Practical use of transanal decompression tube following the repair of fourth-degree perineal tears associated with vaginal delivery
Hisanori Miki, Kobayashi Toshinori, Hatta Masahiko, Takuki Yagyu, Mitsugu Sekimoto

TL;DR
A transanal decompression tube helps reduce complications after repairing severe perineal tears from vaginal delivery.
Contribution
A practical method using a transanal decompression tube is proposed to improve outcomes in fourth-degree perineal tear repair.
Findings
Five patients had successful repair with no fistula or incontinence.
Transanal decompression tube placement reduced anastomotic leakage risks.
Gastrografin enema and CT scans confirmed safety before tube removal.
Abstract
Fourth-degree perineal tears associated with vaginal delivery (PTAVD) occur in approximately 0.25 to 6% of vaginal deliveries. A persistent challenge in treating fourth-degree PTAVD is the high incidence of anastomotic leakage, leading to impaired quality of life, marked by incontinence, rectovaginal fistula, and painful sexual intercourse. Thus, effective interventions are necessary. Herein, we report our successful approach in repairing a fourth-degree PTAVD, involving the placement of a transanal decompression tube (TDT) during the early postoperative period. Five patients underwent the repair of fourth-degree PTAVD by suturing the mucosal and muscular layers of the rectum, and the vaginal wall in layers. Subsequently, a TDT was placed in the rectum, positioned 10–15 cm from the anal verge. The TDT was allowed to drain spontaneously without suction. Gastrografin enema examination…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
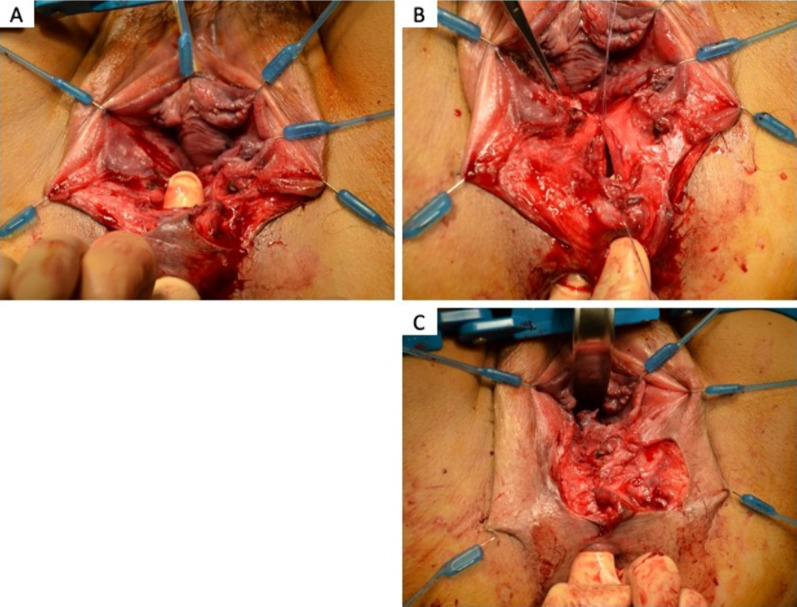 Figure 1
Figure 1 Figure 2
Figure 2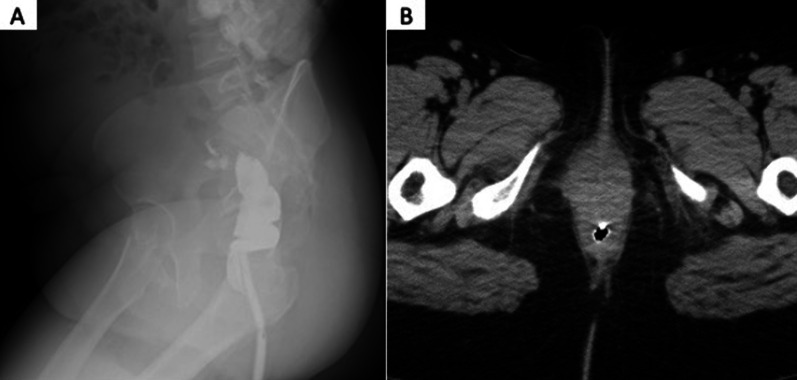 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnorectal Disease Treatments and Outcomes · Colorectal Cancer Surgical Treatments · Pelvic floor disorders treatments
Background
The American College of Obstetricians and Gynecologists classifies perineal tears associated with vaginal delivery (PTAVD) into four degrees based on injury severity. Fourth-degree PTAVD involves anal and rectal laceration [1], and occurs in 0.25–6% of vaginal deliveries [2]. Surgical repair is necessary, but a significant challenge is the frequent occurrence of anastomotic leakage [3], leading to complications such as fecal incontinence, painful sexual intercourse, and rectovaginal fistula [1, 4, 5]. Meticulous anatomic approximation during repair of all disrupted layers is recommended to minimize the leakage [5]. However, approximately 25% of patients with third- and fourth-degree PTAVD still experience anastomotic leakage [3]. The challenge of anastomotic leakage is parallel to the challenges of anal-sparing surgery for rectal cancer near the anus, where the incidence reaches to approximately 20%[6]. Severe anastomotic leakage results in lifelong defecation disturbances, such as fecal incontinence. Thus, to prevent anastomotic leakage, the creation of temporary stomas has been prompted. While numerous studies have proven the effectiveness of temporary stomas[7], stomas pose risks such as small bowel obstruction, high output, skin excoriation, herniation, prolapse, and associated surgical closure risks[8, 9]. Therefore, a transanal decompression tube (TDT) is proposed for anastomotic management during rectal surgery [10, 11]. In this study, a TDT was implanted to decompress the anastomosis after repair of 4th degree PTAVD and prevent infection due to stool contamination. The effectiveness of the TDTs was investigated and the results of the initial five cases are reported herein.
