Ligation-assisted endoscopic full-thickness resection combined with preloaded sutures for tiny mesenchymal tumors of the gastric fundus
Minna Zhang, Peng Shen, Wenzhuo Zhao, Weijie Dai, Xiaozhong Yang, Rui Xie

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
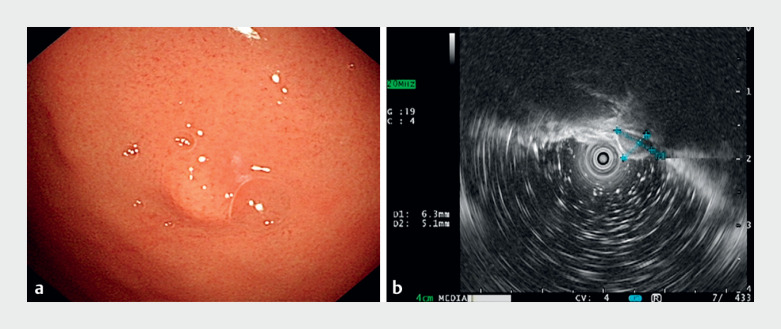 Fig. 1
Fig. 1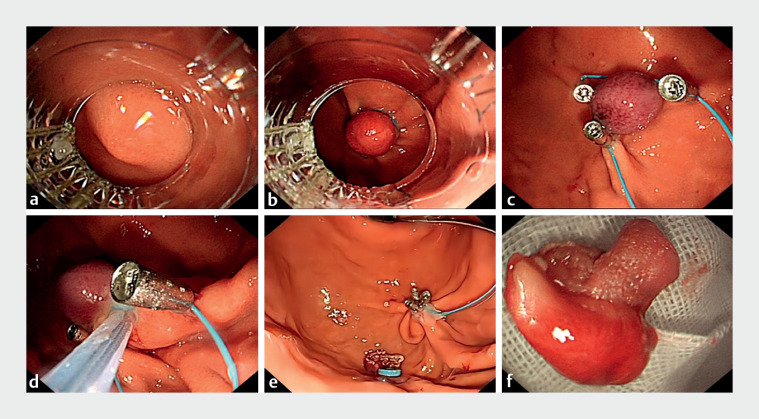 Fig. 2
Fig. 2- —Scientific Research and Innovation Team of Huaiʼan First Peopleʼs Hospital
- —Jiangsu Provincial Medical Key Discipline Cultivation Unit
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal Tumor Research and Treatment · Gastric Cancer Management and Outcomes · Gastrointestinal disorders and treatments
Gastrointestinal stromal tumors (GISTs) are the most prevalent tumors of mesenchymal tissue origin in the gastrointestinal tract 11 . Currently, the treatment of small GISTs (≤2 cm) and micro-GISTs (<1 cm) remains controversial. Endoscopic full-thickness resection (EFTR) is indicated for microscopic GISTs originating from the intrinsic muscularis propria, facilitating thorough tumor removal and minimizing the risk of dissemination 22 . The fundus of the stomach is one of the commoner sites for GISTs, and performing EFTR here requires high levels of endoscopic skill and, because of the small size of the tumor, it is very easy for it to fall into the abdominal cavity after the final resection 33 . To overcome this challenge, we used a transparent cap-assisted endoscopic full-thickness ligation (EFTR-L) technique combined with preloaded sutures ( Video 1Video 1 ), which allowed not only complete tumor resection and rapid specimen recovery, but also the prevention of intraoperative bleeding and perforation by use of the preloaded sutures.
A transparent cap-assisted endoscopic full-thickness ligation technique combined with preloaded sutures is used to resect a tiny mesenchymal tumor in the gastric fundus.Video 1Video 1
A 45-year-old man was found to have a 0.7-cm hemispherical bulge on the fundus of the stomach during gastroscopy ( Fig. 1. Fig. 1 a ). Endoscopic ultrasound suggested that the lesion was a hypoechoic mass of submucosal intrinsic muscular layer origin in the gastric fundus ( Fig. 1. Fig. 1 b ). With the EFTR-L approach, we first drew the lesion into the lancing cap with forceful suction ( Fig. 2. Fig. 2 a ). Localized ligation of the lesion was performed using a lancing device to form a pseudo-polypoid bulge ( Fig. 2. Fig. 2 b ). The ligature ring was then removed and three metal clips were pre-positioned around the tumor with nylon cords to form the shape of a purse-string suture ( Fig. 2. Fig. 2 c ). Next, the root of the tumor was encircled using a loop device, which was gradually tightened and lifted, while the nylon cord was tightened to pre-close the peripheral tissues of the lesion, before the mass was excised in its entirety ( Fig. 2. Fig. 2 d ). Ultimately, the gastric fundus mass was swiftly and entirely excised with no post-procedural bleeding or exposure of muscular tissue ( Fig. 2. Fig. 2 e, f ).
Fig. 1 A submucosal mass in the fundus of the stomach is seen on: a endoscopic view, where it presents as a submucosal bulge with a smooth surface; b endoscopic ultrasound, which shows that the lesion originates in the lamina propria, is hypoechoic, has an intact peritoneum, and measures approximately 6.3 × 4.8 mm.
Fig. 2 Endoscopic images of the treatment process showing: a after installation of the ligature at the end of the endoscope, the mirror being used to find the tumor, adjust the angle, and slowly draw the tumor into the ligature; b a pseudo-polypoid bulge that is formed after correctly aligning the head end of the ligature, applying negative pressure to draw the tumor completely into the transparent cap, and releasing the ligature ring; c three metal clips placed around the tumor after removal of the ligature ring, with a nylon rope forming a purse-string suture; d gradual tightening of the loop ligature ring and lifting around the root of the tumor, which is performed simultaneously with tightening of the nylon cord to pre-close the peripheral tissues of the lesion, before resection of the entire lesion; e the final appearance of the tightened purse-string suture after tumor resection. f The macroscopic appearance of the resected specimen.
This approach not only ensures the effectiveness and safety of the procedure, but also reduces both the duration of the procedure and the post-procedure hospitalization, rendering it innovative and worthy of clinical promotion.
Endoscopy_UCTN_Code_TTT_1AO_2AG_3AF
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Casali PG Blay JY Abecassis N Gastrointestinal stromal tumours: ESMO-EURACAN-GENTURIS Clinical Practice Guidelines for diagnosis, treatment and follow-up Ann Oncol 202233203310.1016/j.annonc.2021.09.00534560242 · doi ↗ · pubmed ↗
- 2Abdallah M Suryawanshi G Mc Donald N Endoscopic full-thickness resection for upper gastrointestinal tract lesions: a systematic review and meta-analysis Surg Endosc 2023373293330510.1007/s 00464-022-09801-x 36517704 · doi ↗ · pubmed ↗
- 3Zhou PH Yao LQ Qin XY Endoscopic full-thickness resection without laparoscopic assistance for gastric submucosal tumors originated from the muscularis propria Surg Endosc 2011252926293121424195 10.1007/s 00464-011-1644-y · doi ↗ · pubmed ↗