Comparison of Intercostal and Subxiphoid Left Pleural Drain After Coronary Artery Bypass Grafting (CABG) Surgery: A Systematic Review and Meta-Analysis
Pranay Mehsare, Nitinkumar Borkar, Nitin Kumar Kashyap, Gaind Saurabh, Nirupam Chakraborty

TL;DR
This study compares two methods for inserting chest drains after heart surgery, finding that one method reduces pain and improves breathing outcomes.
Contribution
The paper provides a meta-analysis comparing subxiphoid and intercostal drain insertion outcomes after CABG surgery.
Findings
Subxiphoid drains reduced postoperative ventilation time and pain scores compared to intercostal drains.
Subxiphoid drains improved vital capacity, forced vital capacity, and oxygen levels in arterial blood gas analysis.
The findings suggest subxiphoid drain placement is more beneficial for pulmonary function recovery.
Abstract
Coronary artery bypass grafting (CABG), a prevalent surgery for coronary artery disease, often involves left internal mammary artery harvesting, necessitating left pleural drain insertion. This can lead to pain, discomfort, and respiratory issues. This analysis compares outcomes between subxiphoid and intercostal left pleural drain insertion. Following the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines, this systematic review and meta-analysis involved searches in MEDLINE, Cochrane Central Register of Controlled Trials (CENTRAL), Scopus, Google Scholar, and Clinical Trial Registry. Studies were selected based on primary outcomes (postoperative ventilator support duration and pain score) and secondary outcomes (percentage predicted vital capacity (VC), forced VC (FVC), and partial pressure of oxygen (PO2) in arterial blood gas (ABG) analysis).…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
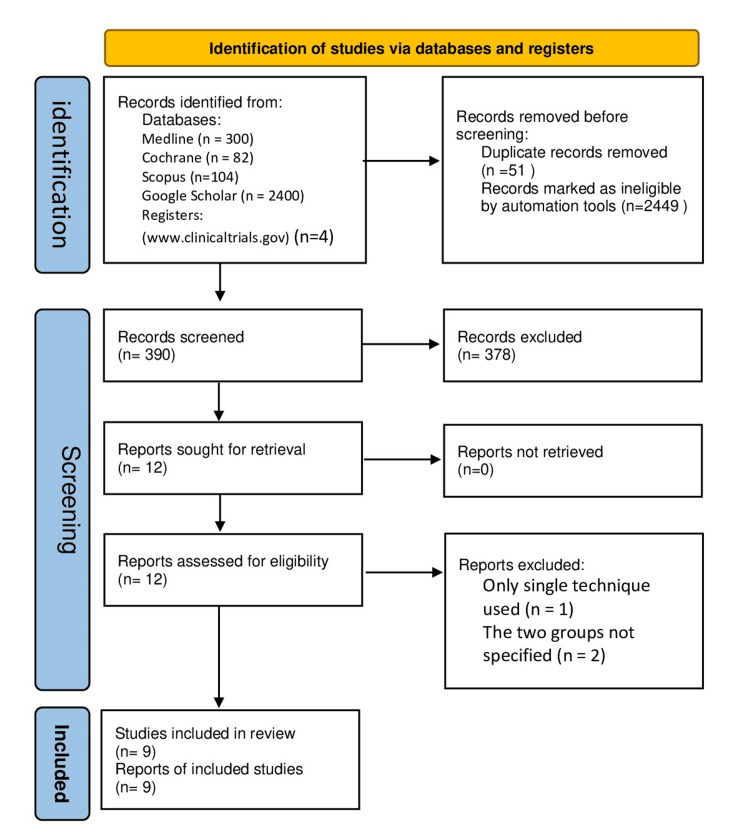 Figure 1
Figure 1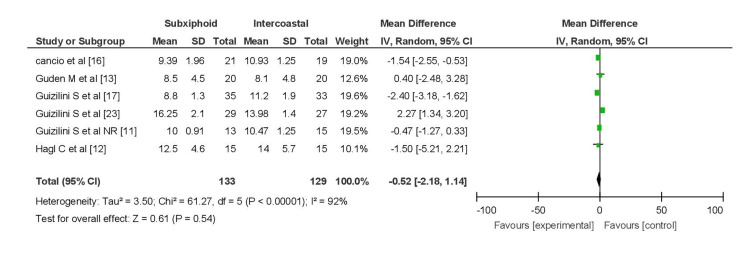 Figure 2
Figure 2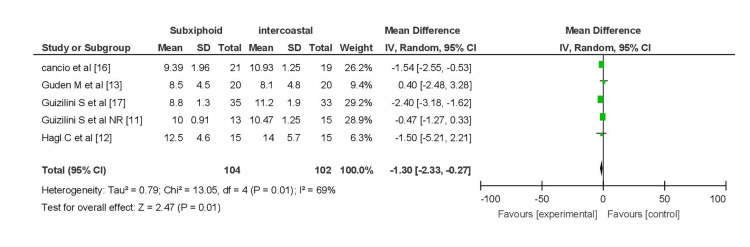 Figure 3
Figure 3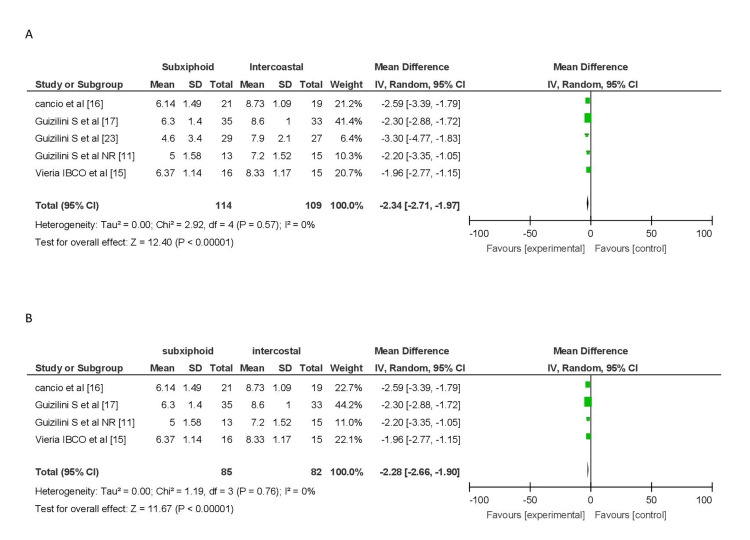 Figure 4
Figure 4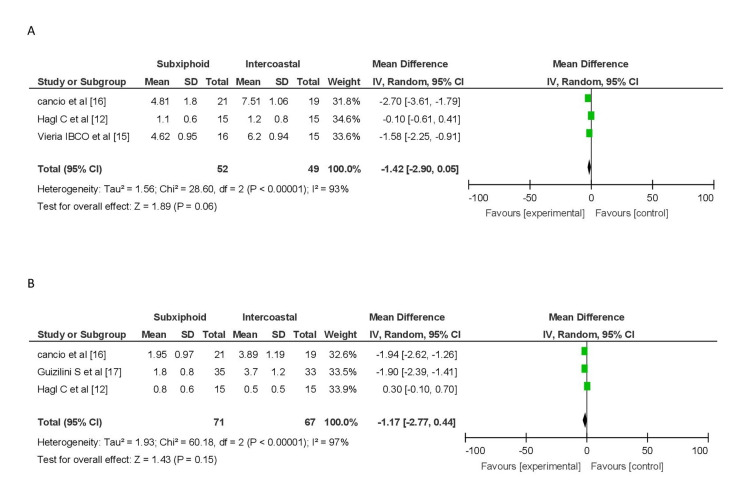 Figure 5
Figure 5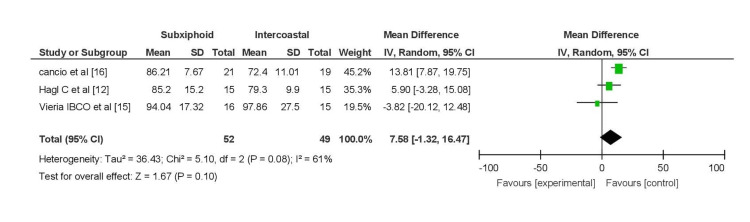 Figure 6
Figure 6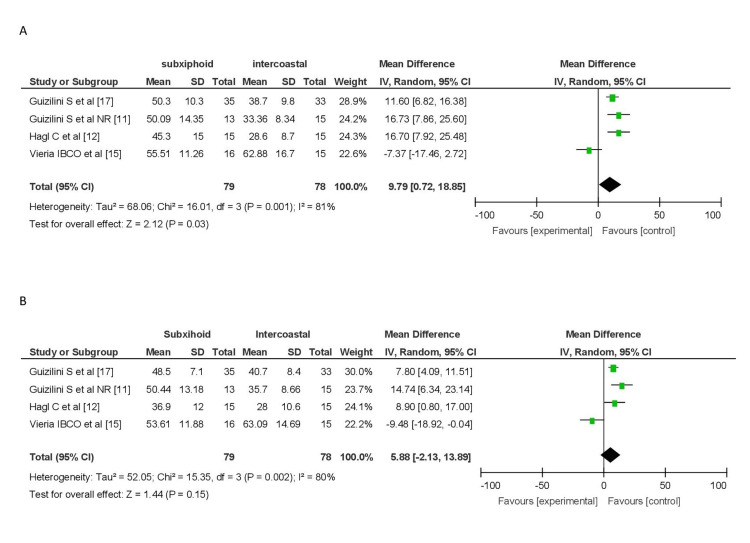 Figure 7
Figure 7| Serial number | Studies | Setting | Study period | Design | Number of patients (N) | Mean age (years) | Pulmonary function assessment | Outcome |
| 1 |
Hagl et al. [ | Hannover Medical School, Hannover, Germany | 1999 | RCT | Total (N) = 30 | NA | First, third, and fifth day | The subxiphoid drain better preserves lung function compared to the intercostal drain. |
| Group 1 (subxiphoid) = 15 | 57.8 + 11.2 years | |||||||
| Group 2 (intercostal) = 15 | 60.7 + 9.4 years | |||||||
| 2 |
Ozelami Vieira et al. [ | Hospital de Clínicas da Faculdade de Medicina da Universidade do Triângulo Mineiro, Uberaba, Minas Gerais, Brazil | January 2010 to July 2011 | RCT | Total (N) = 31 | NA | First, second, and third day | The subxiphoid drain better preserves lung function. |
| Group 1 (subxiphoid) = 16 | 56.43 ± 9.04 years | |||||||
| Group 2 (intercostal) = 15 | 59.20 ± 8.4 years | |||||||
| 3 |
Guden et al. [ | Akif Ersoy Thoracic & Cardiovascular Surgery Education & Research Hospital, Istanbul, Turkey | December 2010 | RCT | Total (N) = 40 | NA | Before extubation and one, three, six, 12, 18, 24, and 48 hours after extubation | Subxiphoid and intercostal both have similar clinical outcomes. |
| Group 1 (subxiphoid) = 20 | 57.3 + 11.6 years | |||||||
| Group 2 (intercostal) = 20 | 55.7 + 10.4 years | |||||||
| 4 |
