A 24-Year-Old Male Patient With an Ostium Secundum Complex Atrial Defect Secondary to a Perforated Aneurysm With Inferior Vena Cava Agenesis
Atl Simon Arias Rivera, Katherine Rubio, Lizbeth S Gonzalez Solano, Mauricio Damian Gomez Gonzalez, Alain Ledu Lara, Manuel Carrillo Cornejo, Moises C Calderon Abbo

TL;DR
A 24-year-old man with a rare heart defect and missing inferior vena cava underwent successful open-heart surgery and made a full recovery.
Contribution
This case report highlights a rare combination of congenital heart defects and their successful surgical management.
Findings
The patient had an ostium secundum atrial defect secondary to a perforated aneurysm and inferior vena cava agenesis.
Open-heart surgery with a pericardium patch successfully repaired the defect with no residual shunts postoperatively.
The patient showed favorable recovery and no complications during follow-up at one and three months.
Abstract
The article describes a successful clinical outcome in the case of a 24-year-old male with a diagnosis of an ostium secundum atrial defect secondary to a perforated aneurysm associated with vena cava agenesis. During hospitalization, an echocardiogram revealed the presence of ostium secundum inter-atrial communication with a left to right shunt, a left ventricular ejection fraction (LVEF) of 60%, and mild pulmonary hypertension, measured