Postoperative Infection Following Hip Arthroscopy in Patients Receiving Preoperative Intra-articular Injections: A Systematic Review and Meta-Analysis
Sonia Aamer, Ilham Tokhi, Maaz Asim, Muzammil Akhtar, Daniel I Razick, Jimmy Wen, Trevor J Shelton

TL;DR
This study finds that hip arthroscopy patients who receive intra-articular injections within three months before surgery face a higher risk of postoperative infection.
Contribution
The study identifies a three-month safety window for preoperative intra-articular injections to reduce postoperative infection risk in hip arthroscopy.
Findings
Intra-articular injections anytime before hip arthroscopy increase infection risk compared to no injections.
Injections within three months before surgery significantly raise infection risk.
Injections more than three months before surgery do not significantly affect infection risk.
Abstract
Intra-articular injections prior to hip arthroscopy are often used to diagnose and conservatively manage hip pathologies, such as femoroacetabular impingement, labral tears, and chondral lesions. As a diagnostic tool, the relief of hip pain following an intra-articular injection helps pinpoint the primary source of pain and assists surgeons in recommending arthroscopic intervention for underlying intra-articular pathologies. However, when injections are not sufficiently spaced apart in time prior to hip arthroscopy, there is an elevated risk of postoperative infection. This systematic review aims to assess whether preoperative intra-articular injections prior to hip arthroscopy are associated with an increased risk of postoperative infection and to determine the safety timeframe for administering such injections prior to the procedure. A comprehensive search was conducted in the PubMed,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
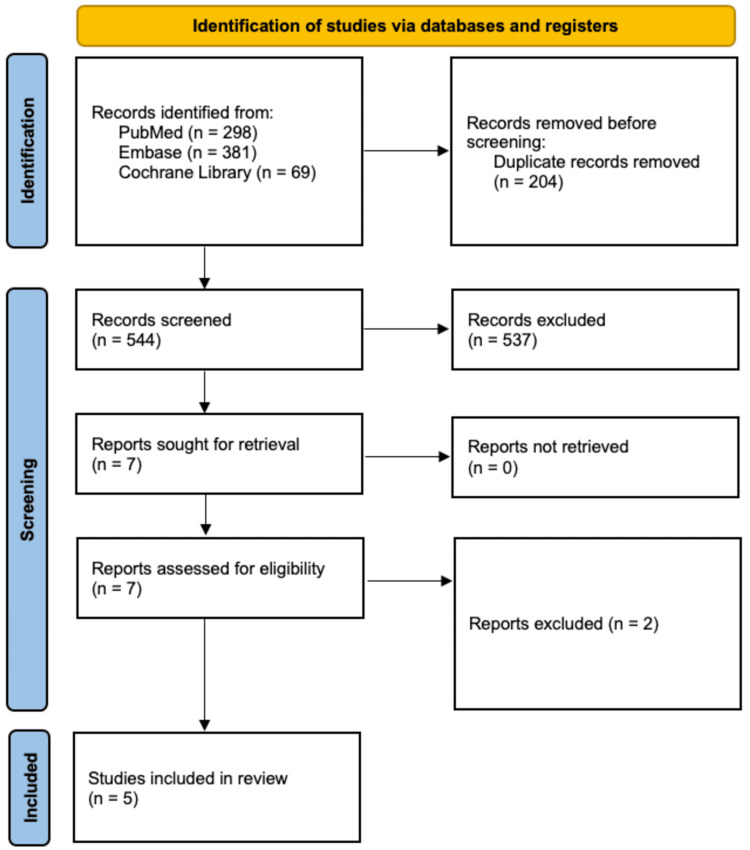 Figure 1
Figure 1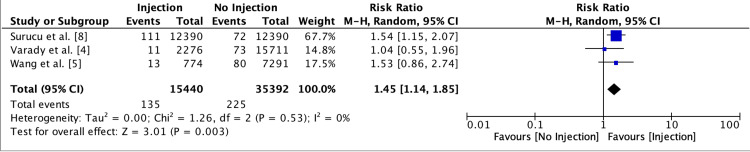 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4 Figure 5
Figure 5| Author | Study Design | MINORS Score | Patients (Female/Male) | Main Findings |
| Varady et al. [ | Patients were grouped into a control group which received no injections, and two groups which received an injection within 0-3 and 3-12 months of HA. Patients who received injections under FL vs. US guidance were evaluated separately. Postoperative infection was evaluated within 6 months of the HA procedure. | 19/24 | 0-3 months: 1262 (368/894) | For FL-guided injection, there was no significant difference in infection rate between the 0-3 month vs. Control group (P > 0.999) and the 3-12 month vs. Control group (P = 0.74). |
| 3-12 months: 1014 (340/674) | ||||
| For US-guided injection, there was no significant difference in infection rate between the 0-3 month vs. Control group (P = 0.76) and the 3-12 month vs. Control group (P > 0.999). | ||||
| Control: 15,711 (5814/9897) | ||||
| Wang et al. [ | Patients were grouped into a control group which received no injections, and three groups which received an injection within 0-3, 3-6, and 6-12 months of HA. Patients who were privately insured and those who were covered by Medicare were evaluated separately. Postoperative infection was evaluated within 6 months of the HA procedure. | 18/24 | 0-3 months: 339 (230/109) | For privately insured patients, the 0-3 month vs. control group had a significantly higher infection rate (P < 0.001), however, both the 3-6 month and 6-12 month groups compared to the control group did not have significant differences in infection rate (P = 0.285 and 0.396, respectively). |
| 3-6 months: 249 (168/81) | ||||