Cancio et al. [ | Federal University of São Paulo, São Paulo, São Paulo, Brazil | 2012 | RCT | Total (N) = 40 | NA | First, third, and fifth day | Subxiphoid drain better preserves lung function. |
| Group 1 (intercostal) = 19 | 57.37 ± 10.83 years | |||||||
| Group 2 (subxiphoid) = 21 | 53.86 ± 10.30 years | |||||||
| 5 |
Guizilini et al. [ | Federal University of São Paulo, São Paulo, São Paulo, Brazil | 2014 | RCT | Total (N) = 68 | NA | First and fifth day | Subxiphoid drain better preserves lung function. |
| Group 1 (intercostal) = 33 | 57.0 ± 7.7 years | |||||||
| Group 2 (subxiphoid) = 35 | 59.6 ± 8.4 years | |||||||
| 6 |
Simon et al. [ | Fundação Universitária de Cardiologia, Porto Alegre, Rio Grande do Sul, Brazil | July 2014 to August 2015 | RCT | Total (N) = 48 | NA | First, third, and before discharge | There was no difference in maximal respiratory pressures. |
| Group 1 (intercostal) = 24 | 65.58 ± 9.50 years | |||||||
| Group 2 (subxiphoid) = 2 4 | 61.75 ± 9.58 years | |||||||
| 7 |
Guizilini et al. [ | São Paulo Hospital, Escola Paulista de Medicina, Federal University of São Paulo, São Paulo, São Paulo, Brazil. | December 2007 and March 2012 | RCT | Total (N) = 56 | NA | First, third, and fifth postoperative day | Subxiphoid pleural drain has better preservation and recovery of pulmonary capacity and volume. |
| Group 1 (intercostal) = 27 | 59.22 ± 11.73 years | |||||||
| Group 2 (subxiphoid) = 29 | 56.66 ± 10.33 years | |||||||
| 8 |
Guizilini et al. [ | Federal University of São Paulo | 2004 | Retrospective cohort study | Total (N) = 28 | 57.49 ± 8.40 years | First, third, and fifth day | The subxiphoid technique of drain insertion has demonstrated better preservation of lung function compared to the intercostal drain site. |
| Group 1 (intercostal) = 15 | 57.53 ± 10.29 years | |||||||
| Group 2 (subxiphoid) = 13 | 57.46 ± 5.94 years | |||||||
| 9 |
Elnasr et al. [ | Cardiothoracic Surgery Department, Tanta University, Egypt | 2017 | Retrospective cohort study | Total (N) = 71 | NA | Preoperative, one-hour post-extubation, on the third post-extubation day, and predischarge | Subxiphoid and intercostal both have similar clinical outcomes. Analgesia is a requirement for patients with intercostal pleural drainage. |
| Group 1 (intercostal) = 38 | 55.9 ± 8.6 years | |||||||
| Group 2 (subxiphoid) = 33 | 54 ± 7.9 years |
| Serial number | Studies | Patients (N) | Time of intubation/mechanical ventilation (hours) | PRE-OP | POD 1 | POD 2 | POD 3 | POD 5 | Outcome | |
| 1 |
Hagl et al. [ | Group 1 (subxiphoid) = 15 | 12.5 + 4.6 hours | VC (L/MIN) | 3.7 ± 0.7 (L/MIN) | 1.9 ± 1.0 (L/MIN) | NA | 1.8 ± 0.6 (L/MIN) | 2.2 ± 0.5 (L/MIN) | Inserting the suxiphoid pleural drain results in significantly less impairment of pulmonary function and subjective pain compared to intercostal insertion. |
| % predicted VC | 92.3 ± 30.6 (% PRED VC) | 45.3 ± 15.00 (% PRED VC) | NA | 44.5 ± 15.1 (% PRED VC) | 56.9 ± 12.6 (% PRED VC) | |||||
| FEV (L/MIN) | 2.8 ± 0.7 (L/MIN) | 1.2 ± 0.4 (L/MIN) | NA | 1.4 ± 0.4 (L/MIN) | 1.6 ± 0.5 (L/MIN) | |||||
| % predicted FEV | 86.2 ± 18.2 (% PRED FEV) | 36.9 ± 12.0 (% PRED FEV) | NA | 42.0 ± 12.1 (% PRED FEV) | 50.8 ± 12.1 (% PRED FEV) | |||||
| PO2 (mmHg) | 84.4 ± 8.8 (mmHg) | 85.2 ± 15.2 (mmHg) | NA | 89.4 ± 10.5 (mmHg) | 79.7 ± 9.1 (mmHg) | |||||
| PCO2 (mmHg) | 39.3 ± 7.4 (mmHg) | 42.2 ± 6.5 (mmHg) | NA | 39.0 ± 2.4 (mmHg) | 41.6 ± 5.4 (mmHg) | |||||
| Pain score (0-10) | NA | NA | NA | Pain score at rest = 1.1 + 0.6 | Pain score at rest = 0.8 + 0.6 | |||||
| Pain score on forced inspiration = 1.5 + 0.8 | Pain score on forced inspiration = 1.1 + 0.5 | |||||||||
