Experience of focused workshop intervention in presentation skills - Importance of foundational skills for ophthalmologists in training
Snigdha Snigdha, Avinash Pathengay, Shefali Pandey, Ruby Kala Prakasam, Shobha Mocherla, Ninani Kombo, Chen Zhi Xiong

TL;DR
A workshop improved ophthalmology trainees' presentation skills, showing significant self-rated improvements in content and soft skills.
Contribution
Demonstrates the effectiveness of a focused workshop in enhancing presentation skills among ophthalmology trainees.
Findings
Self-rated presentation skills significantly improved after the workshop intervention.
Both content and soft skills showed statistically significant improvements across time points.
Workshops can be integrated into medical curricula to develop well-rounded professionals.
Abstract
The study was conducted to assess the impact of a workshop intervention designed to enhance presentation skills of ophthalmology fellows. A 10-hour workshop was conducted for ophthalmology trainees. Trainees were invited via email to participate by preparing a five-minute slide presentation and presenting it in person. Trainees from the fellowship 2022 batch (19 females and ten males) were included in the study. Participants completed a self-rating questionnaire to assess improvement in their presentation skills at different time points: Pre-Workshop (after introduction), During the Workshop (after trainee presentation), End-Workshop Intervention (after conclusion of all presentations), and Post-Workshop (scope of improvement). The self-rating questionnaire utilized a ten-point rating scale (1–10) and evaluated properties and content (PC) and soft skills (SS). Data were analysed using…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
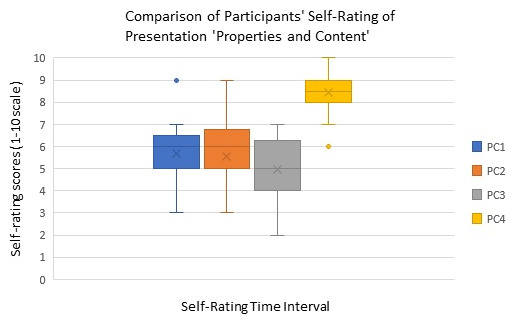 Figure 1
Figure 1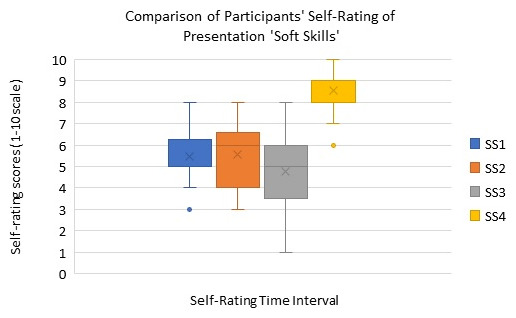 Figure 2
Figure 2| Serial Number | Self-rating questionnaire
| Time points |
|---|---|---|
| 1 | Rate your presentation skills (scale of 1–10)
| Pre-workshop (after introduction) PC1, SS1 |
| 2 | Rate your presentation skills today (scale of 1–10)
| During the workshop (after trainee presentation) PC2, SS2 |
| 3 | Rate your presentation skills today (scale of 1–10)
| At end of workshop intervention PC3,SS3 |
| 4 | Rate your scope of improvement
| Post-workshop intervention PC4,SS4 |
| 5 | Do you feel these workshops need to be revisited?
| Post-workshop intervention |
| 6 | If YES: how frequently?
| Post-workshop intervention |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInnovations in Medical Education · Empathy and Medical Education · Clinical Reasoning and Diagnostic Skills
Introduction
Skilful communication is intrinsic to professionalism ^ 1 ^. For doctors, professional presentation skills are fundamental resources for interpersonal and public interaction. With professional aspirations increasingly linked to effectively managing impressions ^ 2 ^, clinicians, scientists and researchers are using every opportunity to present themselves well.
For professional presenters, presentation skills give shape to an idea, helping to share ongoing learning with multiple teams. For medical professionals speaking to diverse audiences – colleagues, peers, patients, and the public – presentation skills help them to demonstrate their currency in medical knowledge and lobby for staged skill transfer through correct understanding, recall, internalization, and implementation ^ 3 ^.
