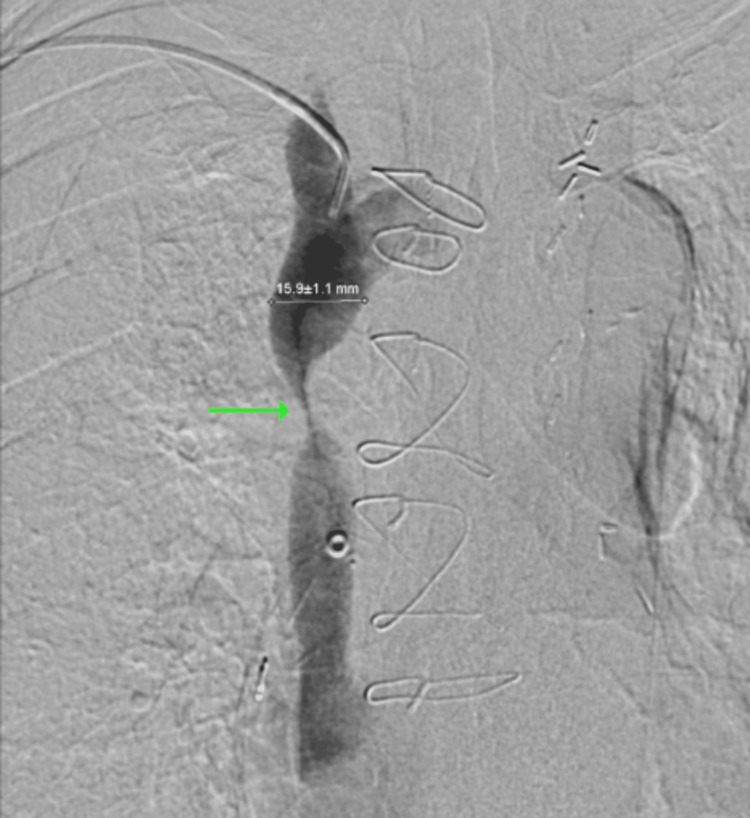 Figure 7
Figure 7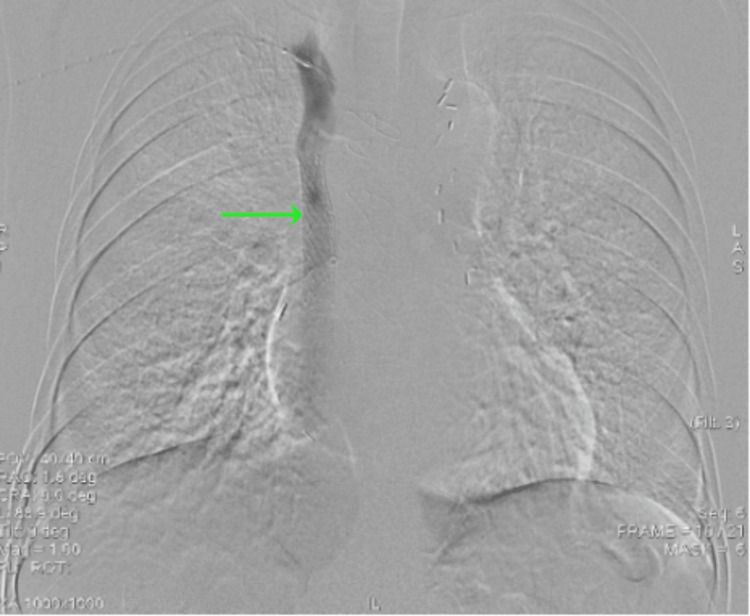 Figure 8
Figure 8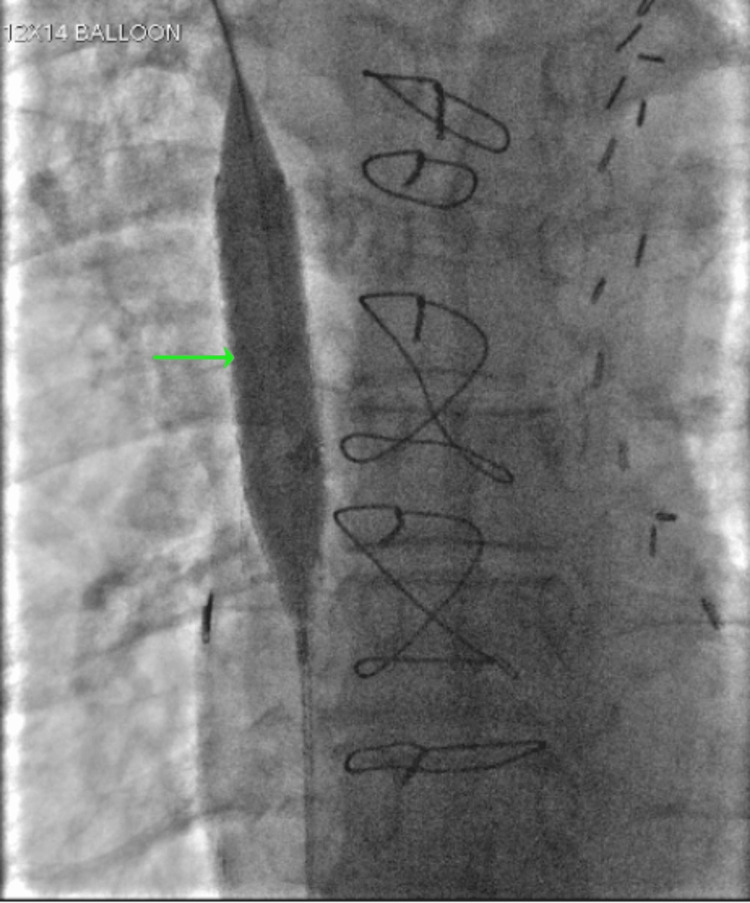 Figure 9
Figure 9Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac tumors and thrombi · Central Venous Catheters and Hemodialysis · Venous Thromboembolism Diagnosis and Management
Introduction
Superior vena cava (SVC) syndrome is an uncommon condition with about 15,000 cases in the United States per year [1]. It is the result of partial or complete obstruction of blood flow returning to the SVC and can be life-threatening with significant morbidity and mortality. The SVC is a thin-walled, low-pressure system that can be compressed intrinsically and extrinsically in the middle or anterior mediastinum. Although the most common cause used to be infectious, such as syphilitic aortic aneurysm and tuberculosis, malignancy is now responsible for more than 90% of cases [2]. The most common malignancy is non-small cell lung cancer (NSCLC) (50%), followed by small cell lung cancer (SCLC) (25%) and lymphomas (10%). Benign causes are rising with intrinsic etiologies of SVC syndrome including thrombi, stenosis, and fibrosis from medical devices such as indwelling catheters and pacemaker leads, hypercoagulable states, or vasculitis [3,4].
Case presentation
A 59-year-old female with a past medical history of diabetes mellitus, coronary artery bypass graft, and cocaine abuse presented to the emergency department (ED) with worsening headaches, shortness of breath, and upper and lower extremity swelling over the past two weeks.
On presentation, her blood pressure was 156/68 mmHg, heart rate was 58 beats per minute, temperature was 98.0 degrees Fahrenheit, and respiratory rate was 19 breaths per minute with an oxygen saturation of 98% on room air. A physical exam revealed an anxious-appearing female with diffuse facial swelling and bilateral upper extremity swelling (see Figure 1 and Figure 2).