| Group 2 (intercostal) = 15 | 14.0 ± 5.7 hours | VC (L/MIN) | 3.6 ± 0.9 (L/MIN) | 1.2 ± 0.4 (L/MIN) | NA | 1.7 ± 0.7 (L/MIN) | 2.3 ± 0.6 (L/MIN) | |||
| % predicted VC | 88.0 ± 18.2 (% PRED VC) | 28.6 ± 8.7 (% PRED VC) | NA | 42.2 ± 17.6 (% PRED VC) | 55.5 ± 14.8 (% PRED VC) | |||||
| FEV (L/MIN) | 3.3 ± 1.0 (L/MIN) | 1.2 ± 0.7 (L/MIN) | NA | 1.8 ± 1.0 (L/MIN) | 2.5 ± 1.6 (L/MIN) | |||||
| % predicted FEV | 83.5 ± 16.4 (% PRED FEV) | 28.0 ± 10.6 (% PRED FEV) | NA | 40.6 ± 14.5 (% PRED FEV) | 53.9 ± 12.5 (% PRED FEV) | |||||
| PO2 (mmHg) | 81.9 ± 9.1 (mmHg) | 79.3 ± 9.9 (mmHg) | NA | 88.1 ± 7.8 (mmHg) | 84.1 ± 7.4 (mmHg) | |||||
| PCO2 (mmHg) | 42.3 ± 11.2 (mmHg) | 39.0 ± 6.5 (mmHg) | NA | 41.1 ± 5.6 (mmHg) | 38.3 ± 6.0 (mmHg) | |||||
| Pain score (0-10) | NA | NA | NA | Pain score at rest = 1.2 + 0.8 | Pain score at rest = 0.5 + 0.5 | |||||
| Pain score on forced inspiration = 1.3 + 0.7 | Pain score on forced inspiration = 0.8 + 0.4 | |||||||||
| 2 |
Ozelami Vieira et al. [ | Group 1 (subxiphoid) = 16 | VC (L/MIN) | 3.25 ± 0.65 (L/MIN) | 2.26 ± 0.58 (L/MIN) | NA | 2.00 ± 0.55 (L/MIN) | NA | Inserting the drain in the subxiphoid region causes minimal change in lung function and discomfort, leading to improved recovery of respiratory parameters. | |
| % predicted VC | 86.58 ± 7.51 (% PRED VC) | 55.51 ± 11.26 (% PRED VC) | NA | 47.93 ± 11.93 (% PRED VC) | NA | |||||
| FEV (L/MIN) | 2.60 ± 0.49 (L/MIN) | 1.73 ± 0.44 (L/MIN) | NA | 1.56 ± 0.41 (L/MIN) | NA | |||||
| % predicted FEV | 87.50 ± 7.45 (% PRED FEV) | 53.61 ± 11.88 (% PRED FEV) | NA | 47.57 ± 11.13 (% PRED FEV) | NA | |||||
| PO2 (mmHg) | 82.93 ± 9.89 (mmHg) | 94.04 ± 17.32 (mmHg) | 96.20 ± 15.04 (mmHg) | NA | NA | |||||
| Pain score (0-10) | NA | Pain score at rest = 6.37 ± 1.14 | Pain score at rest = 5.62 ± 1.02 | Pain score at rest = 4.62 ± 0.95 | NA | |||||
| Pain score on forced expiratory effort = 7.68 ± 1.19 | Pain score on forced expiratory effort = 6.68 ± 0.87 | Pain score on forced expiratory effort = 5.37 ± 1.08 | ||||||||
| Group 2 (intercostal) = 15 | VC (L/MIN) | 3.12 ± 0.76 (L/MIN) | 2.32 ± 0.70 (L/MIN) | NA | 2.04 ± 0.56 (L/MIN) | NA | ||||
| % predicted VC | 88.23 ± 11.88 (% PRED VC) | 62.88 ± 16.70 (% PRED VC) | NA | 54.68 ± 14.53 (% PRED VC) | NA | |||||
| FEV (L/MIN) | 2.54 ± 0.61 (L/MIN) | 1.82 ± 0.53 (L/MIN) | NA | 1.64 ± 0.48 (L/MIN) | NA | |||||
| % predicted VC | 91.19 ± 11.91 (% PRED VC) | 63.09 ± 14.69 (% PRED VC) | NA | 56.99 ± 13.92 (% PRED VC) | NA | |||||
| PO2 (mmHg) | 81.93 ± 10.65 (mmHg) | 97.86 ± 27.50 (mmHg) | NA | NA | NA | |||||
| Pain score (1-10) | NA | Pain score at rest = 8.33 ± 1.17 | Pain score at rest = 7.60 ± 1.05 | Pain score at rest = 6.20 ± 0.94 | NA | |||||
| Pain score on forced expiratory effort = 9.06 ± 0.88 | Pain score on forced expiratory effort = 8.86 ± 1.12 | Pain score on forced expiratory effort = 7.00 ± 1.13 | ||||||||
| 3 |
Guden et al. [ | Group 1 (subxiphoid) = 20 | 8.8 ± 4.5 hours | PO2, mmHg | NA | 111 (5.76) (mmHg) | 105 (4.41) (mmHg) | NA | NA | Both the subxiphoid and intercostal approaches for chest tube placement resulted in comparable clinical outcomes. |
| PCO2, mmHg | NA | 38 (0.59) (mmHg) | 39 (0.69) (mmHg) | NA | NA | |||||
| O2 saturation (%) | NA | 96 (0.37) % | 97 (0.49) % | NA | NA | |||||
| Group 2 (intercostal) = 20 | 8.1 ± 4.8 hours | PO2, (mmHg) | NA | 111 (5.3) (mmHg) | 106 (4.87) (mmHg) | NA | NA | |||
| PCO2, (mmHg) | NA | 37 (0.5) (mmHg) | 38 (0.65) (mmHg) | NA | NA | |||||
| O2 saturation | NA | 94 (0.49) % | 97 (0.52) % | NA | NA | |||||
| 4 |
