Endoscopic management of long-standing rectovaginal fistula caused by foreign bodies
Li Wang, Zu-Qiang Liu, Pei-Rong Xu, Lu Yao, Hao Hu, Quan-Lin Li, Ping-Hong Zhou

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
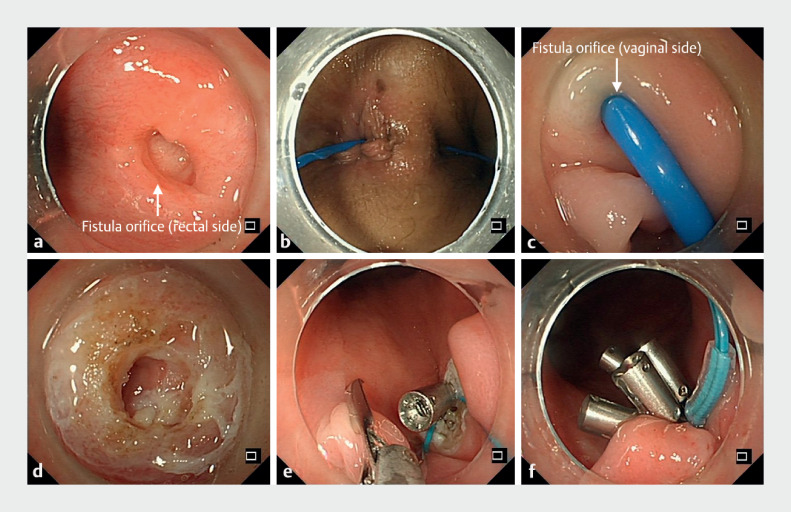 Fig. 1
Fig. 1- —Shanghai Rising Stars of Medical Talent Youth Development Program
- —Ministry of Science and Technology of the Peopleʼs Republic of China > National Natural Science Foundation of China
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAnorectal Disease Treatments and Outcomes · Diverticular Disease and Complications · Pelvic floor disorders treatments
A 32-year-old woman was admitted, presenting with a 30-year history of rectovaginal fistula (RVF). At the age of 1 year, the patient inadvertently ingested a paperclip, resulting in fecal discharge from the vagina, and no intervention was implemented.
Colonoscopy revealed a 0.8-cm fistula above the dentate line on the anterior rectal wall ( Fig. 1. Fig. 1 a ). Transanal endoscopic closure was proposed after a multidisciplinary evaluation ( Video 1Video 1 ).
Fig. 1 Endoscopic management of rectovaginal fistula. a Colonoscopy revealed a 0.8-cm fistula (arrowhead) above the dentate line on the anterior rectal wall. b, c A bougie inserted through the rectal fistula opening was exposed within the vagina. d The mucosal epithelium and scar tissue within the fistula orifice and sinus tract were destroyed with argon ion coagulation. e, f After confirming no bleeding, purse-string suturing was used to close the rectal fistula.
A long medical history of rectovaginal fistula caused by swallowing a foreign body was successfully treated with endoscopic purse-string suturing.Video 1Video 1
Upon bimanual examination, a cord-like structure extending from the anterior wall of the rectum to the posterior wall of the vagina was palpable. A bougie inserted through the rectal fistula opening was exposed within the vagina ( Fig. 1. Fig. 1 b, c ). Argon ion coagulation was used to destroy the mucosal epithelium and scar tissue within the fistula orifice and sinus tract ( Fig. 1. Fig. 1 d ). After confirming no bleeding, purse-string suturing was used to close the rectal fistula ( Fig. 1. Fig. 1 e, f ). The procedure duration was 30 minutes.
The patient recovered uneventfully and was discharged on postoperative day 2. The patient did not experience any discomfort during the 2-year postoperative follow-up.
The main causes of RVF are obstetric trauma, chronic inflammatory bowel disease, pelvic floor or rectal surgery, trauma, or radiation therapy, and swallowed foreign bodies are a rare cause 11 . Although various medical and surgical (including transanal, transvaginal, and transperineal) methods have been used to manage RVFs, the treatment remains a challenge due to its tendency to recur. Innovative transanal endoscopic surgery has been proposed for the treatment of RVF, but endoscopic purse-string suturing has not previously been reported for the treatment of RVF 22 . Here, we present the first report of a case of a long medical history of RVF caused by swallowing a foreign body, which was successfully treated with endoscopic purse-string suturing. This report provides an innovative, minimally invasive treatment approach for patients with RVF.
Endoscopy_UCTN_Code_TTT_1AQ_2AB
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Byrnes JN Schmitt JJ Faustich BM Outcomes of rectovaginal fistula repair Female Pelvic Med Reconstr Surg 20172312413010.1097/SPV.000000000000037328106653 · doi ↗ · pubmed ↗
- 2Yuan X Chen H Chen C Minimally invasive treatment of mid-low rectovaginal fistula: a transanal endoscopic surgery study Surg Endosc 2020343971397710.1007/s 00464-019-07174-231728753 · doi ↗ · pubmed ↗