Effective communication makes the good doctor popular, trusted ^ 4, 5 ^. Soft skills for medical doctors are coveted assets, and include speaking in the language preferred by the patient, giving precise instructions to follow, showing genuine concern, and maintaining pleasant interactions ^ 6, 7 ^. Generally, doctors in training learn standard responses and behaviours by observing their peers and seniors ^ 8– 10 ^. In medical schools in India, students are not tutored in role play and patient interactions as curricular activities ^ 11, 12 ^. Inculcating soft skills in medical education will empower doctors to master their delivery of care and service ^ 13– 15 ^. Presentation skill development may be effected by staged skill transfer, and therefore was taken on as an initiative at an eye health network in south central and eastern central India.
Methods
Workshop genesis and details
A 10-hour long physical workshop on presentation skills development was conducted on 2 ^nd^ July 2022 for trainees pursuing an ophthalmology fellowship. All the participants (29) were recruited as trainees under a common session of ophthalmology fellowship and was the eligibility criteria for enrolment in the workshop. The workshop was conducted in a classroom setting where the facilitator could facilitate the activity with the help of required audio-visual assistance. The learnings acquired when conducting virtual workshops during the COVID-19 lockdown helped us improve the structure and quality of the physical workshop. The data captured through this workshop ^ 16 ^ was later reviewed retrospectively. The entire process of workshop was explained by the facilitator in the beginning. The participants were actively encouraged to ask questions and clarify any doubts from time to time specially before self-rating at various intervals. This helped reduce any potential bias while rating themselves. The participants provided informed consent when completing the self-administered rating questionnaire in writing. The study complied with tenets of the Declaration of Helsinki. The study involved the study participants’ perceptions and study approval was obtained from the Institutional Review Board (IRB) of the Institute Ethics Committee (IEC) Hyderabad Eye Research Foundation later with the Ethics Reference Number: LEC-BHR -01-23-151 approved on 22 ^nd^ March 2023.
The trainees (Fellowship batch 2022, number=29) were initially invited via e-mail to participate in the presentation skills workshop.
The e-mail communication also included clear guidelines to prepare a 5-minute presentation for the workshop, on certain topics and presenting it in person during the workshop. The workshop began with a speech by the facilitator/moderator introducing the structure and sequential content, inviting the participants to fill-in a self-rating questionnaire survey. The self-assessment form was distributed to all trainees and the self-rating procedure was explained to them at the beginning of the workshop. The self-ratings were administered at four different time points of the workshop (See Table 1); pre-workshop (after introduction), during the workshop (after trainee presentations), end of-workshop (after concluding workshop intervention) and final response on scope of improvement (Post workshop intervention). The moderator allowed participant queries or suggestions, facilitating knowledge sharing.
**Table 1.: Description of self-rating questionnaire
18 .**
Self-administered rating
The self-rating consisted of ten-point rating scales (1–10) which evaluated two main components of presentation skills, 1. Properties and Content (PC), and 2. Soft Skills (SS) at four different time points. The final response collected participant perceptions on improvement in presentation skills, commenting on and sharing their preference for content, duration, location, format, and frequency of participation in similar workshops. (See Table 1)
Statistical analysis
Analyses were performed using SPSS Version 21.0 (IBM SPSS Statistics Inc., Armonk, NY, USA) software ^ 17 ^. Normality was checked using Shapiro Wilk test. Continuous data were represented as median range or interquartile range. Categorical data were presented in proportions. Multiple comparative analyses were performed using Friedman test. A probability value < 0.05 was considered statistically significant. Friedman test post-hoc analysis was applied for multiple comparisons and p-value < 0.02 was considered statistically significant.
Results
The analyses of self-rating scores of ophthalmology fellows at four different time points are illustrated in Figure 1 (See Figure 1). In all, 29 trainees in first year ophthalmology fellowship {19(65.51%) females and 10 (34.49%) males} were part of this workshop. The mean age of the participants was 28.89 +/- 2.5 (Mean, SD) years.
Box plot showing the comparison of participants’ presentation skills’ Properties and Content (PC) self-rating at different time points of the workshop.(PC1: Self rating after introduction, PC2: Self-rating during the workshop (after trainee presentation) PC3: Self-rating at end of workshop intervention, PC4: Self-rating at post-workshop intervention for gauging improvement).
The box-whisker plot in Figure 1 (See Figure 1) demonstrates participant self-rating about ‘properties and content’ of their presentation skill on a scale of 1–10 (with one indicating minimum and ten the maximum rating of oneself in presentation skill acquisition) at four different time points of the workshop (PC1, PC2, PC3, PC4). For all trainees, the self-rating at time point 4 (PC4), indicated improvement in ‘properties and content’ of the presentation compared to self-rating at the remaining three time points PC1, PC2, and PC3. This difference was statistically significant (Friedman Test, p<0.001). The median value at time point PC3 too showed that the trainees’ rated lower on properties and content aspects of presentation skills compared to earlier time points PC1 and PC2, however it was statistically insignificant.