Case presentation
Five cases of fourth-degree PTAVD underwent surgical repair in our hospital between January 2019 and May 2022 (Table 1). The median age was 34 years (range: 29–38), median body mass index (BMI) was 21.72 (range: 17.58–36.63), and the median birth weight of the delivered infants was 3345 g (range: 2756–3650 g). All cases involved primiparous individuals, with vacuum-assisted delivery performed in four cases. Postoperatively, all patients received second-generation cephalosporin for 3–5 days. After cleansing the wound, the rectal mucosa and muscular layers were individually closed with 3-0 absorbable sutures. Subsequently, the posterior vaginal wall was closed with 3–0 absorbable sutures (Fig. 1). Finally, a TDT (10 mm soft pleated drain) was placed in the rectum, positioned 10–15 cm from the anal verge (Fig. 2). The TDT was left unaspirated and allowed to excrete spontaneously. Gastrografin, a water-soluble contrast agent was administered through TDT for the enema examination. Immediately after the examination, a plain computed tomographic scan (CT) was performed (Fig. 3) to check for contrast leakage, disruption of wall continuity, and abscesses. After unfavorable complications were ruled out, the patients resumed their normal diet. The median period from operation to gastrografin enema through TDT was 4 days (range: 1–8 days), and the median postoperative hospital stay was 11 days (range: 4–12 days). Case 3, who initially had fourth-degree PTAVD at another hospital, experienced anastomotic leakage seven days postoperatively following the initial suturing. The patient was sent to our hospital for further treatment. Due to the highly contaminated wound, we performed colostomy alongside TDT insertion, considering the high risk of anastomotic leakage despite careful resuturing.Table 1. Patients backgroundCaseAge (years)Height (cm)Weight (kg)BMI (kg/m^3^)Reproductive historyGestational age at birthDelivery methodBirth weight (g)1291558836.63G0P040w2dNormal304523415954.921.72G1P040w5dVacuum-assisted delivery3370333156.763.825.98G1P041w0dVacuum-assisted delivery3345437163.54717.58G1P036w2dVacuum-assisted delivery275653816254.820.2G1P039w4dVacuum-assisted delivery3650Fig. 1A Fourth-degree perineal tears associated with vaginal delivery. The finger passes from anal to vagina. B Suture of the rectal mucosal layer with 3-0 absorbable sutures. C Suture of the rectal muscular layer with 3-0 absorbable suturesFig. 2A soft pleated drain was inserted 10–15 cm from the anal verge and secured to the skin using 2-0 silk threadFig. 3Gastrografin enema (A) using a water-soluble contrast medium through the transanal decompression tube, followed by a plain computed tomography (B)
Result
In most cases, the TDT drained a minimal amount of stool. All patients demonstrated no evidence of anastomotic leakage on gastrografin enema and CT. Except for Case 3, all patients received laxatives post-TDT extraction. Over a median follow-up period of 2.7 years (range: 1.1–3.9), none of the patients developed rectovaginal fistula or fecal incontinence.
Discussion
While 0.1–5% of overall PTAVD patients experience anastomotic leakage, the incidence rises significantly to approximately 25% among patients with third- and fourth-degree PTAVD, with 20% facing wound infections within six weeks post-repair surgery [3]. Adequate laceration repair is crucial to prevent rectovaginal fistulas, as around 9% of rectovaginal fistulas in the United States are associated with PTAVD [5]. Postoperative management for third- and fourth-degree PTAVD remains relatively unexplored. Anastomotic leakage is often attributed to wound contamination, infection susceptibility, and unconscious increases in anorectum pressure, frequently disrupting rest at the suture site [12–15]. Intrarectal pressure can rise to 40–60 mmHg, causing involuntary anal contraction [16]. While antibiotics and laxatives are recommended as countermeasures [17], their effectiveness is limited. Therefore, taking more effective measures in preventing anastomotic leakage in fourth-degree PTAVD is essential. A key strategy we developed was to maintain the sutured rectum at rest immediately after suturing. This is considered necessary to prevent anastomotic leakage in anal-sparing surgery for low-lying rectal cancer. Temporary stomas have been utilized and have been proven effective. However, impaired cosmesis and complications, such as intestinal obstruction and skin disorders present as challenges. Furthermore, additional surgery will be required for closure. As a less invasive alternative, TDT offers a promising solution to prevent anastomotic leakage in fourth-degree PTAVD.