Cancio et al. [ | Group 1 (intercostal) = 19 | 10.93 ± 1.25 hours | MIP (CM H2O) | 76.89 ± 21.15 (CM H2O) | 39.58 ± 12.92 (CM H2O) | NA | 44.62 ± 10.89 (CM H2O) | 53.09 ± 9.84* (CM H2O) | Patients who underwent subxiphoid pleural drainage demonstrated less decrease in respiratory muscle strength, better preservation of blood oxygenation, and reduced thoracic pain compared to those with intercostal drains in early postoperative OPCAB cases. |
| MEP (CM H2O) | 93.89 ± 24.70 (CM H2O) | 49.89 ± 11.02 (CM H2O) | NA | 59.57 ± 9.08 (CM H2O) | 66.88 ± 10.90 (CM H2O) | |||||
| PO2 (mmHg) | 81.33 ± 9.80 (mmHg) | 72.40 ± 11.01 (mmHg) | NA | NA | NA | |||||
| pCO2 (mmHg) | 37.40 ± 3.35 (mmHg) | 47.73 ± 8.68 (mmHg) | NA | NA | NA | |||||
| Pain score (0-10) | Pain score = 8.73 ± 1.09 | NA | Pain score = 7.15 ± 1.06 | Pain score = 3.89 ± 1.19 | ||||||
| Group 2 (subxiphoid) = 21 | 9.39 ± 1.96 hours | MIP (CM H2O) | 81.25 ± 26.49 (CM H2O) | 49.96 ± 12.05 (CM H2O) | NA | 56.68 ± 16.07 (CM H2O) | 67.29 ± 15.62 (CM H2O) | |||
| MEP (CM H2O) | 93.00 ± 30.00 (CM H2O) | 61.49 ± 12.07 (CM H2O) | NA | 69.59 ± 12.01 (CM H2O) | 78.23 ± 12.98 (CM H2O) | |||||
| PO2 (mmHg) | 77.67 ± 8.19 (mmHg) | 86.21 ± 7.67 (mmHg) | NA | NA | NA | |||||
| pCO2 (mmHg) | 38.00 ± 2.94 (mmHg) | 39.77 ± 4.02 (mmHg) | NA | NA | NA | |||||
| Pain score (0-10) | NA | Pain score = 6.14 ± 1.49 | NA | Pain score = 4.81 ± 1.80 | Pain score = 1.95 ± 0.97 | |||||
| 5 |
Guizilini et al. [ | Group 1 (intercostal) = 33 | 11.2 ± 1.9 hours | FVC (L/MIN) | 3.3 ± 0.4 (L/MIN) | NA | NA | NA | NA | Subxiphoid pleural drainage resulted in better functional capacity and exercise tolerance, along with a smaller pulmonary shunt fraction and improved clinical outcomes compared to intercostal pleural drainage following off-pump CABG. |
| % predicted FVC | 95.5 + 12.7 (% PRED FVC) | 38.7 ± 9.8 (of preop) (% PRED FVC) | NA | NA | 61.9 ± 7.2 (% PRED FVC) | |||||
| FEV (L/MIN) | 2.9 ± 0.3 (L/MIN) | NA | NA | NA | NA | |||||
| % predicted (FEV) | 101.1 + 11.8 (% PRED FEV) | 40.7 ± 8.4 (% PRED FEV) | NA | NA | 62.3 ± 5.8 (% PRED FEV) | |||||
| Pain score (0-10) | NA | Pain score = 8.6 ± 1.0 | NA | NA | Pain score = 3.7 ± 1.2 | |||||
| Group 2 (subxiphoid) = 35 | 8.8 ± 1.3 hours | FVC (L/MIN) | 3.5 ± 0.2 (L/MIN) | NA | NA | NA | NA | |||
| % predicted FVC | 91.5 + 9.4 (% PRED FVC) | 50.3 ± 10.3 (% PRED FVC) | NA | NA | 75.8 ± 8.6 (% PRED FVC) | |||||
| FEV (L/MIN) | 2.9 ± 0.2 (L/MIN) | NA | NA | NA | NA | |||||
| % predicted FEV | 97.9 + 7.8 (% PRED FEV) | 48.5 ± 7.1 (% PRED FEV) | NA | NA | 77.3 ± 8.4 (% PRED FEV) | |||||
| Pain score (0-10) | NA | Pain score = 6.3 ± 1.4 | NA | NA | Pain score = 1.8 ± 0.8 | |||||
| 6 |
Simon et al. [ | Group 1 (intercostal) = 24 | 24 (20 ± 27) hours | MIP (CM H2O) | 53.83 ± 22.71 (CM H2O) | NA | NA | NA | NA | There was no variation in maximal respiratory pressures concerning the insertion site of the pleural drain among patients who underwent CABG surgery with the use of ECC. |
| % predicted MIP | 58.93 + 24.91 (% PRED MIP) | NA | NA | NA | NA | |||||
| MEP (CM H2O) | 67.50 ± 25.02 (CM H2O) | NA | NA | NA | NA | |||||
| % predicted MEP | 38.69 + 14.13 (% PRED MEP) | NA | NA | NA | NA | |||||
| Pain score (0-10) | NA | Pain score = 2.96 | NA | Pain score = 1.39 | NA | |||||
| Group 2 (subxiphoid) = 24 | 24.5 (15 ± 44) hours | MIP (CM H2O) | 61.46 ± 24.58 (CM H2O) | NA | NA | NA | NA | |||
| % predicted MIP | 63.37 + 20.96 (% PRED MIP) | NA | NA | NA | NA | |||||
| MEP (CM H2O) | 73.75 ± 22.95 (CM H2O) | NA | NA | NA | NA | |||||
| % predicted MEP | 40.86 + 10.95 (% PRED MEP) | NA | NA | NA | NA | |||||