The box-whisker plot in Figure 2 (See Figure 2) demonstrates the self-rating results of ophthalmology trainees on how they rate their learning of ‘soft skills’ during the presentation skills workshop on a scale of 1–10 at four different time points of the workshop (SS1, SS2, SS3, SS4). The self-rating 4 (SS4), scope of improvement in soft skills was found to be higher among trainees compared to self-rating at SS1, SS2, and SS3. This difference was statistically significant (Friedman Test, p<0.001). The median value of SS3 shows that the trainees’ rated lower on soft skill aspects of presentation compared to SS1 and SS2, however, it was statistically insignificant.
Box plot showing the comparison of self-rating of soft skills (SS) in presentation skills at four different time points of the workshop.SS1: self-rating after introduction to presentation skills workshop intervention, SS2: self-rating during the workshop (after trainee presentation), SS3: self-rating at end of workshop intervention, and SS4: self-rating for improvement post workshop intervention).
Overall, our study indicates that the presentation skills workshop positively impacted the ophthalmology trainees, and 93.10% (27 trainees) preferred revisiting the workshop for biannual (33%) or quarterly sessions (33%).
Discussion
While only a few studies have been published on impact of presentation skills training for ophthalmology students, there are several published articles focusing on presentation skills and communication skills of nurses and other health workers. A study conducted by Fowler and Jones that implemented an educational intervention to develop effective presentation skills in postgraduate nurses showed significant improvement in actual and perceived effectiveness of overall presentation skills ^ 19 ^. In our study too, the overall perceived effectiveness of workshop intervention in presentation skills was captured. The scope for improvement of the properties and content and soft skills components at fourth or last time point PC4 and SS4 revealed positive reactions to the presentation skills training. The corresponding f-test analyses (with Bonferroni assumption/Friedman post-hoc analyses) of participants’ self-ratings indicated that the training program led to higher scope for improvement in the participants’ presentation skills for the same components (PC4 and SS4) surveyed at the last time point.
Another study done by Seibold et al evaluated presentation skills training for participants from different industries (manufacturing, service, production, and research organizations) using a quasi-experimental design on behavioural skills ^ 20 ^. Statistical analyses showed positive reactions to the training, improvement in learning, short-term and long-term behavioural change, and on-the-job change in several skills. Similarly, in our study, the participant’s self-ratings indicated their perceived willingness to alter opinions and related behaviours that would demonstrably improve their personal presentation skills.
Our study showed the reduction in the mean scores of self-ratings PC1 and SS1 at the beginning of the workshop to the self-rating PC4 and SS4 post-workshop could be because of greater awareness and shared learning during skill transfer in the workshop.
The workshop succeeded in providing the participants a structure for developing both written and oral presentations. Such inculcation will likely encourage ophthalmology trainees to make better presentations in the classroom, at a conference, and various other platforms, as they begin to be astute young clinician-presenters. Tutoring novice doctors in presentation skills during induction into a tertiary eye care setting would equip them to seize presentation opportunities for growing their experience and acumen. Each time the trainees face an audience, whether of peers, colleagues, co-workers, patients and their families, donors, institutional management boards, vendors, or other stakeholders, they are catapulting themselves of their own zealous accord closer to leadership orbits and satellite positions of centre stage power in eye care service delivery.
The acceptance of our workshop is evident from the positive comments received from participants’ feedback, requesting a periodic (quarterly/biannual) intervention on presentation skills. We did not consider feedback on changing the workshop format as we have evolved from conducting virtual to hybrid format workshops over time. For greater participation, medical education is designed to include didactic lectures, simulated surgery, and increasingly, flipped or blended learning ^ 21– 24 ^. Transferring subject expertise through collaborative discussions requires dedicated time, so all these elements need to be carefully employed when conducting a short-term medical workshop intervention ^ 25– 27 ^.
Feedback and recommendations
The rigor and frequency of these workshops are not given due importance, perhaps because the hands-on training is not immediately applied, or not practiced in the spare time that must be created during a busy clinical workday.