| 6-12 months: 186 (131/55) | For Medicare patients, the 0-3 month vs. control group had a significantly higher infection rate (P < 0.037); however, both the 3-6 month and 6-12 month groups compared to the control group did not have significant differences in infection rate (P = 0.172 and 0.195, respectively). | |||
| Control: 6846 (4295/2551) | ||||
| Surucu et al. [ | Patients were grouped in a control group which received no injections, and three groups which received an injection within 0-4, 4-8, and 8-12 weeks of HA. | 18/24 | 0-4 weeks: 3579 (2611/968) | Patients in the 0-4 week group had significantly greater odds of infection compared to the control group (P = 0.0005). Patients in both the 4-8 and 8-12 week groups had similar odds of infection compared to the control group (P = 0.1543 and 0.1352, respectively). Additionally, patients who received an injection vs. those who did not had a significantly higher rate of infection (P < 0.0001). |
| 4-8 weeks: 4759 (3426/1333) | ||||
| 8-12 weeks: 4052 (2383/1669) | ||||
| Control: 12,390 (9012/3387) | ||||
| Johnson et al. [ | Patients were grouped into a control group which received no injections and an injection group which received an injection within a year of HA. Injections were administered under US or FL guidance. The injection group was subdivided into those who received CSI or local anesthetic injections. Patients were evaluated at 1 and 5 years after HA. | 20/24 | Injection: 6511 (4488/2023); (CSI (3739) and Local Anesthetic (2749)) | Any injection vs. control group had significantly higher odds of repeat HA at 1 and 5 years (P < 0.001 for both), but not THA, infection, or new onset OA. |
| CSI vs. control group had significantly higher odds of repeat HA at 1 and 5 years (P < 0.001 for both), but not THA, infection, or new onset OA. | ||||
| Control: 1178 (563/615) | Local anesthetic vs. control group had significantly lower odds of repeat HA at 1 year (P < 0.001) but not at 5 years (P = 0.361). Local anesthetic vs. control group did not have significantly higher odds of THA, infection, or new onset OA at 1 or 5 years. | |||
| CSI vs. local anesthetic had significantly greater odds of repeat HA at 1 and 5 years (P < 0.001 for both), but not THA, infection, or new onset OA. | ||||
| Byrd et al. [ | Only patients who received injections within three months of HA were included. Injections were administered under US guidance and consisted of 1 mL (40 mg) methylprednisolone, 4 mL 1% lidocaine, and 4 mL 0.25% bupivacaine. | 7/16 | 500 (388/112) | There were zero postoperative cases of infection. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHip disorders and treatments · Orthopaedic implants and arthroplasty · Orthopedic Infections and Treatments
Introduction and background
Hip arthroscopy has increasingly been utilized over the past few decades for addressing intra-articular hip pathologies, such as femoroacetabular impingement, labral tears, and chondral lesions, yielding favorable outcomes. Prior to hip arthroscopy, intra-articular injections are often used by orthopedic surgeons as both diagnostic tools and therapeutic nonoperative treatments for hip pain unresponsive to other conservative management methods. As a diagnostic tool, relief of hip pain following an intra-articular injection helps isolate the primary pain source and guides surgeons in recommending arthroscopic intervention for underlying intra-articular pathology. Conversely, a lack of pain relief following an intra-articular injection may indicate extra-articular sources of hip pain [1-3]. An increasing number of surgeons and institutions now incorporate intra-articular injections to guide clinical decision-making in managing hip pain.