at 40 mmHg. CT imaging showed anomalous dilation of the azygos vein (16.8 mm), associated with interruption of the vena cava in the intrahepatic and adrenal portion, continuing through the azygos system and draining into the superior vena cava. Open-heart surgery was performed with pericardium patch placement on the defect. Postoperative transthoracic echocardiography revealed a tracking of the interatrial septum, with adequate placement of the surgical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
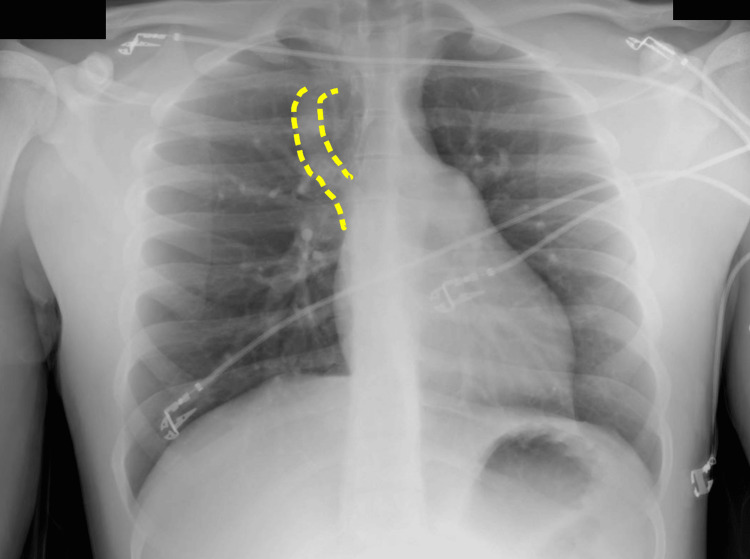 Figure 1
Figure 1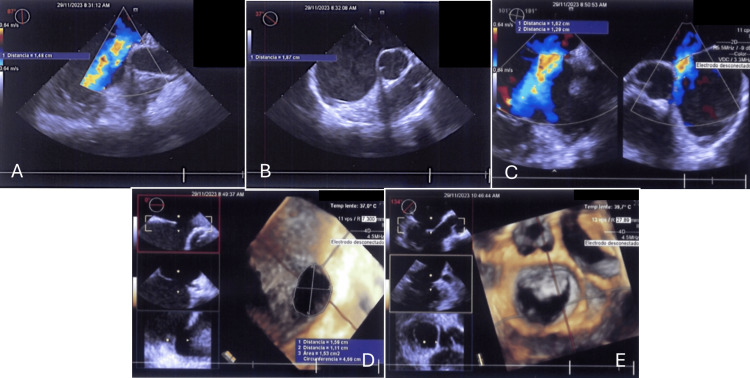 Figure 2
Figure 2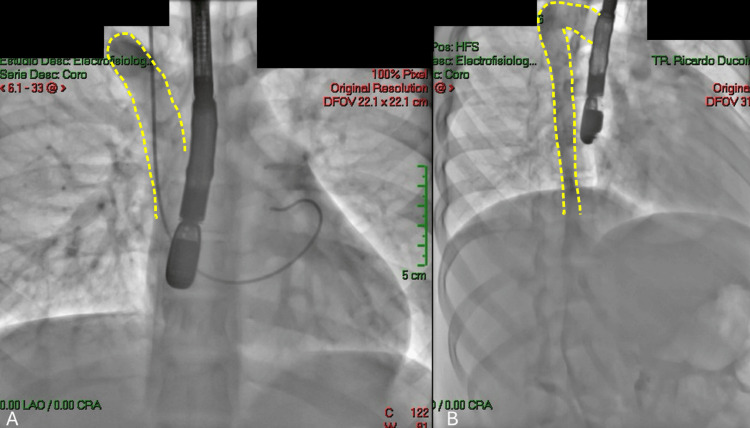 Figure 3
Figure 3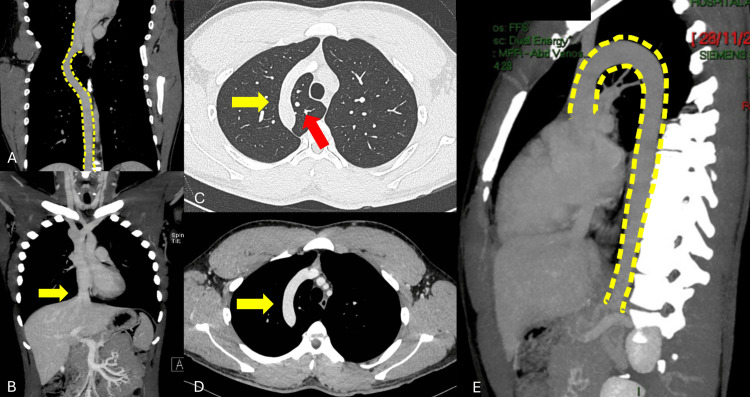 Figure 4
Figure 4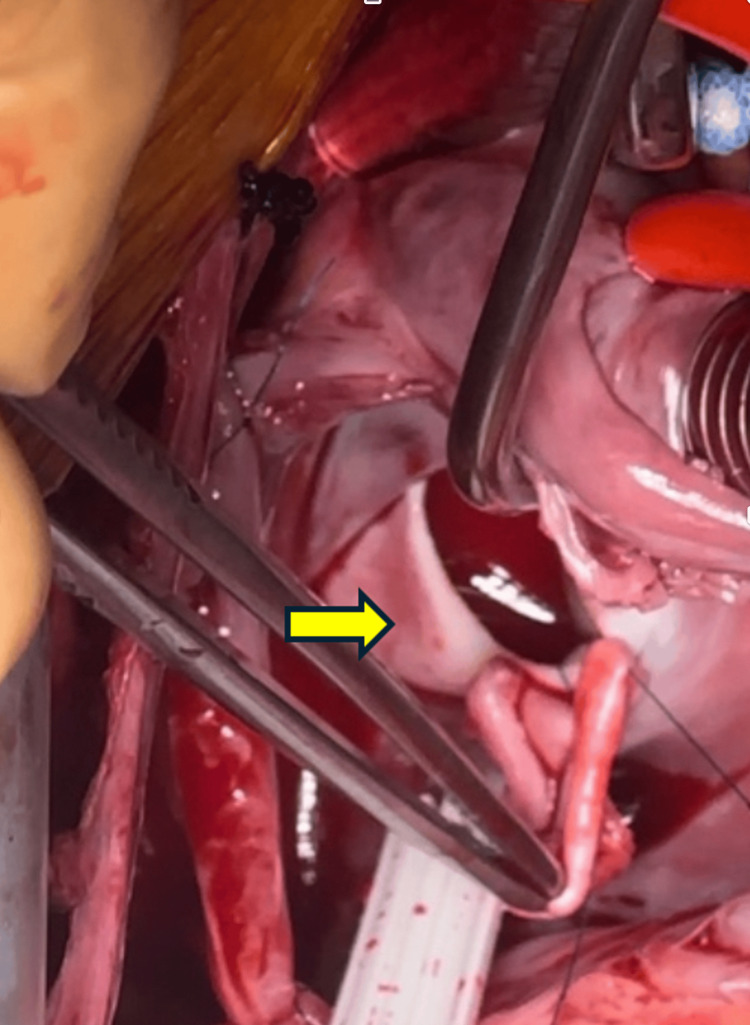 Figure 5
Figure 5 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Heart Disease Studies · Coronary Artery Anomalies · Vascular anomalies and interventions
Introduction
Congenital heart disease (CHD) encompasses structural abnormalities of the heart that are present at birth and arise in the fetus during embryonic development in the uterus. Approximately half a million adults in the United States (US) are affected with congenital cardiac disease and approximately 1% of children are born with congenital cardiac problems as a result of genetic or chromosomal disorders [1].