| Pain score (0-10) | Pain score = 3.54 | NA | Pain score = 1.89 | NA | ||||||
| 7 |
Guizilini et al. [ | Group 1 (intercostal) =27 | 13.98 ± 1.4 hours | FVC (L/MIN) | 3.27 ± 0.26 (L/MIN) | NA | NA | NA | NA | In severe COPD patients, subxiphoid pleural drainage resulted in better preservation and recovery of pulmonary capacity and volumes, with a lower pulmonary shunt fraction and improved clinical outcomes in early postoperative OPCAB. |
| % predicted FVC | 98.2 ± 21.70 (% PRED FVC) | NA | NA | NA | NA | |||||
| FEV1 (L/MIN) | 1.40 ± 0.35 (L/MIN) | NA | NA | NA | NA | |||||
| % predicted FEV1 | 40.32 ± 7.22 (% PRED FEV) | NA | NA | NA | NA | |||||
| Group 2 (subxiphoid) = 29 | 16.25 ± 2.1 hours | FVC (L/MIN) | 3.51 ± 0.45 (L/MIN) | NA | NA | NA | NA | |||
| % predicted FVC | 101.25 ± 25.24 (% PRED FVC) | NA | NA | NA | NA | |||||
| FEV1 (L/MIN) | 1.37 ± 0.22 (L/MIN) | NA | NA | NA | NA | |||||
| % predicted FEV | 38.21 ± 9.07 (% PRED FEV) | NA | NA | NA | NA | |||||
| 8 |
Guizilini et al. [ | Group 1 (intercostal) = 15 | 10.47 ± 1.25 hours | VC (L/MIN) | 3.69 ± 0.68 (L/MIN) | NA | NA | NA | NA | The subxiphoid technique of drain insertion has demonstrated better preservation of lung function compared to the intercostal drain site. |
| % predicted VC | 102.20 ± 16.64 (% PRED VC) | 33.36 ± 8.34 (% PRED VC) | NA | 45.42 ± 7.06 (% PRED VC) | 55.13 ± 8.30 (% PRED VC) | |||||
| FEV (L/MIN) | 2.86 ± 0.47 (L/MIN) | NA | NA | NA | NA | |||||
| % predicted FEV | 98.89 ± 14.40 (% PRED FEV) | 35.70 ± 8.66 (% PRED FEV) | NA | 48.04 ± 7.22 (% PRED FEV) | 58.80 ± 8.51% (% PRED FEV) | |||||
| PO2 (mmHg) | 74.40 ± 6.85 (mmHg) | NA | NA | NA | NA | |||||
| PCO2 (mmHg) | 38.27 ± 3.65 (mmHg) | NA | NA | NA | NA | |||||
| Group 2 (subxiphoid) = 13 | 10.00 ± 0.91 hours | VC (L/MIN) | 3.46 ± 1.16 (L/MIN) | NA | NA | NA | NA | |||
| % predicted VC | 96.05 ± 13.72 (% PRED VC) | 50.09 ± 14.35% (% PRED VC) | NA | 67.00 ± 15.88 (% PRED VC) | 78.22 ± 11.90% (% PRED VC) | |||||
| FEV (L/MIN) | 2.90 ± 0.97 (L/MIN) | NA | NA | NA | NA | |||||
| % predicted FEV | 99.16 ± 15.81 (% PRED FEV) | 50.44 ± 13.18 (% PRED FEV) | NA | 67.09 ± 15.12% (% PRED FEV) | 79.56 ± 11.52% (% PRED FEV) | |||||
| PO2 (mmHg) | 77.00 ± 6.75 (mmHg) | NA | NA | NA | NA | |||||
| PCO2 (mmHg) | 37.62 ± 4.03 (mmHg) | NA | NA | NA | NA | |||||
| 9 |
Elnasr et al. [ | Group 1 (intercostal) = 38 | 7 (6 ± 20) hours | PO2/FiO2 | 388.2 ± 38.9 | NA | NA | 299.95 ± 92.7 | NA | Both post-CABG approaches for pleural drains are effective without compromising pulmonary functions. However, patients with intercostal pleural drains require more analgesia. |
| Group 2 (subxiphoid) = 33 | 9 (6 ± 20) hours | PO2/FiO2 | 374.9 ± 38.6 | NA | NA | 334.8 ± 307.4 | NA |
| Study | Rater 1 | Rater 2 | Kappa |
|
Hagl et al. [ | 16 | 17 | 0.92 |
|
Ozelami Vieira et al. [ | 18 | 18 | NA |
|
Guden et al. [ | 18 | 17 | NA |
|
Cancio et al. [ | 16 | 16 | NA |
|
Guizilini et al. [ | 16 | 17 | NA |
|
Simon et al. [ | 17 | 17 | NA |
|
Guizilini et al. [ | 16 | 17 | NA |
|
Elnasr et al. [ | 11 | 12 | NA |
|
Guizilini et al. [ | 12 | 13 | NA |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac and Coronary Surgery Techniques · Cardiac, Anesthesia and Surgical Outcomes · Pleural and Pulmonary Diseases
Introduction and background
Coronary artery bypass grafting (CABG) surgery stands as the most frequently performed procedure by cardiac surgeons today [1]. A wide range of vascular conduits are available for CABG, with the primary options being the internal thoracic artery (ITA), saphenous vein, and radial artery [2].
