Evaluating soluble Axl as a biomarker for glioblastoma: A pilot study
Daniel Raymond, Melanie Fukui, Samuel Zwernik, Amin Kassam, Richard Rovin, Parvez Akhtar, Salvatore V Pizzo, Salvatore V Pizzo, Salvatore V Pizzo

TL;DR
This pilot study explores whether soluble Axl in blood can serve as a biomarker for glioblastoma but finds no significant difference between healthy individuals and patients.
Contribution
The study evaluates sAxl as a potential blood-based biomarker for glioblastoma in a small pilot setting.
Findings
No significant difference in sAxl levels between healthy volunteers and GBM patients.
Postoperative sAxl levels were significantly higher than preoperative levels.
Axl expression was low or absent in 55% of patient-derived GBM cell lines.
Abstract
With current imaging, discriminating tumor progression from treatment effect following immunotherapy or oncolytic virotherapy of glioblastoma (GBM) is challenging. A blood based diagnostic biomarker would therefore be helpful. Axl is a receptor tyrosine kinase that is highly expressed by many cancers including GBM. Axl expression is regulated through enzymatic cleavage of its extracellular domain. The resulting fragment can be detected in serum as soluble Axl (sAxl). sAxl levels can distinguish patients with melanoma, hepatocellular carcinoma, and pancreatic ductal adenocarcinoma from healthy controls. This is a pilot study to determine if sAxl is a candidate biomarker for GBM. The sAxl levels in the serum of 40 healthy volunteers and 20 GBM patients were determined using an enzyme-linked immunosorbent assay (ELISA). Pre- and post- operative sAxl levels were obtained. Volumetric MRI…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