Notable asymmetric facial edema, left more than right, as well as a saddle nose
Upper extremity edema, left more than right
Laboratory evaluation was largely unremarkable, with electrolytes, hemoglobin, and leukocytes within normal limits. A chest X-ray (CXR) radiography noted a central prominence of pulmonary vessels but was otherwise unremarkable (see Figure 3). A computed tomography pulmonary angiography (CTPA) revealed a right suprahilar mass measuring approximately 5.2 cm × 5.1 cm with severe compression of the right upper lobe pulmonary artery branch and severe short segment narrowing of the SVC (see Figure 4 and Figure 5). It also showed left upper and lower lobe segmental and subsegmental pulmonary emboli without right heart strain (see Figure 6).
Chest radiograph anterior-posterior view showing no evidence of pulmonary infiltrates, pleural effusions, or pneumothorax. The heart size is in the upper limits of normal with evidence of previous cardiac surgery. There is prominence of central pulmonary vessels
CTPA (axial view) showing severe narrowing of the SVC from compression by the right suprahilar massCTPA: computed tomography pulmonary angiography; SVC: superior vena cava
CTPA (coronal view) showing severe short segment narrowing of the SVC from compression by the right suprahilar massCTPA: computed tomography pulmonary angiography; SVC: superior vena cava
CTPA (axial view) showing subsegmental pulmonary emboliCTPA: computed tomography pulmonary angiography
A heparin drip was subsequently started and interventional radiology was consulted for further management. An initial venogram demonstrated severe SVC stenosis related to the infiltrating right suprahilar mass (see Figure 7), so an intravascular biopsy of the mass using the HawkOne system was obtained for pathology review. Afterward, a 12 mm × 6 cm Abre stent was placed across the SVC stenosis below the level of brachiocephalic vein confluence and its distal portion at the cavoatrial junction (see Figure 8). This was followed by an in-stent venoplasty with 12 mm and 14 mm balloons (see Figure 9). An immunostain of the mass revealed positive synaptophysin, chromogranin, CD56, TTF1, and BCL-2 which was consistent with SCLC. The patient was transitioned to a direct oral anticoagulant and was discharged with near full resolution of her symptoms with plans for oncology follow-up outpatient.
Venogram demonstrating SVC stenosisSVC: superior vena cava
Venogram demonstrating the self-expandable Abre stent
Venogram demonstrating the in-stent venoplasty with balloon
Discussion
SVC syndrome is diagnosed by clinical symptoms and advanced imaging. While malignancy is the most common cause, it is important to note that with more therapies requiring catheters ending in the right atrium, the incidence of nonmalignant causes is rising [4,5]. When obtaining a history from patients with common symptoms, screening for a history of malignancy and intravascular procedures is crucial [2]. Patients present with progressive symptoms, usually over several weeks, such as facial swelling, upper extremity swelling, distended neck veins, dyspnea, cough, and headaches [2,4,6]. In severe cases, confusion, visual changes, syncope, and coma can occur [4]. SVC syndrome that develops chronically can present with dilated tributary veins seen on physical exam [4].
Yu et al. proposed a grading scale based on clinical presentation, with grades ranging from 0 for asymptomatic to 5 for death [5]. Imaging with CXR is nonspecific and can show mediastinal widening and vascular engorgement. CT scans, such as the CTPA utilized in this patient, help characterize and localize the etiology of SVC obstruction. Venography is considered the gold standard for the diagnosis of SVC syndrome as collateral pathways are better visualized which helps guide management [4,7]. Compared to Yu et al., the Stanford method focuses on the anatomical obstruction visualized by venography and consists of four different types [4]. Its focus was to identify the patients at fatal risk of airway compromise who may need urgent intervention, but with patients having progressive symptoms, it is not as applicable [4]. The severity of presenting symptoms can guide therapy, along with the anatomic obstruction, but there is not yet an integrated classification that combines both [4] to further risk-stratify patients.