After nearly four decades of coronary artery bypass surgery, ITA grafts have emerged as the superior conduit for revascularization. They demonstrate resistance to arteriosclerosis and offer exceptional long-term patency. Notably, employing the left ITA to revascularize the left anterior descending artery yields improved long-term survival and reduced cardiac events [3].
However, in the majority of cases, harvesting the left ITA pedicle necessitates opening the left pleural cavity, resulting in the need for drainage. CABG itself is associated with impaired pulmonary function in the postoperative phase, contributing to increased postoperative morbidity [4]. The pleurotomy required for this procedure, coupled with the presence of a pleural drain, adds to patient discomfort and negatively impacts respiratory mechanics [5,6].
These drains serve several purposes, including minimizing fluid accumulation in the pleural cavity, monitoring bleeding, and preventing potential complications such as pericardial effusion, hemothorax, and tamponade [7]. They are inserted either in the subxiphoid region or the intercostal space. The subxiphoid drain is directed toward the base of the left lung, while the intercostal drain is placed in the fifth or sixth intercostal space and directed toward the apex of the lung [8].
While essential, the presence of these drains can lead to alterations in pulmonary function, restricting the activity of respiratory muscles, modifying ventilatory mechanics, and causing intense pain and postoperative discomfort [8,9]. Several factors, such as general anesthesia, sternotomy, cardiopulmonary bypass, ITA grafts with pleurotomy, and pleural drain placement, can influence pulmonary function and clinical outcomes in CABG patients [10].
Recent evidence suggests that inserting the pleural drain in the subxiphoid position, rather than the intercostal space, minimizes chest wall trauma and preserves respiratory function during the early postoperative period [11,12]. Studies by Guden et al. [13] and Simon et al. [14] reported that clinical outcomes remain similar in both groups of patients. Hagl et al. [12], Ozelami Vieira et al. [15], Cancio et al. [16], Guizilini et al. [11,17] and Elnasr et al. [8] have reported positive outcomes associated with subxiphoid drain insertion, including reduced impairment of lung function, lower subjective pain, and improved recovery parameters.
This study systematically compares the outcomes of subxiphoid and intercostal pleural drain placements after CABG surgery.
Review
Materials and methods
This systematic review and meta-analysis followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines [18]. We initially conducted a literature search on PubMed and Google Scholar to ensure the absence of similar published meta-analyses.
A comprehensive and systematic search was then performed in electronic databases, including MEDLINE, Cochrane Central Register of Controlled Trials (CENTRAL), Scopus, and Google Scholar. The authors conducted this search independently and extended it up to December 31, 2023. Additionally, we searched the Clinical Trial Registry (ClinicalTrials.gov) and major conference proceedings up to the same date without imposing any language restrictions. We reran the searches before the final analysis to capture any updated or newly available data.
The search terms employed were as follows: (intercostal drain OR pleural drain OR subxiphoid drain OR drain) AND (coronary artery bypass surgery (CABG)). We also conducted manual searches by reviewing related references provided in the identified studies.
Eligibility criteria
In our meta-analysis, we considered randomized controlled trials and comparative studies. The study participants consisted of patients who had undergone CABG surgery. We included studies where intercostal left pleural drain insertion was the surgical intervention and the comparator was subxiphoid left pleural drain insertion. Patients who had undergone emergency CABG and surgery without left pleural drain insertion were excluded from our analysis.
The primary outcome of our study was the time required for ventilator support postoperatively and postoperative pain scores. The secondary outcome was postoperative spirometry parameters, including partial pressure of oxygen (PO2) in arterial blood gas (ABG), a decrease in percentage predicted vital capacity (VC), and a decrease in percentage predicted forced VC (FVC).
These criteria were used to ensure that the selected studies were relevant to our research objectives and allowed us to assess the impact of intercostal and subxiphoid left pleural drain insertion on the specified outcomes.
Data collection and analysis
Study Selection
The authors conducted an independent review of the abstracts and titles of the identified articles. All potentially relevant articles were thoroughly assessed by reviewing the full text. After eliminating any duplicate publications from the search results, the full texts of potentially eligible studies were retrieved. The authors independently evaluated these full-text articles to determine their eligibility for inclusion (Figure 1).
PRISMA flow diagramPRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses
Methodological Quality Assessment and Risk of Bias Assessment of Included Studies
To assess methodological quality, the authors employed the Modified Downs and Black scale [19]. Additionally, we calculated the Kappa coefficient to estimate the inter-rater reliability for the included studies using the Modified Downs and Black scale [20]. The authors independently assessed bias using the Cochrane Collaboration tool, specifically designed for randomized studies [21].
Data Extraction
Upon selecting the relevant studies, data extraction was carried out independently by the authors. The extracted data included baseline information for each study, such as author information and year of publication, as well as the number of patients in each study, the number of patients in each group, the mean or median age, and the age range of the included patients. Furthermore, the specified outcome measures were also extracted and recorded in a data extraction table using MS Excel (version 16.16.27; Microsoft Corporation, Redmond, Washington, United States). Any discrepancies between the two observers were resolved through consensus and consultation with the senior author.
