Successful prevention of balloon dilatation after complete circumferential endoscopic submucosal dissection including long-segment Barrett’s esophagus
Kenichiro Okimoto, Tomoaki Matsumura, Keisuke Matsusaka, Yuki Ohta, Takashi Taida, Jun Kato, Naoya Kato

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
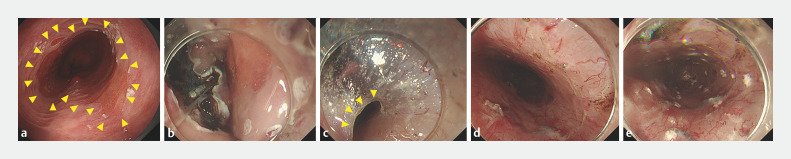 Fig. 1
Fig. 1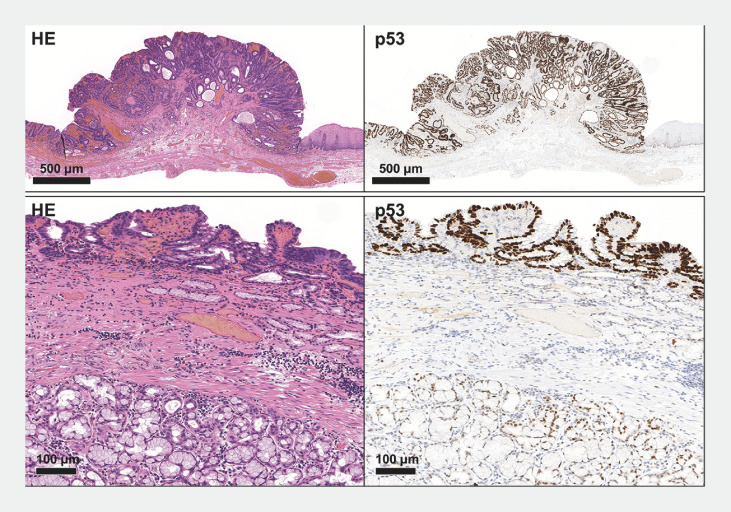 Fig. 2
Fig. 2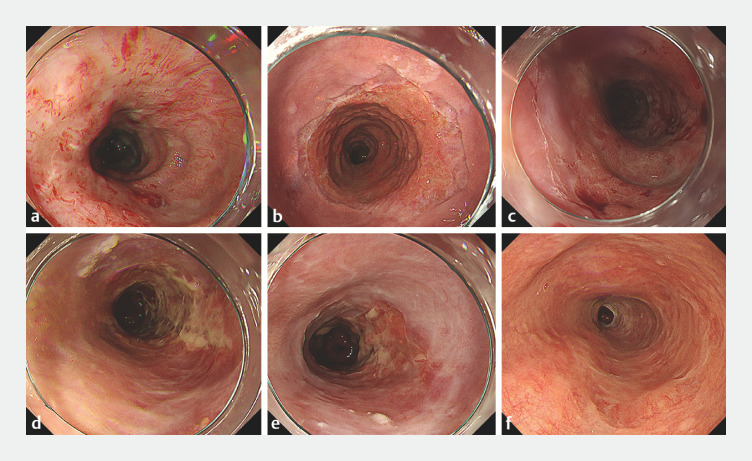 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Gastric Cancer Management and Outcomes · Esophageal Cancer Research and Treatment
Triamcinolone acetonide (TA) injection into submucosa is useful for prevention of stricture after esophageal endoscopic submucosal dissection (ESD) 11 . However, despite attempts with steroid use, complete circumferential esophageal ESD still leads to high stricture rates (36.4% to 85.7% 22 33 44 ). Although endoscopic balloon dilatation (EBD) is often necessary for stricture relief, it carries the risk of perforation 22 . In addition, in long-segment Barrett’s esophagus (BE) with Barrett's esophageal adenocarcinoma (BEA), post-ESD ulcers can be too long, making EBD challenging. Thus, alternative stricture methods preventing EBD are needed.
Here we present a case of successful prevention of EBD after a circumferential ESD for BEA in long-segment BE (longitudinal length of resected area was 12 cm endoscopically) with intensive TA injections ( Video 1Video 1 ). ESD utilized MucoUp (Seikagaku, Tokyo, Japan and Boston Scientific Japan, Kanagawa, Japan) with indigo carmine, 1.5-mm DualKnife J (Olympus Medical Systems, Tokyo, Japan), and the clip-and-line method 55 . En bloc resection, including the entire long-segment BE (Prague classification C8M9), was performed ( Fig. 1. Fig. 1 ). The pathological finding was BEA with unclear horizontal margin and negative vertical margin ( Fig. 2. Fig. 2 ).
