Combined endoscopic management of a postoperative rectocutaneous fistula after cystectomy using modified percutaneous endofistular and transanal endoluminal vacuum therapy
Ahmed Alwali, Clemens Schafmayer, Imad Kamaleddine

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1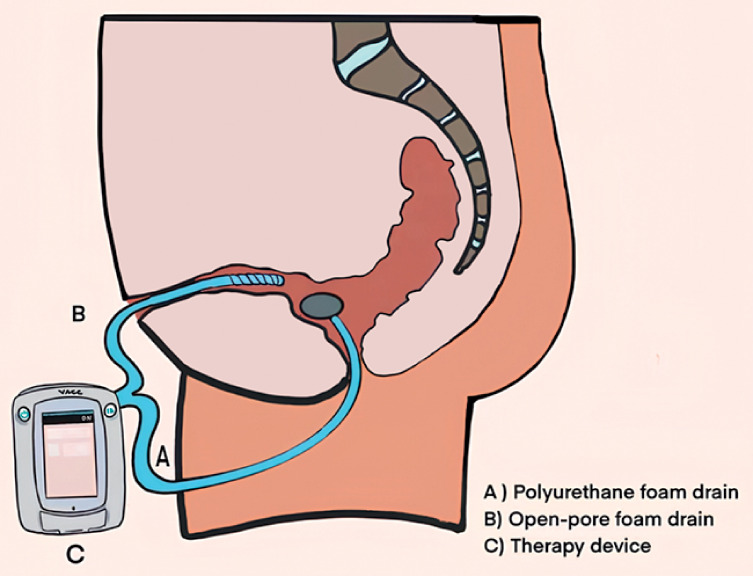 Fig. 2
Fig. 2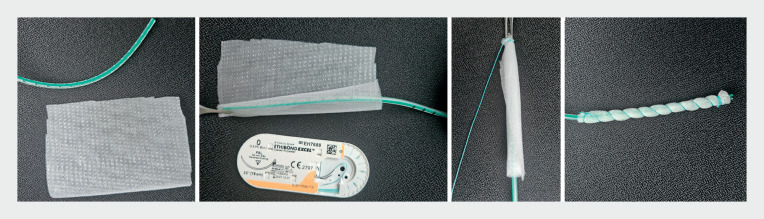 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiverticular Disease and Complications · Anorectal Disease Treatments and Outcomes · Ureteral procedures and complications
A 79-year-old man presented with a transanal purulent discharge following cystectomy with rectal injury 10 months previously. At that time, surgical closure with suturing of the rectal defect had been performed, along with the creation of a colostomy. Endoscopic examination revealed a perforation 5 cm from the anal verge. An attempt was made to close the perforation with an over-the-scope clip; however, during the follow-up endoscopy, a significant defect was observed in rectum, with an accompanying large cavity. The patient then underwent 6 weeks of inpatient therapy with endoluminal transanal vacuum therapy, which resulted in a reduction of the cavity size. The patient returned to us 4 months later with persistent purulent discharge from the caudal pole of the laparotomy scar and anus ( Fig. 1. Fig. 1 ). Endoscopic examination revealed a defect in the anterior wall of the rectum 5 cm from the anal verge, with a cavity full of pus and a rectocutaneous fistula. We opted for a combined approach involving endoluminal and endofistular vacuum therapy for 3 weeks in the hospital setting ( Fig. 2. Fig. 2 ).
Fig. 1 A computed tomography image showing a pararectal cavity with a complex rectocutaneous fistula.
Fig. 2 Schematic of the combined modified percutaneous endofistular and transanal endoluminal vacuum therapy.
Endoscopic vacuum therapy was initiated using an open-pore polyurethane foam drain (EndoSponge; B. Braun, Melsungen, Germany) placed transanally into the cavity, along with a customized open-pore film drain (Suprasorb CNP; Lohmann & Rauscher, Rengsdorf, Germany) inserted through the skin ( Fig. 3. Fig. 3 ) 11 . Suction of –125 mmHg was applied (ACTIV.A.C; KCI, San Antonio, Texas, USA) ( Video 1Video 1 ).
Fig. 3 Photographs showing the creation of an open-pore film drain, which involves wrapping a strip of double-layered open-pore film around a small drainage tube and securing it in place with a suture.
The combined endofistular and endoluminal endoscopic management of a postoperative complex rectocutaneous fistula after cystectomy.Video 1Video 1
Owing to the patientʼs preference for outpatient therapy, we continued therapy with outpatient percutaneous endofistular vacuum therapy, as previously described, changed twice weekly for an additional 3 weeks, progressively shortening the drain length with each adjustment. Upon follow-up examination 3 days later, the fistula had completely closed, and the pararectal cavity could no longer be visualized.
Endofistular vacuum therapy represents an effective method for the management of complex rectocutaneous fistulas, serving as a valuable adjunctive technique in the treatment of challenging cases.
Endoscopy_UCTN_Code_TTT_1AQ_2AG
The reference list from the paper itself. Each links out to its DOI / PubMed record.