Despite their widespread use for diagnostic and therapeutic purposes, recent studies have reported an increased risk of infection when intra-articular injections are administered too close to elective surgeries, such as hip arthroscopy, generally within three months prior [4-8]. For example, a recent meta-analysis involving over 300,000 patients found that administering preoperative intra-articular steroid injections within three months of total knee arthroplasty (TKA) significantly increased the odds of periprosthetic joint infection (PJI) (P < 0.01) [9]. Similarly, another study indicated a significantly higher risk of PJI when intra-articular injections were given within three months prior to total shoulder arthroplasty (TSA), with elevated odds of infection at both three (P = 0.007) and six months (P = 0.001) postoperatively. However, when injections were administered three to 12 months before TSA, the odds of PJI were comparable to those without preoperative injections [10]. A systematic review of eight studies in 2020 evaluating the risk of infection in patients undergoing rotator cuff repair who were previously administered corticosteroid injections reported significantly higher odds of infection when injections were given within six months of the surgery or if ≥ 2 injections were administered within a year [11].
With the increasing use of intra-articular hip injections to guide clinical decision-making and determine candidacy for hip arthroscopy, it is crucial to assess the associated risks. Therefore, the primary objective of this systematic review is to evaluate whether preoperative intra-articular injections increase the risk of postoperative infection following hip arthroscopy. The secondary objective is to determine the safe interval for administering these injections before hip arthroscopy. We hypothesize that administering intra-articular injections closer to the time of hip arthroscopy increases the risk of postoperative infection.
Review
Methods
A search following guidelines established by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) was performed in three databases in April 2024: PubMed, Embase, and Scopus. Two authors identified all articles included in the study. The query was performed utilizing the Boolean search phrase “(hip AND arthroscop* AND injection).” There were no restrictions set to the search. Studies were included if they reported on postoperative infection in patients who received intra-articular injections prior to hip arthroscopy. Exclusion criteria included case reports, review articles, conference abstracts, studies performed in animals, articles not in English, expert opinions, letters to editors, and studies in which outcomes pertaining to preoperative intra-articular injections prior to hip arthroscopy were not specified.
The titles and abstracts of all studies were independently reviewed by two reviewers using the predetermined eligibility criteria. If they were not unanimous in their decision to include or exclude a study, a third reviewer was consulted. Next, the full text of select articles was independently reviewed by two reviewers, and again, if the reviewers were not unanimous in their decision, a third reviewer was consulted. All included articles underwent rigorous reference search to determine whether additional studies could be added to the systematic review. Study variables extracted from each article included study characteristics, patient demographic information, time between preoperative injection and subsequent hip arthroscopy, number of injections, and incidence of postoperative infection and revision.
The methodological quality of studies was assessed using the methodological index for non-randomized studies (MINORS) checklist. The MINORS items are scored 0 (not reported), 1 (reported but inadequate), or 2 (reported and adequate), with a maximum possible score of 16 for non-comparative studies (from eight categories) and 24 for comparative studies (from 12 categories). Two authors scored each article in the systematic review. Each author scored the article individually before reviewing their scores, and any discrepancies were resolved by re-reviewing the articles until a unanimous consensus was met.
Descriptive statistics (mean, percentage, standard deviation, range, median) are reported in this study when applicable and when available. A meta-analysis was performed to compare the risk of infection between patients who received injections prior to hip arthroscopy at various time points with those who received no prior injections. Forest plots were generated to depict overall significance. A P-value of less than 0.05 was considered statistically significant.
Results
Upon the initial search of the PubMed, Embase, and Cochrane Library databases, 748 studies were identified, with 204 duplicates removed. The remaining 544 studies underwent full title and abstract review, resulting in the removal of 537 studies based on our predetermined exclusion criteria. Seven studies underwent full-text review to determine eligibility. Two studies were excluded for not reporting on infection following hip arthroscopy in patients who received preoperative intra-articular injections or due to overlapping study periods with multiple studies from the same senior author and institution. Consequently, five studies were included in this systematic review. The PRISMA flow diagram illustrating our search strategy and article selection process is depicted in Figure 1.
