Utility of uneven double-lumen catheter for difficult guidewire manipulation in endoscopic ultrasonography-guided pancreaticogastrostomy
Ayaka Machida, Yusuke Takasaki, Sho Takahashi, Akinori Suzuki, Shigeto Ishii, Toshio Fujisawa, Hiroyuki Isayama

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
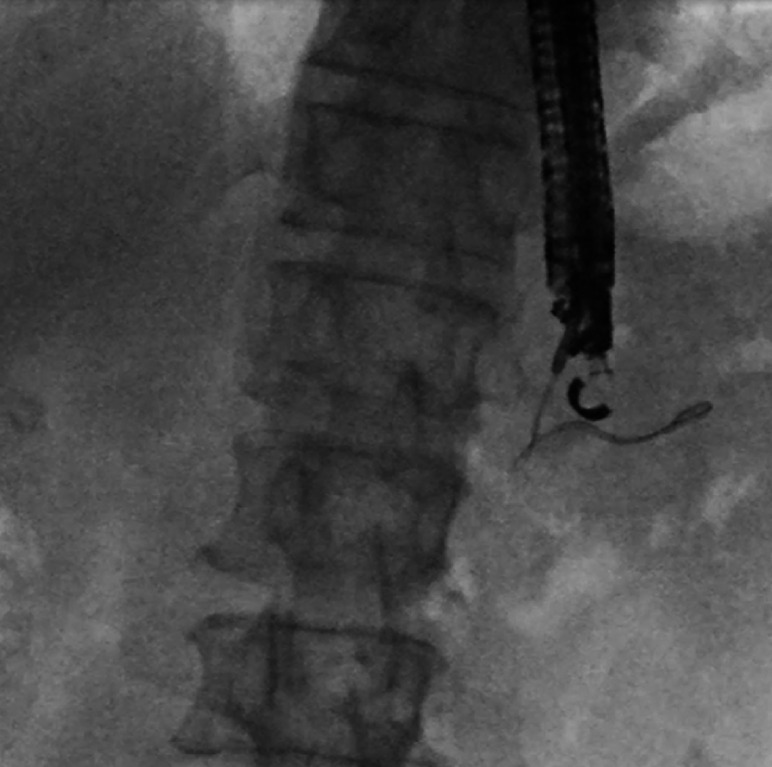 Fig. 1
Fig. 1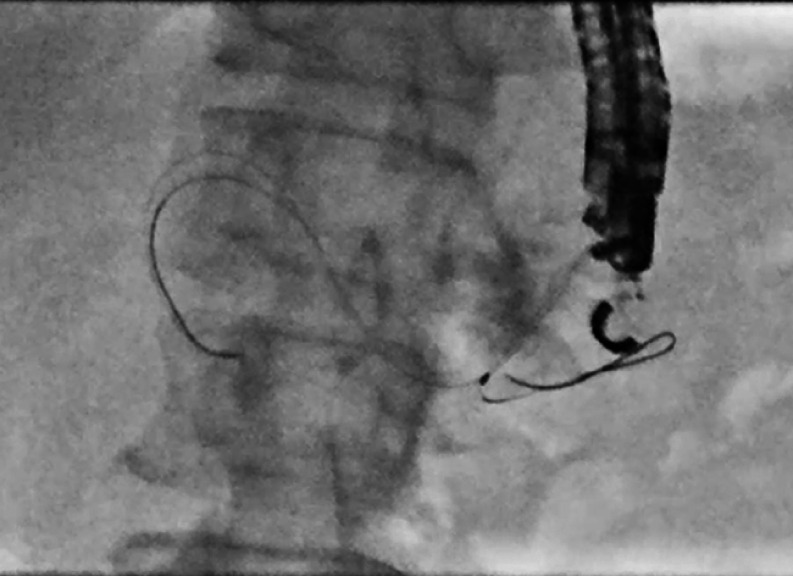 Fig. 2
Fig. 2 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatic and Hepatic Oncology Research · Gallbladder and Bile Duct Disorders · Esophageal and GI Pathology
Endoscopic ultrasonography-guided pancreaticogastrostomy (EUS-PGS) is a challenging procedure, and the most difficult step is guidewire insertion to the appropriate portion. We report herein a case in which the guidewire was not advanced in the correct direction after puncture during EUS-PGS, and a double-lumen catheter was used to correct the direction of the guidewire.
A 57-year-old man who had undergone subtotal stomach-preserving pancreaticoduodenectomy 5 years previously was referred to our department for management of recurrent pancreatitis due to pancreaticojejunostomy stenosis (PJS). As pancreatic access with balloon-assisted endoscopy had failed at the previous institution, we performed EUS-PGS with antegrade stenting across the PJS. We successfully punctured the main pancreatic duct (MPD) from the stomach with a 19-gauge needle (EZ Shot 3 Plus; Olympus Medical Systems, Tokyo, Japan) and injected contrast medium. A 0.025-inch angled guidewire (VisiGlide 2; Olympus Medical Systems) was then placed in the tail of the MPD because insertion toward the anastomotic site had failed ( Fig. 1 ). We kept the guidewire in the MPD and dilated the puncture tract with a bougie dilator (ES Dilator; Zeon Medical, Tokyo, Japan). We inserted an uneven double-lumen cannula (Piolax Medical Devices, Yokohama, Japan) with an additional a 0.025-inch guidewire (EndoSelector; Boston Scientific Japan, Tokyo, Japan) in the other lumen. The additional guidewire was inserted into the opposite side and then passed across the PJS ( Fig. 2 ). The PJS and puncture tract were dilated with a balloon dilator (REN 4 mm; Kaneka, Tokyo, Japan). Finally, a 7-Fr, 15-cm, double-pigtail stent (Zimmon Biliary Stent; Cook Medical, Bloomington, Indiana, USA) was placed across the PJS ( Fig. 3 , Video 1 ).
We were unable to insert the guidewire into the anastomotic site and, instead, could only place it on the opposite side (tail of the main pancreatic duct).
An uneven double-lumen cannula (Piolax Medical Devices, Yokohama, Japan) was inserted. A 0.025-inch guidewire (EndoSelector; Boston Scientific Japan, Tokyo, Japan) was then added from the other lumen and successfully inserted into the anastomotic site.
A 7-Fr, 15-cm, double-pigtail stent (Zimmon Biliary Stent; Cook Medical, Bloomington, Indiana, USA) was placed across the pancreaticojejunostomy stenosis.
When the guidewire was not advanced in the correct direction after puncture during endoscopic ultrasonography-guided pancreaticogastrostomy , a double-lumen catheter was useful for correcting the direction of the guidewire.Video 1
A double-lumen catheter was useful for changing the guidewire to the opposite side during EUS-PGS when the guidewire was not oriented in the correct direction.
Endoscopy_UCTN_Code_TTT_1AS_2AI