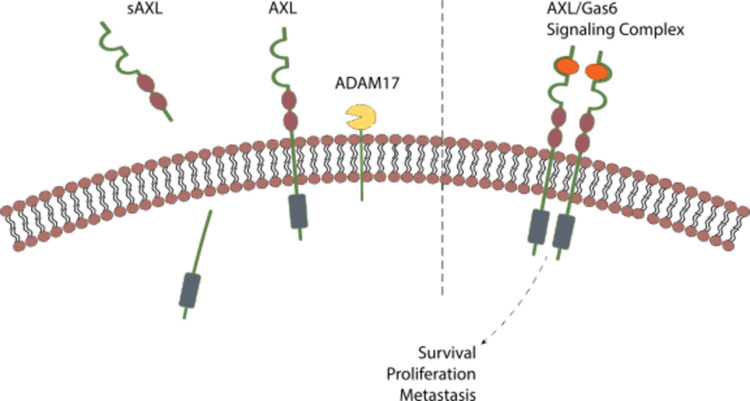 Fig 1
Fig 1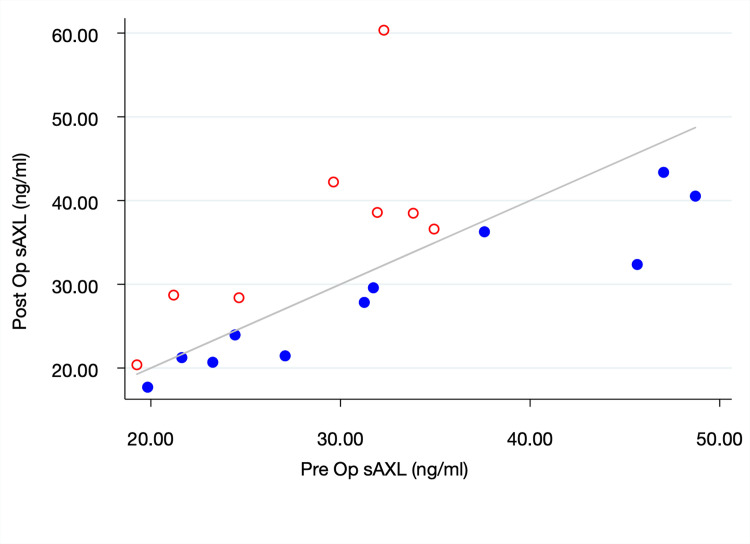 Fig 2
Fig 2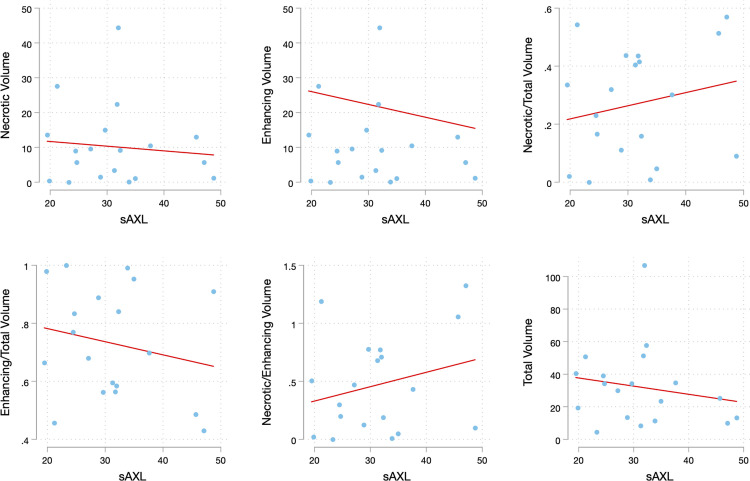 Fig 3
Fig 3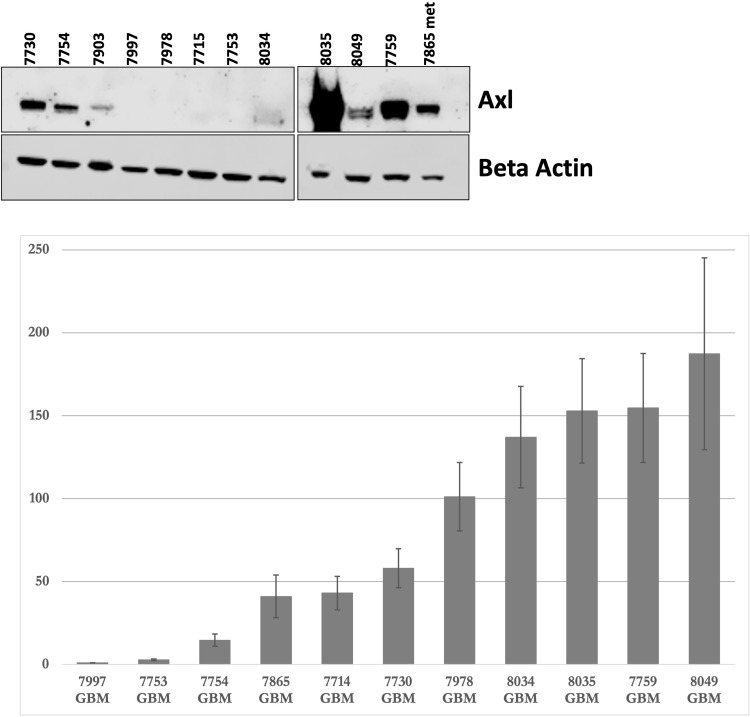 Fig 4
Fig 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPhagocytosis and Immune Regulation · Pancreatic and Hepatic Oncology Research · Glioma Diagnosis and Treatment
Introduction
Since 1977, interval imaging to monitor a brain tumor’s response to treatment has been standard of care [1]. However, distinguishing true progression from treatment effect (pseudoprogression) is challenging, particularly so with the advent of immunotherapy and oncolytic virotherapy [2]. A circulating biomarker that reflects the biological activity of the tumor would be useful. While available for breast cancer [3], lung cancer [4], melanoma [5], prostate cancer [6], and colorectal cancer [7], a circulating biomarker to monitor the course of gliomas remains elusive.
In earlier work, we found that patient derived glioblastoma (GBM) cell lines are susceptible to productive Zika virus infection especially when Axl is overexpressed [8]. Axl is a member of the TAM family of receptor tyrosine kinases (RTKs) along with Tyro3 and Mer. Like other RTKs, Axl has an extracellular domain for ligand binding, a transmembrane domain, and an intracellular domain. When stimulated through its ligand, growth-arrest specific factor 6 (Gas6), Axl activates myriad intracellular signaling pathways that contribute to the cancer phenotype, including: epithelial-mesenchymal transition, survival, proliferation, angiogenesis, chemotherapy resistance, and immune suppression [9, 10] (Fig 1, right).