We assert that this presentation skills workshop intervention is required for learners in all phases of higher medical education ^ 28– 31 ^. Some of the ways to improve workshop effectiveness are having fewer participants in the workshop for a higher trainer: student ratio, using audiovisual aids for easier visualization of and guided explanation of the teaching points, and deploying teachable moments for riveting their attention ^ 32– 35 ^. These educational strategies might be more relevant for training learners who require special attention. We strongly recommend educators in ophthalmology to incorporate into the syllabus, actively teach and practice presentation skills to better help learners in all phases of their training. Workshops on presentation skills and related foundational skills, such as managerial, technical and leadership skills, may ingrain in tertiary care trainees the holistic perspective required for an effortless yet steep learning curve. We recommend schooling tertiary care trainees in observation, curiosity, critical thinking, and similar basic building blocks or foundational skills of professionalism be started from primary and secondary care levels for optimal proficiency in science and medicine ^ 36– 39 ^.
Curiosity, which kindles creativity and rolls out sharing and discussion as by-products, initiates innovation, discovery, and invention ^ 40 ^. Communication and dissemination take forward the outcomes of curiosity – products, processes, and knowledge – to time-spaces near and far, for doing greater public good. Empathy, the basis of communication, builds the bonds that integrate all levels of bonding in society and is reported to decline in medical training ^ 41, 42 ^. After teasing out the technicalities of presentation skills, such as knowledge of the features of Microsoft PowerPoint, dealing with a breakdown midway, or maintaining a rapid pace of presentation, what remains are the creative and empathic factors in professional communication ^ 43 ^. Nonverbal communicativeness (by adopting measures such as proffering eye contact and a half smile that reaches the eyes, for presenting oneself well) signals the credibility of the speaker and topic, and can be medicinal, mood-elevating, and health-giving. Every effort must be made to inculcate empathy in medical trainees, so that they present well not only themselves but also the legacy institutions, mates, and others that they represent, in hospital corridors and wider world circles.
While being master (and slave) of the digital technology (multimedia production and display) of our times, continuing the presentation with personable equanimity (by staying unruffled on occasions when team spirit, system, software, or power supply become dysfunctional) is the ultimate test of one’s empathic leadership. We believe that training may be maximized by encouraging trainees to speak publicly and share widely their subject expertise – in the format of their recently acquired presentation skills ^ 44 ^. Along with such truly generous knowledge sharing, the surgeons’ attentiveness, learning and doing may disrupt disparities, hastening translational research in our society and razing the inequities miring our world ^ 45 ^. The movement back and forth from presentation granularity afforded by quality checklists to presenter self-reflexivity may work wonders for our post-pandemic digital endeavours – deep breathing life into our humanity and symbiotic sociality.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mahajan R Aruldhas BW Sharma M : Professionalism and ethics: A proposed curriculum for undergraduates. Int J Appl Basic Med Res. 2016;6(3):157–63. 10.4103/2229-516X.186963 27563578 PMC 4979294 · doi ↗ · pubmed ↗
- 2Goffman E : The presentation of self in everyday life.Anchor Books,1959. Reference Source
- 3Tsai JC : Medication adherence in glaucoma: approaches for optimizing patient compliance. Curr Opin Ophthalmol. 2006;17(2):190–195. 10.1097/01.icu.0000193078.47616.aa 16552255 · doi ↗ · pubmed ↗
- 4Honavar SG : Patient-physician relationship - Communication is the key. Indian J Ophthalmol. 2018;66(11):1527–1528. 10.4103/ijo.IJO_1760_18 30355854 PMC 6213668 · doi ↗ · pubmed ↗
- 5Ha JF Longnecker N : Doctor-patient communication: a review. Ochsner J. 2010;10(1):38–43. 21603354 PMC 3096184 · pubmed ↗
- 6Bensing JM Verhaak PF van Dulmen AM : Communication: the royal pathway to patient-centered medicine. Patient Educ Couns. 2000;39(1):1–3. 10.1016/s 0738-3991(99)00107-x 11013542 · doi ↗ · pubmed ↗
- 7King A Hoppe RB : "Best practice" for patient-centered communication: a narrative review. J Grad Med Educ. 2013;5(3):385–393. 10.4300/JGME-D-13-00072.1 24404300 PMC 3771166 · doi ↗ · pubmed ↗
- 8Perron NJ Nendaz M Louis-Simonet M : Impact of postgraduate training on communication skills teaching: a controlled study. BMC Med Educ. 2014;14: 80. 10.1186/1472-6920-14-80 24731477 PMC 3989778 · doi ↗ · pubmed ↗