Initial management focuses on reducing symptoms with supplemental oxygen and stabilization of the airway. Elevating the head of the bed aims to reduce edema and decrease hydrostatic pressure [4]. Treatment is based on severity. If symptoms are not life-threatening and mass effect is suspected, patients can undergo tissue biopsy with staging evaluation to tailor chemotherapy with or without radiation [8]. However, if patients are at risk of circulatory compromise, they may require endovascular therapy including angioplasty, stenting, surgical bypass, and even SVC reconstruction [2,4]. In the case of our patient, she was a grade 1 or mild for edema in the head and neck based on Yu et al.'s symptom grading scale [9]; however, with the Stanford method, she was a type B with more than 90% stenosis prompting more urgent intervention [10]. The advantage of percutaneous stent placement is that it allows for symptomatic relief and an opportunity for interventional radiology to obtain a tissue biopsy. Obstruction due to intrinsic causes, such as thrombosis secondary to indwelling catheters, requires the removal of devices and consideration of anticoagulation [2,4].
Notably, this patient had presented to the ED one year before this admission for a chief complaint of chest pain, where a CTPA was performed and did not reveal any pulmonary emboli, lung mass, or lymphadenopathy. This aligns with the presentation of SCLC, which is known to be a rapidly growing malignancy with a doubling time estimated between 25 and 217 days [11]. This rapid growth poses a challenge for screening as SCLC is more often discovered past early, curative stages. It is important to note that our patient's CTPA was less sensitive than the CT of the chest for detecting lung cancer. A retrospective study done by Kino et al. showed that the rate of detection for lung cancer in patients presenting to the ED with pulmonary embolism through CTPA was low at 0.47% [12]. Therefore, the emphasis remains on guideline-directed screening through high-resolution CT for those with a smoking history [13].
Conclusions
SVC syndrome is uncommon and should be diagnosed through careful history-taking, physical examination, and imaging. Since malignancy is the most common inciting event, clinicians should maintain a high index of suspicion when encountering patients with a history and symptoms consistent with SVC syndrome. Addressing the underlying cause is the mainstay of management, but more severe presentations may prompt endovascular therapy. Treatment should include a multidisciplinary team that may include internal medicine, radiology, surgery, and oncology.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Superior vena cava syndrome Stat Pearls Seligson M Surowiec S Treasure Island (FL)Stat Pearls Publishing 2022 https://pubmed.ncbi.nlm.nih.gov/28723010/28723010 · pubmed ↗
- 2Superior vena cava syndrome JACC Cardiovasc Interv Azizi AH Shafi I Shah N Rosenfield K Schainfeld R Sista A Bashir R 289629101320203335752810.1016/j.jcin.2020.08.038 · doi ↗ · pubmed ↗
- 3Superior vena cava syndrome with malignant causes N Engl J Med Wilson LD Detterbeck FC Yahalom J 1862186935620071747601210.1056/NEJ Mcp 067190 · doi ↗ · pubmed ↗
- 4The superior vena cava syndrome: clinical characteristics and evolving etiology Medicine (Baltimore) Rice TW Rodriguez RM Light RW 37428520061652305110.1097/01.md.0000198474.99876.f 0 · doi ↗ · pubmed ↗
- 5Superior vena cava syndrome from extensive lung cancer J Osteopath Med Prasad R Kemnic T 32933012120213363596210.1515/jom-2020-0304 · doi ↗ · pubmed ↗
- 6Rapid fire: superior vena cava syndrome Emerg Med Clin North Am Zimmerman S Davis M 5775843620183003744410.1016/j.emc.2018.04.011 · doi ↗ · pubmed ↗
- 7Interventions for superior vena cava syndrome J Cardiovasc Surg (Torino) Sen I Kalra M Gloviczki P 67468163202210.23736/S 0021-9509.22.12448-136469045 · doi ↗ · pubmed ↗
- 8Screening for lung cancer: US Preventive Services Task Force recommendation statement JAMA Krist AH Davidson KW Mangione CM 96297032520213368747010.1001/jama.2021.1117 · doi ↗ · pubmed ↗