Right. Axl signaling pathways and post-translational cleavage. Axl is a transmembrane receptor tyrosine kinase. Gas-6 ligand binding leads to dimerization and activation of cellular pathways including: epithelial-mesenchymal transition, survival, proliferation, angiogenesis, chemotherapy resistance, and immune suppression. left. Axl signaling pathways and post-translational cleavage. One mechanism to regulate Axl expression is cleavage of the extracellular domain by the sheddases ADAM10 and ADAM17. The cleavage product makes its way into the bloodstream as soluble Axl (sAxl).
Soluble Axl (sAxl) is the byproduct of regulation of Axl expression through post-translational deactivation by enzymatic cleavage. The sheddases ADAM10 and ADAM17 cleave the extracellular domain of Axl, and this product can be identified in the bloodstream as sAxl [9] (Fig 1, left). Many cancers highly express Axl [10]. In these cancers, cleavage of the Axl ectodomain leads to high levels of circulating sAxl. In this way, sAxl can serve as a biomarker for hepatocellular carcinoma [11], pancreatic cancer [12], and melanoma [13].
Given that Axl is also overexpressed in GBM [14], we hypothesized that serum sAxl levels should be elevated and could serve as a biomarker as it does in other solid tumors. Therefore, we designed this pilot study to determine if circulating sAxl levels are elevated in patients with GBM compared to healthy controls and to determine if there is a relationship between tumor volume and sAxl levels.
Materials and methods
This study was approved by the Northern Michigan University Institutional Review Board #HS19-1033 and the Aurora St Luke’s Institutional Review Board #14–79. Participants signed a written informed consent document before enrolling in this study.
Study design
This is a clinico-pathological correlation study using biospecimens (blood and tumor tissue) collected per an existing Aurora St Luke’s Medical Center biorepository protocol (Prospective Biospecimen Collection, Storage, and Distribution).
Study populations
Control cohort. Volunteers without pre-existing medical conditions were eligible to participate. The control group included students and faculty at Northern Michigan University, Marquette, Michigan. Student volunteers were recruited from the CLS 100 Phlebotomy course. Their blood draws for soluble Axl analysis were part of their standard course work. Blood collection for the control cohort took place between April 8^th^ and May 6^th^, 2019.
Glioblastoma patients. Patients with preoperative imaging consistent with GBM were eligible to participate in this study. Patients underwent medically indicated surgery at Aurora St Luke’s Medical Center, Milwaukee, Wisconsin. Blood was collected before and after surgery and did not necessitate additional venipuncture. Blood collection for the GBM cohort took place between April 1^st^, 2018 and October 31^st^, 2018.
Patient derived cell lines. The patient derived GBM cell lines used to determine Axl expression and sAxl levels in cell culture supernatant were previously established. They are not derived from patients participating in the current study.
Serum collection
The blood collection tubes were labeled with a randomly generated ID number. The samples were deidentified except for age, biological sex, cohort, and, for the GBM cohort, the time period (pre- or post- operative) of the blood draw.
Serum was separated from whole blood samples using gold-top serum separator tubes, which were then centrifuged at 1000 rpm for 5–10 minutes. Serum was aliquoted and stored at -80° C.
Enzyme-linked immunosorbent assay for sAxl concentration
Serum sAxl and cell culture supernatant sAxl concentrations were determined by enzyme linked immunosorbent assay (ELISA) using the commercially available human Axl DuoSet ELISA kit (R&D Biosystems, Minneapolis, MN) with previously reported optimizations [15]. The 96-well ELISA plates were read in a multi-mode microplate reader (BioTek Synergy H1, Agilent Technologies, Santa Clara, CA). The optical density was measured at 450nm and 540nm. For wavelength correction, the 540nm measurement was subtracted from the corresponding 450nm value. After adjusting for background by normalizing against blank wells, a four-parameter logarithmic curve-fit was generated in GraphPad Prism. A standard curve using known sAxl standards was generated and used to interpolate the sAxl concentration of the samples. For each plate, standards were applied in duplicate, and samples were applied in triplicate. The assay was repeated either the same day using a duplicate 96-well plate on a separate day.
