A Case on Papillary Thyroid Carcinoma With Intraluminal Tracheal Extension: A Malaysian Experience and Literature Review
Alex Zxi Jian Ho, Azwan Halim Abdul Wahab, Atikah Rozhan

TL;DR
This paper presents a rare case of papillary thyroid cancer that extended into the trachea, detailing the surgical challenges and outcomes.
Contribution
The paper contributes a case report and literature review on surgical approaches for tracheal-invading thyroid cancer.
Findings
A 56-year-old patient with tracheal-invading PTC underwent total thyroidectomy and partial tracheal resection.
Post-operative complications, including pulmonary embolism, led to the patient's death.
Surgical planning for tracheal invasion requires careful airway management and nerve monitoring.
Abstract
Papillary thyroid carcinoma (PTC) is a common malignancy originating from the thyroid gland. In rare cases, it can invade the trachea, resulting in airway obstruction. Subsequent surgical planning may be complicated as the technique selected depends on a case-by-case basis. Here, we report a case of PTC with tracheal involvement and a literature review on the latest surgical options. A 56-year-old gentleman presented with an anterior neck swelling of 3 x 3 cm for 3 months. Flexible endoscopy showed irregular mass in the subglottic region. Subsequent aspiration for cytology confirmed a diagnosis of PTC. Neck contrast enhanced computed tomography showed an ill-defined lesion in the right thyroid (3.1 x 3.8 x 2.9 cm) with a subtle irregularity of the adjacent tracheal wall suggestive of infiltration. The findings indicated a clinical staging of cT4aN0M0 (Stage III) with Shin’s staging of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1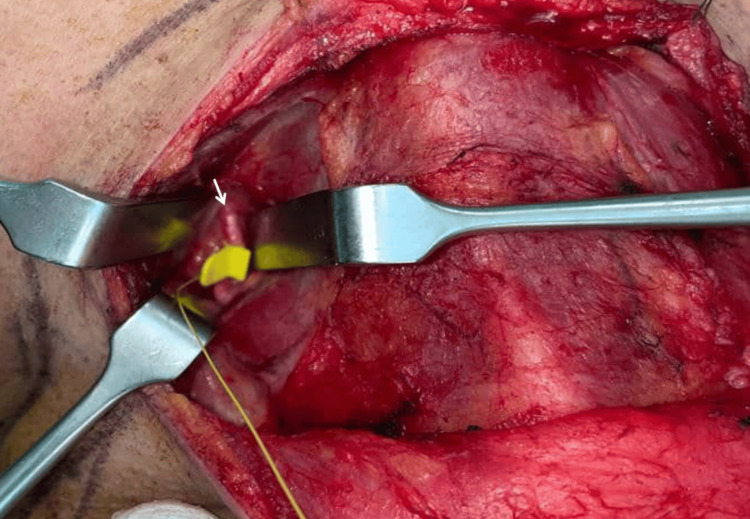 Figure 2
Figure 2 Figure 3
Figure 3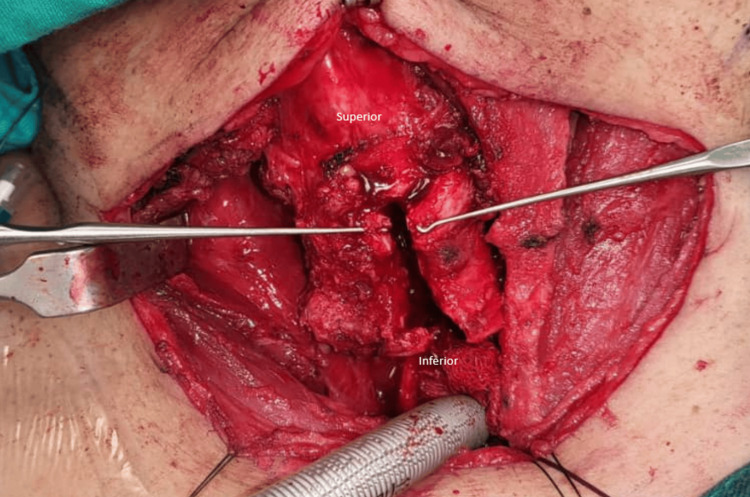 Figure 4
Figure 4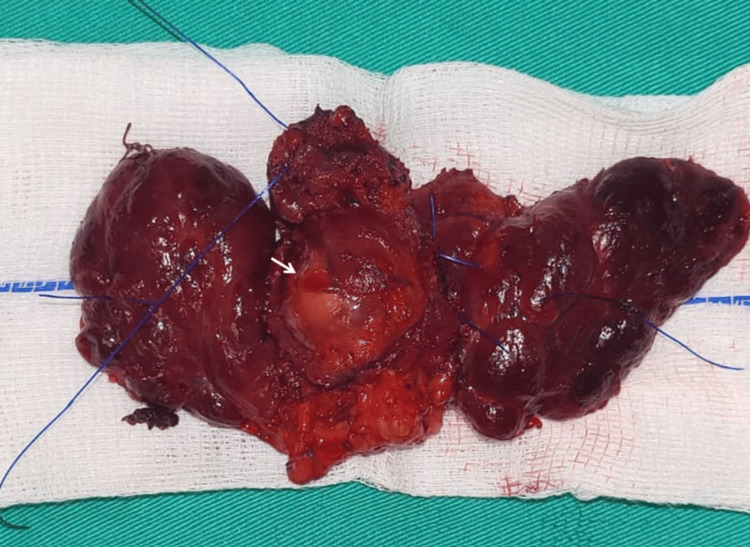 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTracheal and airway disorders · Head and Neck Anomalies · Thyroid and Parathyroid Surgery
Introduction