Weekly intensive triamcinolone acetonide injections were beneficial for preventing stricture in complete circumferential esophageal endoscopic submucosal dissection.Video 1Video 1
Fig. 1 The details of endoscopic submucosal dissection (ESD). a The patient was diagnosed with circumferential Barrett's adenocarcinoma with long-segment Barrett’s esophagus (BE) (C8M9 according to the Prague classification). The yellow arrows indicate the proximal boundary of long-segment BE. b ESD was performed with the clip-and-line method. c ESD was performed by creating a submucosal tunnel. The yellow arrows indicate the edge of the submucosal tunnel. d Immediately after ESD, en bloc resection was performed including the entire long-segment BE. The longitudinal length of the post-ESD defect measured endoscopically was up to 12 cm from the oral to the anal side. e A total of 100 mg of triamcinolone acetonide (TA) was locally injected into the remaining submucosa.
Fig. 2 Pathological findings of the resected specimen. Histological photograph of an adenocarcinoma at the esophagogastric junction. Atypical glandular epithelium forms irregular tubules, creating polypoid, protruding lesions. Immunostaining shows a mutant pattern of p53 overaccumulation. Meanwhile, a flatly spreading adenocarcinoma is observed around the protrusions. Submucosal esophageal glands in the columnar epithelium region are identified, suggesting an adenocarcinoma arising in Barrett's esophagus.
TA (KENACOLT-A 50 mg/5 mL; Bristol Myers Squibb, Tokyo, Japan) was diluted to 5 mg/mL with normal saline. A 26-gauge 4-mm needle (SG-A 26G FE 4 mm 2200 mm; TOP Corporation, Tokyo, Japan) was used for injection. TA injection into the submucosa, starting immediately post-ESD, was performed at intervals of 0.5 mL (TA 2.5 mg), preventing injury to the muscularis propria. Subsequent injections occurred 3 days post-ESD and then weekly for 21 weeks, with additional injections on weeks 23 and 25, totaling 25 sessions. A total of 50–100 mg TA was administered in each session. At 40 weeks post-ESD, complete epithelialization without stricture was achieved ( Fig. 3. Fig. 3 ).
Fig. 3 The healing process of the post-ESD ulcer. The epithelialization progressed in chronological order from Fig. 3. Fig. 3 a–f . A total of 50 mg or 100 mg of TA was locally injected into the regenerating submucosal layer from Fig. 3. Fig. 3 a–e , respectively. a 1 week after ESD (3rd local injection of TA). b 4 weeks after ESD (6th local injection of TA). c 8 weeks after ESD (10th local injection of TA). d 12 weeks after ESD (14th local injection of TA). e 20 weeks after ESD (22nd local injection of TA). f 40 weeks after ESD. Complete epithelialization without any stricture was achieved, and a φ9.8-mm scope (GIF-H290T; Olympus Medical Systems, Tokyo, Japan) passed easily.
Weekly intensive TA injections alone were beneficial for preventing stricture in complete circumferential esophageal ESD even if the resected area was long.
Endoscopy_UCTN_Code_TTT_1AO_2AO
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hashimoto S Kobayashi M Takeuchi M The efficacy of endoscopic triamcinolone injection for the prevention Gastrointest Endosc 2011741389139310.1016/j.gie.2011.07.07022136782 · doi ↗ · pubmed ↗
- 2Iizuka T Kikuchi D Hoteya S Effectiveness of modified oral steroid administration for preventing esophageal stricture after entire circumferential endoscopic submucosal dissection Dis Esophagus 20183110.1093/dote/dox 14029444278 · doi ↗ · pubmed ↗
- 3Kadota T Yoda Y Hori K Prophylactic steroid administration against strictures is not enough for mucosal defects involving the entire circumference of the esophageal lumen after esophageal endoscopic submucosal dissection (ESD)Esophagus 20201744044732172461 10.1007/s 10388-020-00730-z · doi ↗ · pubmed ↗
- 4Minamide T Kawata N Maeda Y Clinical outcomes of endoscopic submucosal dissection for superficial circumferential esophageal squamous cell carcinoma Gastrointest Endosc 20239723224010.1016/j.gie.2022.09.02736228694 · doi ↗ · pubmed ↗
- 5Oyama T Counter traction makes endoscopic submucosal dissection easier Clin Endosc 20124537537810.5946/ce.2012.45.4.37523251884 PMC 3521938 · doi ↗ · pubmed ↗