Although CHD is mostly diagnosed during the neonatal period, or early childhood, diagnosis of these conditions during adulthood isn’t unheard of. Atrial septal defect (ASD) is the primary type of CHD that is first diagnosed in adulthood. The estimated prevalence of ASDs in adults is 0.88 per 1000 patients [2].
The term ASD includes a group of abnormalities that allow communication between left and right atria. The location of the defect categorizes ASD into five types: patent foramen ovale (PFO), ostium secundum defect (OSD), ostium primum defect (OPD), sinus venosus defect (SVD), and coronary sinus defect (CSD) [3].
Secundum atrial septal defect refers to the communication within the fossa ovalis. It is considered the most prevalent cardiac abnormality present at birth that continues into adulthood (80% of cases). It is responsible for around 30% of newly diagnosed cases. It occurs due to a lack of tissue near the fossa ovalis [3].
OPD refers to the initial opening or entrance. In comparison to OSD, SVD anomalies are more frequently observed in the superior portion of the embryologic sinus venosus and are associated with partial anomalous pulmonary venous return. CSD is a rare form of ASD that is typically difficult to diagnose. However, an exposed coronary sinus can be seen when agitated saline contrast bubbles originating from the left upper extremities enter the left atrium (LA) prior to the right atrium (RA) [3-4].
Frequently the history of the patient uncovers a progressive alteration in exercise capacity, typically described as modest, and sometimes obvious difficulty in breathing during physical effort. While ASD is typically characterized by a gradual clinical progression and lack of symptoms in patients, its detection helps prevent time-related consequences, including arrhythmias, thrombosis, right heart failure, and pulmonary arterial hypertension (PAH) [5].
We present a case of a 24-year-old male patient with a large interatrial defect secondary to a perforated aneurysm presented with inferior vena cava (IVC) agenesis.
Case presentation
A 24-year-old male patient presented with two months of evolution with progressive dyspnea and multiple episodes of orthopnea at night. The symptoms progressed with daily episodes accompanied by chest palpitations and precordial pain exacerbated with physical activities. Upon arrival at the emergency department, the physical exploration showed a wide, fixed splitting of S2. The electrocardiogram sinus rhythm without enlargement of cardiac cavities. The diagnostic evaluation began with an echocardiogram and a chest X-ray that showed images suggesting the prominence of the azygos vein (Figure 1). The transthoracic echocardiogram showed the presence of ostium secundum interatrial communication of 1.5 cm x 1.2 cm with a left to right shunt from a perforated atrial aneurysm, a left ventricular ejection fraction (LVEF) of 60%, and mild pulmonary hypertension of 40 mmHg (Figure 2). The patient was programmed for a percutaneous closure intervention with an Amplatzer device, which failed because of a vascular variant with evidence of inferior vena cava agenesis (Figure 3). Subsequent to these findings, a contrasted thoracoabdominal computed tomography (CT) was performed. The CT showed an anomalous dilation of the azygos vein (16.8 mm), associated with interruption of the inferior vena cava in the intrahepatic and adrenal portion, with continuation through the azygos system and drainage of the superior vena cava. The suprahepatic veins drain to the right atrium with the rest of the study with no abnormalities (Figure 4). Based on these findings, the patient was scheduled for open-heart surgery.
Posterior anterior (PA) chest X-rayAorta with normal course and density. Image suggesting prominence of the azygos vein (yellow intermittent line). Both pulmonary hilia without evidence of lesions. The cardiac silhouette preserves shape, size, and contours.
Preoperative transthoracic echocardiogramA-C: Ostium secundum-type atrial septal defect, with shunts from left to right, with agenesis of the inferior vena cava. D-E: Inter-atrial septum with a defect of 1.5 cm x 1.2 cm, with shunt from left to right, with a posterior edge of 1.6 cm, an upper edge of 0.6 cm, an inferior edge of 1.1 cm, and a short aortic edge of 4 mm.
Catheterization performed via the internal jugular veinA-B: Presence of a prominent azygos vein (yellow intermittent line) with a catheter line through a jugular internal vein approach localized in the right atrium.