Papillary thyroid carcinoma (PTC) is a common malignancy of the thyroid gland with a common metastasis to surrounding cervical lymph nodes. Tracheal invasion is a rare complication that has the potential to cause airway obstruction. An incidence of 1% to 13% has been reported for tracheal involvement in such malignancies [1,2]. The presence of tracheal involvement complicates the subsequent surgical management, leading to increased morbidity and mortality. Here, we report a case of PTC with tracheal involvement, detailing our experience as well as a literature review on the latest surgical management options. This article was previously presented as a meeting abstract at the International Virtual Medical Research Symposium 2023 on December 7, 2023.
Case presentation
A 56-year-old gentleman presented with an anterior neck swelling of 3 x 3 cm. This was associated with increased effort tolerance and a feeling of discomfort upon lying flat. Flexible endoscopy showed irregular mass in the subglottic region. A subsequent aspiration for cytology revealed a diagnosis of PTC. Contrast enhanced computed tomography (CECT) of the neck showed a 3.1 x 3.8 x 2.9 cm ill-defined lesion in the right thyroid lobe abutting the trachea, with mass effect displacing it to the left (Figure 1).
Computed tomography of the neck showing thyroid lesion with tracheal involvementA: Axial cut with arrow showing tumor with tracheal cartilage invasionB: Sagittal cut with arrow showing tumor
A subtle irregularity of the tracheal wall was suggestive of tumor infiltration. Otherwise, multiple sub-centimeter cervical lymph nodes were seen at bilateral levels II, III, and IV regions.
The findings indicated a clinical staging of cT4aN0M0 (stage III) with Shin’s staging of stage IV. Subsequently, the patient underwent a total thyroidectomy with a single-stage partial cricoid-tracheal resection and anastomosis. He required intensive care post-surgery and was planned for intubation for 5 days to allow tracheal wound healing. Intravenous corticosteroids were given to prevent intraluminal granulation tissue formation. There were no immediate postoperative complications reported. However, the patient sustained pulmonary embolism, likely due to prolonged surgery and immobility, which eventually resulted in his demise. A subsequent histopathology report confirmed the diagnosis of PTC.