The use of TDT as an alternative to diverting stomas was first introduced by Rack et al. in 1966[18]. TDT involves the insertion of a drainage tube through the anus into the rectum to facilitate the expulsion of gas and stool during the early postoperative period. Both temporary stoma and TDT aim to reduce intra-rectal pressure and keep the suture sites at rest. Several studies have compared the effectiveness of temporary stomas and TDT, consistently reporting similar efficacy in reducing the occurrence of anastomotic leakage. [10, 11, 19–24]. However, TDTs may not reduce AL overall in patients undergoing rectal cancer surgery, and they are hardly a replacement for colostomy [22, 25]. Because PTAVD occurs in pregnant women, the disease is not pretreated as it is before rectal cancer surgery, and because of the low anastomosis close to the anus, the usefulness of TDTs may be higher in the treatment of PTAVD than after rectal cancer surgery. However, future case studies are needed.
Previous reports in rectal cancer surgery have suggested TDT indwelling periods ranging from 3 to 7 days, though the optimal duration remains unknown. Complications from TDT are rare; however, intestinal perforation has been reported in cases of long-term indwelling [26]. Early return to normal activities for breastfeeding and childcare is important for patients with perineal lacerations. Therefore, we adopted a strategy of removing the TDT 3 to 4 days after surgery, with the exception of case 3 where failure suture occurred once. Before removal, an enema test using gastrografin and CT was performed to examine for any signs of anastomotic leakage or damage caused by the TDT.
A normal diet was started after the enema test using gastrografin and CT, and no issues were identified in any cases. Once no problems were identified, a normal diet could be started, and long-term outcomes were good. Because adequate nutritional intake is essential for nursing mothers, the contrast method using a TDT suggests the possibility of clarifying when it is safe to start a normal diet.
Conclusion
We adopted a transanal decompression tube for postoperative management after repair of fourth-degree perineal tears associated with vaginal delivery. The new treatment was safely administered in five cases. Further studies are necessary to confirm their clinical efficacy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Reid AJ Beggs AD Sultan AH Roos AM Thakar R Outcome of repair of obstetric anal sphincter injuries after three years Int J Gynaecol Obstet 20141271475010.1016/j.ijgo.2014.04.01325097141 PMC 4175217 · doi ↗ · pubmed ↗
- 2Cunningham FG Leveno K Bloom SL Williams obstetrics 201424 New York Mc Graw-Hill 549
- 3Lewicky-Gaupp C Leader-Cramer A Johnson LL Kenton K Gossett DR Wound complications after obstetric anal sphincter injuries Obstet Gynecol 201512551088109310.1097/AOG.000000000000083325932836 · doi ↗ · pubmed ↗
- 4Priddis H Dahlen HG Schmied V Sneddon A Kettle C Brown C Risk of recurrence, subsequent mode of birth and morbidity for women who experienced severe perineal trauma in a first birth in New South Wales between 2000–2008: a population based data linkage study BMC Pregnancy Childbirth 20138138910.1186/1471-2393-13-89PMC 363594223565655 · doi ↗ · pubmed ↗
- 5Committee on Practice Bulletins-Obstetrics ACOG practice bulletin No. 198: prevention and management of obstetric lacerations at vaginal delivery Obstet Gynecol 20181323 e 87e 10210.1097/AOG.000000000000284130134424 · doi ↗ · pubmed ↗
- 6Cong ZJ Hu LH Bian ZQ Ye GY Yu MH Gao YH Systematic review of anastomotic leakage rate according to an international grading system following anterior resection for rectal cancer P Lo S ONE 201389 e 7551910.1371/journal.pone.007551924086552 PMC 3783382 · doi ↗ · pubmed ↗
- 7Matthiessen P Hallböök O Rutegård J Simert G Sjödahl R Defunctioning stoma reduces symptomatic anastomotic leakage after low anterior resection of the rectum for cancer: a randomized multicenter trial Ann Surg 2007246220721410.1097/SLA.0b 013e 318060302417667498 PMC 1933561 · doi ↗ · pubmed ↗
- 8Bakx R Busch OR Bemelman WA Veldink GJ Slors J Fvan Lanschot JJ Morbidity of temporary loop ileostomies Dig Surg 200421427728110.1159/00008020115308867 · doi ↗ · pubmed ↗