A Case of Postoperative Noncardiogenic Edema: Negative Pressure Pulmonary Edema
Miloud Dewilde, Bart Lutin

TL;DR
This paper presents a case of a 24-year-old man who fully recovered from a rare type of post-surgery lung edema.
Contribution
The case highlights negative pressure pulmonary edema as a noncardiogenic cause of postoperative edema that resolves spontaneously.
Findings
Negative pressure pulmonary edema can occur after Cottle surgery.
The condition resolved completely without long-term complications.
It is a noncardiogenic cause of postoperative edema.
Abstract
A case of complete recovery of negative pressure pulmonary edema after a Cottle surgery in a 24-year-old male. Teaching point: Negative pressure pulmonary edema is an important cause of postoperative noncardiogenic edema, with the spontaneous disappearance of all complaints within a relatively short period.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
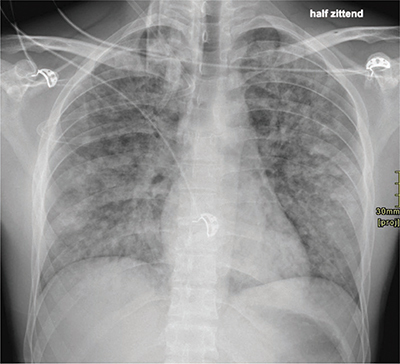 Figure 1
Figure 1 Figure 2
Figure 2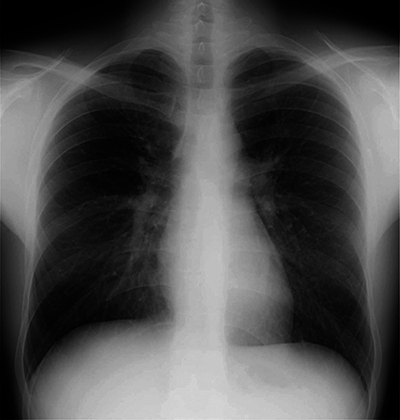 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRestraint-Related Deaths · Neuroscience of respiration and sleep · Traumatic Ocular and Foreign Body Injuries
Introduction
Negative pressure pulmonary edema (NPPE) is an important cause of postoperative noncardiogenic edema [1]. NPPE can result from laryngospasm or other types of upper airway obstruction following extubation [2, 3]. The etiology is multifactorial, but the main reported cause of NPPE is increased negative intrathoracic pressure with increased blood flow to the right heart. The pulmonary vascular bed dilates, the interstitial pressure around the capillaries decreases, with intravascular fluid is drawn into the interstitial space [4]. This worsens gas exchange and triggers a cascade of hypoxemia, catecholamine release, and systemic and pulmonary hypertension. The result is an acute increase in afterload, which worsens transcapillary fluid efflux and increases interstitial and alveolar edema [2].
Case Report
A 24-year-old man with known Gilbert’s syndrome underwent a Cottle septorhinoplastia because of a post-traumatic external and internal deviation of the nose and the nasal septum. Two months earlier, the patient traveled through Costa Rica and Mexico and tested positive for SARS-CoV-II. The patient was currently asymptomatic and fully recovered. The surgery was performed under general anesthesia. Postoperatively, oxygen demand with tachycardia persisted without further tachypnea or distress. A chest X-ray (Figure 1) showed distributed flocculent opacificaties in both lungs. There was no apparent pleural effusion. The image could be consistent with an alveolar edema.
Chest X-ray at day 1.
A chest computed tomography (CT) examination was performed to exclude a possible pulmonary embolism. The chest CT (Figure 2) showed bilateral and diffusely spread ground glass opacities with a flocculent aspect. Some limited flocculent consolidation components were also observed in both lower lobes. Bilateral, diffusely distributed centrilobular nodules were present (tree-in-bud). There was no pleural effusion, and pulmonary embolism was excluded.
Chest CT at day 1.
The differential diagnosis included both post-obstructive pulmonary edema (NPPE) and alveolar edema on medication or inhaled gases. Aspiration pneumonitis was considered unlikely.
After 5 days, a chest X-ray (Figure 3) showed complete regression of the pulmonary infiltrations, and the patient was discharged in good general condition without additional support.
Chest X-ray at day 5.
Discussion
It has been reported that NPPE occurs in less than 1/1000 surgical patients. Around 0.05% till 0.1% of all procedures involving intubation and general anesthesia may show NPPE, but it is often attributable to other etiologies [2, 3].
There are multiple risk factors, including obesity, a short neck, obstructive sleep apnea, or acromegaly. In addition, the risk of NPPE is considered to be higher after oral and maxillofacial surgery as compared to other types of surgery [5].
In cases of NPPE, supportive treatment is required. The patients receive supplemental oxygen, and hypervolemic patients may benefit from diuretics. In selected patients, bronchodilators and/or noninvasive continuous positive airway pressure (CPAP) may be helpful. Some patients will require reintubation [4]. In the long term, all complaints will disappear spontaneously within a relatively short period of time and without sequelae.
Conclusion
NPPE is a significant postoperative complication, primarily provoked by increased negative intrathoracic pressure following upper airway obstruction, often associated with laryngospasm. Typically, there is a need for supportive management and, in some cases, necessity of reintubation. Most patients experience complete resolution of symptoms within a relatively short period and without long-term sequelae.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Liu R, Wang J, Zhao G, Su Z. Negative pressure pulmonary edema after general anesthesia: A case report and literature review. Medicine (United States). 2019;98(17). DOI: 10.1097/MD.0000000000015389 PMC 683133431027133 · doi ↗ · pubmed ↗
- 2Mc Conkey PP. Postobstructive pulmonary oedema - A case series and review. Anaesth Intensive Care. 2000;28(1).10.1177/0310057 X 000280011410701042 · doi ↗ · pubmed ↗
- 3Timby J, Reed C, Zeilender S, Glauser FL. “Mechanical” causes of pulmonary edema. Chest. 1990;98(4).10.1378/chest.98.4.9732209159 · doi ↗ · pubmed ↗
- 4Krishnamurthy VT, Venkatesh SAT. Negative pressure pulmonary oedema after sedation in a patient undergoing pacemaker implantation. J Cardiovasc Dis Res. 2017;8(1).
- 5Mamiya H, Ichinohe T, Kaneko Y. Negative pressure pulmonary edema after oral and maxillofacial surgery. Anesthesia progress. 2009;56(2). DOI: 10.2344/0003-3006-56.2.49PMC 269969219642719 · doi ↗ · pubmed ↗