Discussion
We performed a total thyroidectomy with single-stage partial cricoid-tracheal resection and anastomosis for a case of PTC with tracheal invasion (Shin's stage 4). Upon neck incision, the tracheal cartilage was identified for the placement of a probe as part of Taiwan’s method of nerve monitoring. The left vagus nerve was identified in the region bordered by the superior omohyoid, sternocleidomastoid muscles, and midline of the neck. A probe was attached for continuous nerve monitoring. Next, the left recurrent laryngeal nerve (RLN) was identified and preserved, followed by a left thyroidectomy. The procedure was repeated on the right, with the vagus and right RLN identified and preserved (Figure 2). The right thyroid mass was noted to be embedded into the laryngeal framework in the right cricoid-tracheal region. It was then cut through, leaving tumor remnants.
Localization of the right vagus nerve with probe attachedArrow: Right vagus nerve
Following that, the patient was put under intermittent apnea as we performed a direct laryngoscopy and tracheoscopy to assess intraluminal tumor involvement. The intraluminal tumor length measured 1.9 cm, approximately 1.8 cm inferior to the vocal cords (Figure 3). Markings were made on the outer trachea using a needle as guidance. Reintubation was done with an endotracheal tube cuff positioned distal to the tumor level. The cricoid was split in the midline and extended inferiorly until complete visualization of the tumor (Figure 4). The anterior half of the cricoid with the involved tracheal segment measuring approximately 4 cm was removed (Figure 5). Stay sutures were placed at the lateral borders of the trachea to prevent inferior displacement. Both ends were anastomosed with interrupted sutures. (Posterior: 3 sutures; right/left) Anterolateral: 2 sutures each. Before closure, the Valsalva maneuver was performed with no evidence of leakage demonstrated.
Endoscopic view of tumor with trachea involvementArrow: Tumor
Midline cricoid split with inferior trachea extension
Gross thyroid, resected cricoid, and trachea specimenArrow: Intraluminal tumor
Generally, extrathyroidal extension in PTC indicates a poor prognosis. This is particularly so in cases of aerodigestive tract invasion [3]. Cases as such were described as having increased biological tumor aggressiveness secondary to reduced tumor suppressor adhesion molecule expression (e.g., E-cadherin) [4]. The TNM classification categorized extrathyroidal invasion of PTC with aerodigestive tract invasion as stage T4a [5].
Tracheal invasion was initially hypothesized to be an extension of a metastatic tumor from peritracheal lymph nodes. However, a newer study postulated that tracheal invasion was due to direct invasion of the primary tumor. This may occur through a potential weakness in the tracheal wall at sites of vessel penetration [6]. Shin et al. further described a classification of direct tumor invasion based on the depth of tracheal involvement [6].
In cases of superficial invasion with no cricoid or tracheal lumen breach, tracheal-preserving procedures such as shave excision were deemed appropriate [7]. Shave excision removes a superficially invading tumor with the preservation of normal cricoid and tracheal tissues [8]. Upon comparing shave excision to radical resection in cases of minimal invasion, similar survival rates were demonstrated [8].
However, complete resection is recommended when intraluminal involvement is present [4]. The approach to surgical intervention depends on the depth and extent of tumor involvement. In unilateral laryngotracheal invasion, window resection is recommended for cases with less than 50% tracheal ring circumference involvement spanning less than four tracheal rings [9]. Reconstruction is indicated when tumor involvement is more than one-third tracheal circumference with more than 2.5 cm in length [7]. Previously described techniques include the use of the sternocleidomastoid, pectoralis major muscle, and anterior cervical flap [9]. Vertical hemi-laryngectomy with repair is an alternative surgical consideration for extensive unilateral invasion [7].
Advanced tracheal invasion, such as in Shin’s Stage 4 cases, will require circumferential resection. Various studies suggest that cases with tumor infiltration of more than 50% tracheal ring circumference up to six rings would benefit from circumferential resection with anastomosis [7,9]. In cases with posterior trachea involvement, a total laryngectomy or laryngo-pharyngectomy may be required [7].