Contrasted thoracoabdominal computed tomographyA-B: Anomalous dilation of the azygos vein (16.8 mm) (intermittent yellow line), associated with interruption of the inferior vena cava in the intrahepatic and adrenal portion (yellow arrow). C-D: Presence of dilation of the azygos vein (yellow arrow) in a transversal plane with the presence of an azygos pulmonary lobe (red arrow). E: Continuation through the azygos system (intermittent yellow line) and drainage of the superior vena cava.
A supine position was chosen for the total sternotomy and the thymus was posteriorly removed without any complications. The pericardium was opened, finding dilation of the right cavities, heparin was administered, and cardiopulmonary bypass (CPB) was initiated with a single venous cannula. The venous cannula was placed in the superior vena cava and the suprahepatic veins that make up the vestige of the inferior cava were clamped.
The patient was cooled to relative hypothermia, the aorta was clamped and cardioplegia was initiated. The right atrium was opened, finding the defect of 2.5 x 2 cm, which was closed with a pericardial patch (Figure 5). The cardiac cavities were purged, the right auriculectomy was closed posteriorly, and the aorta was unclamped, initiating spontaneous heartbeating. The patient was then rewarmed, and we exited the CPB with decannulation. Epicardial pacing electrodes and drains were placed in the mediastinum and left pleura. Total aortic clamping was 37 min, and cellular recovery hemodiafiltration was used during surgery. The postoperative transthoracic echocardiogram evidenced a tracking of the interatrial septum, observing the adequate placement of the surgical patch without evidence of residual short circuits. A contrast echocardiogram with agitated saline solution is performed, revealing no evidence of a residual defect in the atrial septum (Figure 6).
Image of ASD in the patient's heartInteratrial defect of 2.5 x 2 cm with the presence of a forceps angle in the middle defect (yellow arrow)ASD: atrial septal defect
Transesophageal echocardiogram in the operating roomA: Contrasted echocardiogram is performed with agitated saline, without evidence of a residual defect in the septum or short circuits due to this approach. B-E: Appropriate placement of the patch, without evidence of residual short circuits. Pulmonary veins are observed without obstruction and the superior vena cava is permeable. The systolic and diastolic function of the left ventricle, without deterioration and without observing complications, associated with the procedure.
The postoperative recovery of the patient was without any complication, with a total of five days of hospital stay. Drains in the mediastinum and left pleura were removed on the third postoperative day.
We performed outpatient monitoring for the first and third months without any complications during the physical exploration and echocardiogram imaging.
Discussion
Sinus venosus type ASD is an uncommon heart abnormality that typically occurs at the entrance of the superior vena cava (SVC) into the right atrium (RA). It is commonly accompanied by abnormal draining of the right pulmonary veins into the RA. The presence of an IVC-type sinus venosus atrial septal defect with an overriding inferior vena cava is an exceptionally uncommon occurrence. The categorization of ASD is determined by the anatomical position within the interatrial septum, the process of embryogenesis, and the size [5].
Inferior SVDs are rare imperfections located in the inferior portion of the atrial septum near the entrance of the IVC. These defects result from abnormal development of the inferior sinus venosus. Abnormal development of this portion of the atrial septum results in an overriding IVC that communicates with both the right and left atria and has the potential for abnormal pulmonary venous return [6].
In our case, the patient had an atrial septal defect of OSD with agenesis of the inferior vena cava being a particularly difficult case to manage via endovascularly. The association between the type of atrial defect of our patient with the vascular variant of agenesis of the IVC is rare compared to the associations with SVDs.
Peacock and Waggstaffe provided descriptions of the pathophysiology of SVD in 1858 and 1868, respectively. In 1956, Ross provided the initial description of the sinus venosus defect, characterizing it as the partial failure of the sinus venosus to merge completely with the right atrium. However, it should be noted that this anomaly is not considered a genuine atrial septal defect [7-9]. The most frequent initial symptom that presents itself is exercise intolerance, which manifests as exertional dyspnea or weariness. Untreated, this illness can advance to Eisenmenger's syndrome and cardiac failure. Untreated ASD has a death rate of 25%. Current guidelines advise that all patients with hemodynamically significant ASD should have ASD closure, irrespective of symptoms, in order to prevent long-term consequences such as atrial arrhythmias, pulmonary hypertension, and/or paradoxical embolism [10-12].