MRI volumetric tumor analysis
MRI scans were analyzed by a board certified neuroradiologist (M.B.F.) using BrightMatter Plan software (Synaptive Medical, Toronto, Canada). From gadolinium enhanced T-1 weighted images, a 3D model of the tumor was generated. From the pre-operative scans, total tumor volume, volume of enhancing tumor, and volume of necrotic tumor were determined. The ratios of enhancing tumor volume to total tumor volume, necrotic tumor volume to total tumor volume, and necrotic tumor volume to enhancing tumor volume were calculated.
Cell lines and cultures
Previously established and characterized patient derived glioblastoma stem cell lines were maintained in NeuroCult NS-A basal medium (Stemcell Technologies), supplemented with B-27 without vitamin A, N-2, GlutaMAX and Pen/Strep (Thermo Fisher Scientific), BSA and heparin (Sigma-Aldrich), human recombinant bFGF and EGF (20 ng/ml each; PeproTech Inc.). All cell lines were routinely tested for mycoplasma contamination by using MycoAlert Detection Kit (Lonza Inc.).
Western blotting
Patient derived GBM stem cells were collected and lysed in RIPA buffer with complete protease inhibitor cocktail (Roche). Lysates were resolved by 4–12% SDS/PAGE and electrotransferred to nitrocellulose iBlot 2 Transfer Stacks (Life Technologies, IB23002). Membranes were blocked with 5% nonfat dry milk in 1x TBS and incubated overnight at 4°C with anti-AXL primary antibody (1: 1000 dilution, R&D Systems, AF154) or β-actin antibody (Sigma, A2066), and subsequently incubated for 1 hour at room temperature with HRP-coupled secondary antibody. All membranes were scanned using the Odyssey infrared imaging system (LI-COR Biosciences) in conjunction with the Clarity Western ECL Substrate (Bio-Rad).
RNA extraction and qRT-PCR
Total RNA was extracted from patient derived GBM stem cells using the RNeasy Mini Kit (Qiagen). Isolated RNAs (1 μg total RNA) were then digested with 1 unit of DNase I (NEB) at 37°C for 25 min to remove genomic DNA contamination before being processed for reverse transcription. Quantitative real time polymerase chain reaction (qRT-PCR) was performed using iTaq Universal SYBR Green One-Step Kit (Bio-Rad, 1725151) according to the manufacturer’s instructions on a Roche LightCycler 480 instrument. The primers for Axl quantification were Forward primer 5′-GGTGGCTGTGAAGACGATGA-3′; Reverse primer 5′-CTCAGATACTCCATGCCACT-3′. The control primers were GAPDH Forward primer 5’- GGATTTGGTCGTATTGGG -3’; Reverse primer 5’- GGAAGATGGTGATGGGATT -3’. Relative expression quantification was performed based on the comparative CT Method (2^-ΔΔCt^), using GAPDH as an endogenous reference control.
Statistical analysis
Data from ELISAs were interpreted using a four-parameter logarithmic curve in GraphPad Prism version 10.1.0 (GraphPad Software, San Diego, CA). Determination of statistically significant variation between the two groups was performed using a two-tailed, unpaired student’s t-test. For datasets with three or more groups were analyzed using one-way ANOVA with Dunnett’s post-hoc multiple comparisons test. Graphical representation of datasets was performed in GraphPad with error bars representing either 95% confidence intervals or mean ± SEM. Correlation between tumor volume measurements and sAxl levels was determined using the Spearman method; p values are provided to judge significance. This and graphical representation of datasets were performed using Stata version 15 (StataCorp, College Station, TX).
Results
Baseline sAxl levels in the control and GBM populations
There were 40 volunteers in the control group and 20 patients in the GBM group. The sAxl level for the healthy controls of 30.16 ± 1.88 ng/ml (mean ± SD) and the preoperative sAxl level in the GBM cohort of 30.74 ± 1.96 ng/ml were not significantly different, p = 0.27. (Table 1)
Table 1: Characteristics of the healthy control and glioblastoma (GBM) cohorts.
sAxl levels in response to surgery
There were 19 GBM patients with matched pre- and post- operative sAxl levels. We found that the post-operative sAxl level (32.32±2.26 ng/ml) was significantly higher than the pre-operative sAxl level (30.74±1.96 ng/ml), p = 0.03. In 11 (58%) patients, the preoperative sAxl level was greater than the postoperative level. (Fig 2)
The relationship between pre- and post-operative soluble Axl levels.The blue closed circles represent patients with postoperative sAxl levels lower than their preoperative levels. The red open circles represent patients with postoperative sAxl levels higher than preoperative. The diagonal line denotes pre- and post-operative sAxl equality.