PRISMA flow chart depicting the article selection processPRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses
All five studies had a retrospective design, with four of the five studies utilizing national administrative databases. Four studies had a level of evidence of III, while one study had a level of evidence of IV. In total, there were 58,576 patients (58.4% female) across the five studies. Table 1 provides a summary of the study design, MINORS score, number of patients, and main findings from each study.
Three studies compared the rates or odds of postoperative infection in hip arthroscopy patients who received intra-articular injections at various time points prior to hip arthroscopy with those who received no prior injections. Varady et al. [4] found that, when compared to the control group, there was no significant difference in the rate of infection when either fluoroscopic or ultrasound-guided injections were administered within zero to three or three to 12 months of hip arthroscopy. Conversely, Wang et al. [5] reported a significantly higher infection rate in patients receiving injections within zero to three months prior to hip arthroscopy, while those receiving injections three to six or six to 12 months before surgery had similar infection rates to the control group. Surucu et al. [8] assessed infection odds at smaller intervals and found significantly greater odds of infection in patients receiving injections zero to four weeks before surgery, but similar odds for those receiving injections four to eight or eight to 12 weeks before surgery compared to the control group.
The risk of infection was significantly higher in patients receiving any injection prior to hip arthroscopy compared to those with no injection (risk ratio = 1.45; 95% confidence interval = 1.14-1.85; P = 0.003; Figure 2). Specifically, the risk was higher in the group receiving injections within three months prior to surgery (risk ratio = 1.55; 95% confidence interval = 1.19-2.01; P = 0.001; Figure 3). There was no significant difference in infection risk for patients receiving injections more than three months prior to surgery compared to those with no injection (risk ratio = 1.05; 95% confidence interval = 0.56-1.99; P = 0.87; Figure 4). Similarly, the infection risk was not significantly different between patients receiving injections within versus greater than three months before surgery (risk ratio = 1.44; 95% confidence interval = 0.64-3.24; P = 0.37; Figure 5).
Forest plot depicting the risk of infection in patients receiving an injection any time prior to hip arthroscopy versus those receiving no injectionRefs. [4,5,8]
Forest plot depicting the risk of infection in patients receiving no prior injection versus those receiving an injection within three months of hip arthroscopy
Forest plot depicting the risk of infection in patients receiving no prior injection versus those receiving an injection more than three months prior to hip arthroscopyRefs. [4,5,8]
Forest plot depicting the risk of infection in patients receiving an injection within three months versus greater than three months prior to hip arthroscopyRefs. [4,5]
Johnson et al. [7] compared the odds of repeat hip arthroscopy, total hip arthroplasty (THA), infection, and new-onset osteoarthritis (OA) at one and five years following hip arthroscopy among patients receiving a prior corticosteroid injection, local anesthetic injection, or no injection. They found no significantly greater odds of infection, THA, or new-onset OA between any injection versus no injection, corticosteroid injection versus no injection, local anesthetic injection versus no injection, and corticosteroid injection versus local anesthetic injection at both one and five years post surgery. However, corticosteroid injections were associated with significantly greater odds of repeat hip arthroscopy compared to local anesthetic injections at both one and five years.
Byrd et al. [6] conducted a retrospective review of 500 consecutive hip arthroscopy patients who had received an intra-articular injection within three months prior to surgery. None of these patients developed postoperative surgical site infections.
Discussion
The primary findings of our study demonstrated that patients receiving an intra-articular injection within three months prior to hip arthroscopy had a significantly greater risk of postoperative infection, whereas those receiving an injection more than three months prior did not have a higher risk of infection. However, when comparing patients who received an injection within three months to those who received one more than three months prior, the risk of postoperative infection was similar. Additionally, patients receiving an injection at any time point prior to hip arthroscopy had a significantly higher risk of infection compared to those who received no prior injections.