Our case had tumor infiltration involving more than 50% of the tracheal and cricoid circumference. The length involved was approximately 2 tracheal rings (1.9 cm). Therefore, it is a suitable case for partial crico-tracheal resection with anastomosis to achieve complete tumor removal. Resection in the cricothyroid region increases the risk of RLN injury as the nerve enters the larynx at this level. This could affect the outcome of surgery, as the risk of nerve injury has to be balanced with the risk of inadequate resection. In our case, cricoid resection was done meticulously with two intraoperative nerve monitoring systems. There was no intraoperative loss of signal, and the resection margins were clear. Incomplete tumor resection may lead to higher recurrence and worse survival rates [10].
Another issue to consider is intraoperative airway management, as a large intraluminal tumor may interfere with intubation. In such cases, excision of the intraluminal tumor may be performed via endoscopic technique. Methods such as endoscopic laser resection have been described in previous literature [11]. In cases where complete tracheal excision is not attainable, adjuvant radioiodine therapy should be given. Karkos et al. described a successful case of total thyroidectomy and endoscopic laser resection of a tumor with preservation of tracheal cartilages for a case of PTC. No recurrence was noted up to nine months of follow-up [11].
Unfortunately, we were unable to evaluate the long-term outcome of our patient due to unfortunate complications. Nevertheless, surgical intervention in such cases is a viable option to ensure complete disease removal. Future research into newer techniques and approaches would be beneficial, especially in cases with complicated tracheal involvement.
Conclusions
Surgical intervention in the management of PTC with tracheal involvement is a viable option to ensure complete disease removal. The choice of surgical technique or approach should be tailored specifically to each patient. In the future, further development of different techniques and approaches would be beneficial, especially in cases with complicated tracheal involvement.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1CT findings of central airway lesions causing airway stenosis-visualization and quantification: a pictorial essay Taehan Yongsang Uihakhoe Chi Choi MJ Kang H 144114768220213623887510.3348/jksr.2020.0212 PMC 9431977 · doi ↗ · pubmed ↗
- 2Surgical management of tracheal invasion by well-differentiated thyroid cancer Cancers (Basel) Matsumoto F Ikeda K 13202110.3390/cancers 13040797 PMC 791842933672929 · doi ↗ · pubmed ↗
- 3Prognostic significance of extrathyroid extension of papillary thyroid carcinoma: massive but not minimal extension affects the relapse-free survival World J Surg Ito Y Tomoda C Uruno T 7807863020061641101310.1007/s 00268-005-0270-z · doi ↗ · pubmed ↗
- 4Aerodigestive tract invasion by well-differentiated thyroid carcinoma: diagnosis, management, prognosis, and biology Laryngoscope Mc Caffrey JC 111116200610.1097/01.MLG.0000200428.26975.8616481800 · doi ↗ · pubmed ↗
- 5TNM classification of malignant tumours 7th edition: what's new for head and neck?Clin Otolaryngol Paleri V Mehanna H Wight RG 2702723520102073833410.1111/j.1749-4486.2010.02141.x · doi ↗ · pubmed ↗
- 6Pathologic staging of papillary carcinoma of the thyroid with airway invasion based on the anatomic manner of extension to the trachea: a clinicopathologic study based on 22 patients who underwent thyroidectomy and airway resection Hum Pathol Shin DH Mark EJ Suen HC 866870241993837585710.1016/0046-8177(93)90136-5 · doi ↗ · pubmed ↗
- 7Locally advanced differentiated thyroid cancer Surg Oncol Kebebew E Clark OH 91991220031294648010.1016/s 0960-7404(03)00032-x · doi ↗ · pubmed ↗
- 8Surgical management of cricotracheal invasion by papillary thyroid carcinoma Ann Surg Oncol Moritani S 400240072220152578674410.1245/s 10434-015-4492-5 · doi ↗ · pubmed ↗