Correlation between preoperative tumor volume and sAxl levels
Twenty patients had matched preoperative tumor volumes measurements and sAxl levels. There was no correlation between total, enhancing, and necrotic tumor volumes and sAxl level. Nor was there a correlation between necrotic to enhancing, necrotic to total, or enhancing to total volume ratios and sAxl levels. (Table 2 and Fig 3)
The relationship between tumor volume metrics and soluble Axl levels.Multiple scatter plots visualize the lack of correlation between tumor volume metrics and sAxl levels. The total tumor volume, necrotic tumor volume, and enhancing tumor volume were determined through volumetric analysis of preoperative MRI scans. The ratios of necrotic to total volume, enhancing to total volume, and necrotic to enhancing volume were then calculated.
Table 2: Correlation between preoperative MRI tumor volume measurements and sAXL level.
Axl expression and sAxl levels in patient derived glioblastoma cell lines
Tumor Axl expression from the GBM patients participating in this study was not determined. Therefore, to get a sense of Axl expression and sAxl levels in GBM, we performed Western blot (Fig 4A) and qRT-PCR (Fig 4B) using our previously established GBM cell lines. The original uncropped, unadjusted gel/blot images are compiled in the PDF document named S1 Raw images. This file is available as Supporting Information. We also determined sAxl levels in the cell culture supernatants using ELISA. No or low Axl expression was seen in 55% of cell lines by Western blot and 33% of cell lines by qRT-PCR. The sAxl levels in the supernatants were not detected or low in 40% of cell lines. (Table 3)
The expression of Axl and soluble Axl in patient derived glioblastoma cell lines.(A) Axl protein expression as determined by Western blot. (B) Axl mRNA expression as determined by qRT-PCR. The mean value and standard deviations are plotted. Each measurement was performed in triplicate and the experiment repeated at least twice.
Table 3: Axl expression and sAxl levels in patient derived glioblastoma cell lines.
Relative Axl levels are reported as mean (standard deviation) as determined by qRT-PCR. This is visualized in Fig 4. sAxl levels in the cell culture supernatant as determined by ELISA.
Discussion
Soluble Axl (sAxl) has emerged as a promising biomarker for the early detection, diagnosis, and monitoring of various cancers [10], including pancreatic ductal adenocarcinoma [12], hepatocellular carcinoma [11, 15], and melanoma [13]. We hypothesized that given the increased expression of Axl in GBM [14], circulating sAxl levels would correspondingly be elevated. We designed this pilot study to determine if sAxl levels were elevated in patients with GBM and if levels correlated with tumor burden. Though the sAxl levels in our GBM cohort were comparable to levels reported in the literature for other cancers, we did not find a difference in sAxl levels between healthy controls and GBM patients. (Table 4) Nor did we find a correlation between sAxl levels and tumor volume. (Table 2 and Fig 3).
Table 4: Serum levels of soluble Axl in several cancers.
As noted in Table 3 above, we found a range of Axl expression in our established GBM cell lines, including no or low Axl expression in just over half of the specimens by Western blot. Moreover, cell lines with no or low Axl expression had no or low sAxl in the cell culture supernatant. A close review of Fig 1A from the Hutterer et al., paper showed 16 of 30 GBM samples had no or low Axl mRNA expression [14].
The regulation of Axl expression is complex and involves transcriptional, post-transcriptional, and post-translational pathways [10]. The post-translational cleavage of the Axl extracellular domain by ADAM10 and ADAM17 creates the soluble Axl fragments [9, 18]. It is possible, then, that in our small cohort, no or low Axl expressing GBMs were overrepresented, lowering the mean sAxl level.
We further hypothesized that sAxl levels would decline following cytoreduction. Unexpectedly, we found postoperative sAxl levels were significantly higher than preoperative. The reason for this is unclear.