The transcatheter closure is a less invasive approach compared to open surgery being the treatment of choice in the majority of cases. This approach is not indicated in the case of a complex ASD. A complex atrial septal defect (ASD) is characterized by defects larger than 38 mm in diameter and/or defective rims other than the anterosuperior rim. These types of defects are typically not suitable for closure using transcatheter methods and are instead recommended for surgical intervention. Device closure may be contraindicated in cases, where there are additional factors such as young age or low weight, multiple abnormalities, comorbidities, and concomitant heart anomalies [4,13].
The patient in our case had an interatrial size defect of 1.5 cm x 1.2 cm, with a posterior edge of 1.6 cm, upper edge of 0.6 cm, inferior edge of 1.1 cm, and short aortic edge of 4 mm. For the dimensions of the atrial defect, an open surgical procedure was indicated instead of the transcatheter closure.
If the transcatheter closure is not recommended due to certain factors, the alternative treatment option is open surgery. The mortality rate for this procedure is approximately 1% in patients who do not have any serious underlying health conditions. Additionally, less than 7% of patients experience substantial complications following the surgery. Postoperative arrhythmia is the most frequently occurring complication. Surgical closure is the recommended treatment for sinus venosus, primum, coronary sinus defect, and secundum atrial septal defects (ASDs) that cannot be closed using transcatheter methods. The indications for ASD closure are the presence of right heart dilatation without irreversible pulmonary hypertension, as well as the occurrence of paradoxical emboli [2,14].
Currently, the surgery is conducted using a partial mini-sternotomy, which involves making a small incision in the middle of the chest, and a thoracotomy, which can be done either on the right side of the chest or through a vertical incision in the axilla. We conducted a mini-sternotomy in this case to get a more favorable cosmetic outcome [15].
The most favorable result is achieved when the repair is performed before the age of 25. If the operation is done in a younger population, the probability of acquiring late cardiac failure, stroke, and atrial fibrillation is lower in comparison to older patients. Successful closure of a condition results in the reversal of right ventricular remodeling, which is inversely related to the age of the patient. This leads to increased functional class, cardiac output, and exercise capacity, regardless of the patient's age [15].
Conclusions
ASD secundum is the most common congenital heart defect (CHD). In some cases, the patient may remain asymptomatic in childhood and adolescence with symptoms appearing in adulthood. In the majority of instances, transcatheter closure of secundum ASD has become the preferred method over surgical closure. In scenarios where transcatheter closure is contraindicated, open surgery is the treatment of choice. These patients should be promptly treated to prevent major complications like right ventricular dysfunction and have an adequate postoperative follow-up by a multidisciplinary team.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Congenital heart disease: causes, diagnosis, symptoms, and treatments Cell Biochem Biophys Sun R Liu M Lu L Zheng Y Zhang P 8578607220152563834510.1007/s 12013-015-0551-6 · doi ↗ · pubmed ↗
- 2Atrial septal defect in adulthood: a new paradigm for congenital heart disease Eur Heart J Brida M Chessa M Celermajer D 26602671432022 https://doi.org/10.1093/eurheartj/ehab 6463453598910.1093/eurheartj/ehab 646 · doi ↗ · pubmed ↗
- 3Changing epidemiology of congenital heart disease: effect on outcomes and quality of care in adults Nat Rev Cardiol Liu A Diller GP Moons P Daniels CJ Jenkins KJ Marelli A 126137202023 https://doi.org/10.1038/s 41569-022-00749-y 3604522010.1038/s 41569-022-00749-y · doi ↗ · pubmed ↗
- 4Congenital heart disease in adults Medicine, Volume Panagiota M Samantha F 587592502022
- 5Undiagnosed inferior vena cava type of sinus venosus atrial septal defect in a middle-aged woman: a rare case report J Clin Ultrasound Ghaemian A Nabati M Shokri M 5658482020 https://doi.org/10.1002/jcu.227673136417310.1002/jcu.22767 · doi ↗ · pubmed ↗
- 6Anatomical criteria for the diagnosis of sinus venosus defects Heart al Zaghal AM Li J Anderson RH Lincoln C Shore D Rigby ML 298304781997 https://doi.org/10.1136/hrt.78.3.298939129410.1136/hrt.78.3.298PMC 484934 · doi ↗ · pubmed ↗
- 7Malformations dependent on arrest of development at an early period of fetal life On Malformations of the Human Heart Peacock TB 2425 London, UK John Churchill 1858 https://www.barnesandnoble.com/w/on-malformations-of-the-human-heart-etc-thomas-bevill-peacock/1136025389
- 8Two cases of free communication between the auricles, by deficiency of the upper part of the septum auricularum Trans Pathol Soc Lond Waggstaffe WW 9198191868