Statistical Analysis
Continuous outcome variables were presented as mean differences (MDs) with corresponding 95% CIs. The individual participant was considered the preferred unit of analysis. To evaluate the heterogeneity among the studies, a visual assessment of the CI in the forest plot (eyeball test) was performed. Additionally, we quantified heterogeneity using the I2 statistics. The interpretation of I2 values followed these ranges: 0-40%: may not be significant; 30-60%: may indicate moderate heterogeneity; 50-90%: may suggest substantial heterogeneity; and 75-100%: indicates considerable heterogeneity [22].
These analyses were conducted to assess the variation among the included studies and to guide the interpretation of heterogeneity levels in the meta-analysis.
Results
The initial literature search yielded a total of 2,890 studies, with contributions from different sources: 300 from PubMed, 82 from Cochrane, 104 from Scopus, 2,400 from Google Scholar, and four from ClinicalTrials.gov. After removing duplicate studies, a total of 390 records were screened based on their titles and abstracts. Subsequently, 12 studies were selected for a full-text review, and from these, nine studies were included in the evaluation (comprising seven randomized and two nonrandomized studies), as illustrated in Figure 1.
Study Characteristics
A summary detailing the characteristics of the included studies can be found in Table 1.
Results of Individual Studies
The outcomes reported in all studies are summarized in Table 2.
Methodological Quality Assessment
The Modified Downs and Black scores were assigned to each study by two authors, and the results are presented in Table 3. Scores ranged from 11 to 18, with the study conducted by Guden et al. [13] receiving the highest score, while the study by Guizilini et al. [11] received the lowest score. Notably, there is a very high and positive correlation (r = 0.92) between the ratings provided by rater 1 and rater 2.
Meta-analysis of outcomes
Ventilation Time
Postoperative ventilation time was assessed in six studies, reported in mean and standard deviation format. A total of 129 patients were included in the intercostal group, while 133 were in the subxiphoid group. The pooled analysis indicated an MD of -0.66 (95% CI (-0.23, -1.08)), signifying shorter ventilation time in the subxiphoid group. However, significant heterogeneity (I2 = 92%) was observed among the studies (Figure 2).
Forest plot for ventilation time
Upon subgroup analysis, excluding the study by Guizilini et al. [23], which exclusively involved chronic obstructive pulmonary disease (COPD) patients undergoing CABG, five studies remained for analysis. In this subset, the subxiphoid group (n = 104) exhibited shorter ventilation time compared to the intercostal group (n = 102), with an MD of -1.43 (95% CI (-1.91, -0.95)). Nonetheless, there was still significant heterogeneity (I2 = 69%) among these studies, but the difference was statistically significant (P = 0.001) (Figure 3).
Forest plot for ventilation time excluding patients with COPDCOPD, chronic obstructive pulmonary disease
Pooled analysis was performed after excluding Elnasr et al. [8], Simon et al. [14], and Ozelami Vieira et al. [15], as they did not report ventilation time in the required format.
Pain Score
A pooled analysis of pain scores on postoperative day 1, involving five studies (144 patients in the subxiphoid group and 109 in the intercostal group), revealed a significant difference (MD = -2.34, 95% CI (-2.71, -1.97)), indicating lower pain scores in the subxiphoid group. No heterogeneity was observed (I2 = 0%). Subgroup analysis, excluding the study by Guizilini et al. [23], produced similar results (MD = -2.28, 95% CI (-2.66, -1.90)) with no heterogeneity (I2 = 0%) (Figure 4).
Forest plot for pain score on POD 1(A) Pain score on POD 1. (B) Pain score on POD 1 excluding patients with COPD.COPD, chronic obstructive pulmonary disease; POD, postoperative day
Elnasr et al. [8], Simon et al. [14], Hagl et al. [12], and Guden et al. [13] were not included in the analysis due to reasons such as missing pain score data or different findings. Notably, Elnasr et al. [8] reported higher tramadol use in the intercostal group, while Simon et al. [14] found no significant difference in subjective pain between the two groups. Hagl et al. [12] concluded that the subxiphoid group experienced significantly less pain during forced inspiration on postoperative day one.
Pooled analysis of pain scores on postoperative day 3, involving three studies (52 patients in the subxiphoid group and 49 in the intercostal group), indicated lower pain scores in the subxiphoid group (MD = -0.98, 95% CI (-1.35, -0.16)). However, significant heterogeneity was observed (I2 = 93%). Similarly, on postoperative day 5, pooled analysis from three studies (71 patients in the subxiphoid group and 67 in the intercostal group) showed lower pain scores in the subxiphoid group (MD = -0.81, 95% CI (-1.09, -0.53)), but with significant heterogeneity (I2 = 97%). These results should be interpreted cautiously due to their heterogeneity (Figure 5).
Forest plot for pain score on POD 3 and POD 5(A) Forest plot of pain score on POD 3. (B) Forest plot of pain score on POD 5.POD, postoperative day
Guden et al. [13] evaluated the effects of analgesia using Visual Analogue Scale and Verbal Rating Scale scores and found no significant differences in the cumulative doses of necessary rescue analgesics between the groups. The low pain scores in both groups suggested reduced pulmonary morbidity when effective analgesia was provided.
PO2
On postoperative day 1, pooled analysis of three studies (Hagl et al. [12], Ozelami Vieira et al. [15], and Cancio et al. [16]) measuring PO2 in ABG (52 patients in the subxiphoid group and 49 in the intercostal group) suggested a greater decrease in PO2 in the intercostal group (MD = 10.17, 95% CI (5.40, 14.94)), with moderately significant heterogeneity (I2 = 61%) (Figure 6).
Forest plot for PO2 on POD 1PO2, partial pressure of oxygen; POD, postoperative day
Percentage Predicted VC and FEV
A pooled analysis of studies by Guizilini et al. [11,23], Hagl et al. [12], and Ozelami Vieira et al. [15] comparing the decrease in % predicted VC, involving 79 patients in the subxiphoid group and 78 in the intercostal group, revealed a greater decrease in VC in the intercostal group (MD = 10.91, 95% CI (7.36, 14.46)). However, there was significant heterogeneity among the studies (I2 = 81%).