The results of our meta-analysis align with findings from similar studies on other orthopedic procedures, such as joint arthroplasty and rotator cuff repair. Albanese et al. in their meta-analysis on the risk of PJI following total joint arthroplasty in patients who received preoperative corticosteroid injections found no association between PJI and TKA. However, they observed a statistically higher risk of PJI (odds ratio: 1.2, 95% confidence interval: 1.058-1.347, P = 0.045) if injections were administered within three months prior to THA [12]. Similarly, Lucenti et al., in their systematic review on infection risk in patients who received corticosteroid injections before TSA or shoulder arthroscopy, determined that the risk of postoperative infection was greater when injections were given within three months of surgery [13].
It is important to emphasize that the timing of the injection is not the sole risk factor for postoperative infection. Other factors, including obesity, sex, smoking, and alcohol use, also impact outcomes. Our systematic review included three studies for meta-analysis, which had variations in baseline patient demographics, comorbidities, and additional risk factors. These differences, along with the timing of the injection, may have contributed to postoperative infection rates.
This study should be considered in the context of its limitations. First, based on our strict inclusion and exclusion criteria, we were limited to only five included studies in the systematic review, of which only three were able to be included in the meta-analysis. Though the meta-analysis encompassed a large number of patients, since they were derived from only three studies, the generalizability of the results may be limited. Second, data on factors such as injection technique, concentration, volume, and contents were either incompletely presented or not provided by the included studies, introducing potential confounding bias. Finally, all included studies had a retrospective design. Although it would be pragmatically challenging to address the research question through studies with stronger designs, such as randomized controlled trials, the use of large administrative databases is warranted to provide more robust evidence.
Conclusions
Patients undergoing hip arthroscopy who previously received intra-articular injections may face a statistically higher risk of developing postoperative infection, particularly when the injection is administered within three months prior to the procedure. Therefore, to mitigate the increased risk of infection, surgeons should avoid administering intra-articular injections to patients scheduled for hip arthroscopy within the subsequent three months.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Diagnostic intra-articular injection with provocative functional testing predicts patient-reported outcomes following hip arthroscopy: a prospective investigation J Hip Preserv Surg Haws BE Condidorio CG Adler KL Giordano BD 158164920223599203210.1093/jhps/hnac 025PMC 9389908 · doi ↗ · pubmed ↗
- 2Preoperative intra-articular steroid injections as predictors of hip arthroscopy: 2-year outcomes Orthop J Sports Med Mujahed T Hassebrock JD Makovicka JL Pollock JR Wilcox JG Patel KA Economopoulos KJ 9202110.1177/23259671211053817 PMC 864727434881337 · doi ↗ · pubmed ↗
- 3Utility of intra-articular hip injections for femoroacetabular impingement: a systematic review Orthop J Sports Med Khan W Khan M Alradwan H Williams R Simunovic N Ayeni OR 2325967115601030320152653539510.1177/2325967115601030 PMC 4622294 · doi ↗ · pubmed ↗
- 4Image-guided intra-articular hip injections and risk of infection after hip arthroscopy Am J Sports Med Varady NH Amen TB Abraham PF Chopra A Freccero DM Smith EL Martin SD 248224884920213416117410.1177/03635465211022798 · doi ↗ · pubmed ↗
- 5The timing of hip arthroscopy after intra-articular hip injection affects postoperative infection risk Arthroscopy Wang D Camp CL Ranawat AS Coleman SH Kelly BT Werner BC 198819943320172880091810.1016/j.arthro.2017.06.037 · doi ↗ · pubmed ↗
- 6The safety of hip arthroscopy within 3 months of an intra-articular injection J Bone Joint Surg Am Byrd JW Bardowski EA Civils AN Parker SE 1467146910120193143665410.2106/JBJS.19.00147 · doi ↗ · pubmed ↗
- 7Injections prior to hip arthroscopy are associated with increased risk of repeat hip arthroscopy at 1 and 5 years Arch Orthop Trauma Surg Johnson AH Brennan JC Maley A Levermore SB Turcotte JJ Petre BM 82382914420243810305210.1007/s 00402-023-05164-7 · doi ↗ · pubmed ↗
- 8Corticosteroid injections administered within 4 weeks prior to hip arthroscopy are associated with higher rates of postoperative infection [IN PRESS]Arthroscopy Surucu S Halperin SJ Monahan PF Gillinov SM Lee MS Grauer JN Jimenez AE 202410.1016/j.arthro.2024.01.01638311263 · doi ↗ · pubmed ↗