In the hope of using sAxl as a proxy for tumor burden [19], we determined total tumor volume, volume of enhancing (and presumably viable) tumor, and volume of necrotic tumor. We found no correlation between these tumor metrics and sAxl levels.
Though our findings that sAxl levels in GBM do not discriminate healthy controls from patients with tumor and do not reflect tumor burden are different from findings in other cancers, they are not unique. Gustafsson et al., found that sAxl levels in patients with renal cell carcinoma (RCC) were lower than in healthy controls, did not correlate with tumor Axl expression, nor tumor size [20]. This suggests that tumor type and its microenvironment impact Axl regulation and sAxl production.
Conclusion
This study is innovative because we additionally included a comparison of pre- and post- operative sAxl levels, and we correlated volumetric MRI tumor metrics with sAxl levels. While this study does not support sAxl as a biomarker for GBM, it is not fair to make a definitive statement given our small sample size. As identifying a GBM biomarker for detection, monitoring, and prognostication, is important, a larger study can be considered.
Supporting information
S1 Raw imagesThe original uncropped, unadjusted gel/blot images.(PDF)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Levin VA, Crafts DC, Norman DM, Hoffer PB, Spire JP, Wilson CB. Criteria for evaluating patients undergoing chemotherapy for malignant brain tumors. J Neurosurg. 1977;47: 329–335. doi: 10.3171/jns.1977.47.3.0329 894339 · doi ↗ · pubmed ↗
- 2Wen PY, van den Bent M, Youssef G, Cloughesy TF, Ellingson BM, Weller M, et al. RANO 2.0: Update to the Response Assessment in Neuro-Oncology Criteria for High- and Low-Grade Gliomas in Adults. Journal of Clinical Oncology. 2023;41: 5187–5199. doi: 10.1200/jco.23.01059 37774317 PMC 10860967 · doi ↗ · pubmed ↗
- 3Dawson S-J, Tsui DWY, Murtaza M, Biggs H, Rueda OM, Chin S-F, et al. Analysis of circulating tumor DNA to monitor metastatic breast cancer. N Engl J Med. 2013;368: 1199–1209. doi: 10.1056/NEJ Moa 1213261 23484797 · doi ↗ · pubmed ↗
- 4Oxnard GR, Paweletz CP, Kuang Y, Mach SL, O’Connell A, Messineo MM, et al. Noninvasive detection of response and resistance in EGFR-mutant lung cancer using quantitative next-generation genotyping of cell-free plasma DNA. Clin Cancer Res. 2014;20: 1698–1705. doi: 10.1158/1078-0432.CCR-13-2482 24429876 PMC 3959249 · doi ↗ · pubmed ↗
- 5Tsao SC-H, Weiss J, Hudson C, Christophi C, Cebon J, Behren A, et al. Monitoring response to therapy in melanoma by quantifying circulating tumour DNA with droplet digital PCR for BRAF and NRAS mutations. Sci Rep. 2015;5: 11198. doi: 10.1038/srep 11198 26095797 PMC 4476039 · doi ↗ · pubmed ↗
- 6Hennessey DB, Lynn C, Templeton H, Chambers K, Mulholland C. The PSA tracker: a computerised health care system initiative in Northern Ireland. Ulster Med J. 2013;82: 146–149. 24505148 PMC 3913403 · pubmed ↗
- 7Campos-da-Paz M, Dórea JG, Galdino AS, Lacava ZGM, de Fatima Menezes Almeida Santos M. Carcinoembryonic Antigen (CEA) and Hepatic Metastasis in Colorectal Cancer: Update on Biomarker for Clinical and Biotechnological Approaches. Recent Pat Biotechnol. 2018;12: 269–279. doi: 10.2174/1872208312666180731104244 30062978 · doi ↗ · pubmed ↗
- 8Zwernik SD, Adams BH, Raymond DA, Warner CM, Kassam AB, Rovin RA, et al. AXL receptor is required for Zika virus strain MR-766 infection in human glioblastoma cell lines. Mol Ther Oncolytics. 2021;23: 447–457. doi: 10.1016/j.omto.2021.11.001 34901388 PMC 8626839 · doi ↗ · pubmed ↗