Similarly, pooled analysis of the decrease in % predicted FEV from the same four studies, involving 79 patients in the subxiphoid group and 78 in the intercostal group, showed a greater decrease in predicted FEV in the intercostal group (MD = 7.11, 95% CI (4.14, 14.14)), with significant heterogeneity (I2 = 80%) (Figure 7).
Forest plot for the decrease in percentage predicted VC and FVC(A) Forest plot for the decrease in percentage predicted VC. (B) Forest plot for decrease in percentage predicted FVC.FVC, forced vital capacity; VC, vital capacity
Discussion
Numerous factors can compromise pulmonary function following CABG surgery involving the left internal mammary artery (LIMA). Some of these studies have examined technical questions regarding chest tube placement and its impact on postoperative pulmonary function. This meta-analysis represents the most comprehensive comparison to date of the clinical outcomes associated with subxiphoid and intercostal pleural drain insertion in CABG patients. Nine studies, including seven randomized and two nonrandomized trials, met the inclusion criteria, encompassing a total of 412 patients. Subgroup analysis of the included studies revealed several favorable outcomes in the subxiphoid group, including reduced pain scores, shorter ventilation time, improved spirometry parameters (VC and FEV), and a higher partial pressure of O2 in postoperative ABG analysis.
Pulmonary function is profoundly affected following cardiac surgery. General anesthesia during the procedure results in diminished respiratory muscle tone, decreased lung compliance, and increased total respiratory system resistance [24]. Median sternotomy further compounds these issues by impairing lung function, causing pain, and altering chest wall compliance. This surgical approach can delay lung function recovery and increase morbidity during the early postoperative period [25]. The use of the LIMA can exacerbate pulmonary dysfunction due to the more frequent opening of the pleura and the consequent need for pleural drainage [26,27]. Additionally, the removal of the internal mammary artery can reduce blood supply to the phrenic nerve, further contributing to postoperative pulmonary dysfunction [28]. All these factors contribute to a higher incidence of atelectasis, rendering patients more susceptible to hypoxic pulmonary complications, primarily pneumonia [12]. Sensoz et al. [29] demonstrated that intercostal pleural drains and subxiphoid drains had similar drainage capacity for pleural effusion but that subxiphoid drains reduced the incidence of atelectasis during the CABG postoperative period.
Chest tubes inserted and exteriorized in the intercostal space come into contact with the highly sensitive periosteum and parietal pleura. This contact can lead to ventilator-dependent pain, limiting deep inspiration and forcing patients to adopt antalgic postures, resulting in immobilization and reduced lung volumes and capacities [30]. Intercostal placement of the drain can irritate the intercostal nerves due to the large bore drain tube, increasing pain [12]. In contrast, subxiphoid drain placement does not breach the intercostal space, resulting in less pain.
This meta-analysis suggests that the preservation of respiratory muscle strength and oxygenation appears to be partly responsible for the shorter intubation time and reduced pain observed in patients with subxiphoid drains compared to intercostal drains. Moreover, the lesser interference with respiratory mechanics by subxiphoid drains leads to better preservation of spirometry parameters, enhancing patient compliance with chest physiotherapy and promoting earlier functional recovery of the lungs.
Limitations
There are some limitations to this study. Notably, Simon et al. [14] conducted elective CABG with extracorporeal circulation, while the other studies included patients who underwent off-pump CABG. The study by Guizilini et al. [23] included patients exclusively with coronary artery disease and COPD, whereas such patients were not included in the other studies. Additionally, the assessment of pulmonary function was not uniform across all studies, with some measuring VC and FEV while Simon et al. [14] and Cancio et al. [16] measured maximal inspiratory pressure and maximal expiratory pressure.
Conclusions
This meta-analysis provides evidence that patients who undergo CABG with left pleural subxiphoid drain placement experience shorter ventilation times, lower pain scores, better postoperative percentages of predicted VC and FVC, and a higher partial pressure of O2 in ABG compared to those with intercostal drain placement. These findings support the notion that subxiphoid left pleural drainage after CABG is associated with less discomfort and better respiratory outcomes when compared to intercostal drainage.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Coronary artery bypass graft surgery: the past, present, and future of myocardial revascularisation Surg Res Pract Diodato M Chedrawy EG 726158201420142537496010.1155/2014/726158 PMC 4208586 · doi ↗ · pubmed ↗
- 2Conduits used in coronary artery bypass grafting: a review of morphological studies Ann Thorac Cardiovasc Surg Martínez-González B Reyes-Hernández CG Quiroga-Garza A Rodríguez-Rodríguez VE Esparza-Hernández CN Elizondo-Omaña RE Guzmán-López S 55652320172820289510.5761/atcs.ra.16-00178 PMC 5422630 · doi ↗ · pubmed ↗
- 3Long-term results of internal thoracic artery grafting Arterial Grafting for Coronary Artery Bypass Surgery Sabik JF 3rd Loop FD 112Berlin, Heidelberg Springer 1052006
- 4Long-term pulmonary functional status following coronary artery bypass grafting surgery ARYA Atheroscler Rouhi-Boroujeni H Rouhi-Boroujeni H Rouhi-Boroujeni P Sedehi M 163166112015 https://pubmed.ncbi.nlm.nih.gov/26405447/26405447 PMC 4568203 · pubmed ↗
- 5Effect of sternotomy and coronary bypass surgery on postoperative pulmonary mechanics. Comparison of internal mammary and saphenous vein bypass grafts Chest Berrizbeitia LD Tessler S Jacobowitz IJ Kaplan P Budzilowicz L Cunningham JN 873876961989279168610.1378/chest.96.4.873 · doi ↗ · pubmed ↗
- 6Postoperative pleural changes after coronary revascularization. Comparison between saphenous vein and internal mammary artery grafting Chest Peng MJ Vargas FS Cukier A Terra-Filho M Teixeira LR Light RW 3273301011992173524910.1378/chest.101.2.327 · doi ↗ · pubmed ↗
- 7Does more than a single chest tube for mediastinal drainage affect outcomes after cardiac surgery?Can J Surg Le J Buth KJ Hirsch GM LégaréJF 1001065820152559817810.1503/cjs.006814 PMC 4373991 · doi ↗ · pubmed ↗
- 8Intercostal versus subxiphoid approach for pleural drainage post coronary artery bypass grafting J Egypt Soc Cardiothorac Surg Elnasr MA Arafat AA Wahab AA Taha AM 813252017