Amelanotic melanoma with neural lesion simulating leprosy
Andrezza Telles Westin, Sebastião Antônio de Barros Junior, Cacilda da Silva Souza

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
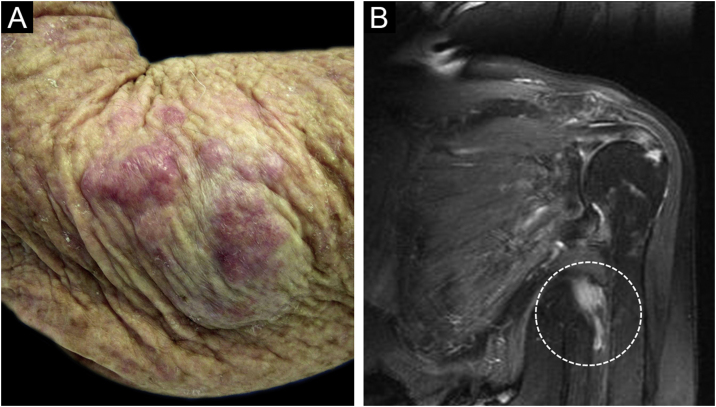 Figure 1
Figure 1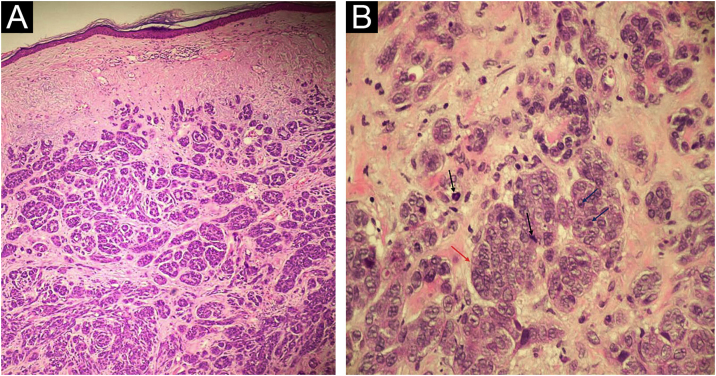 Figure 2
Figure 2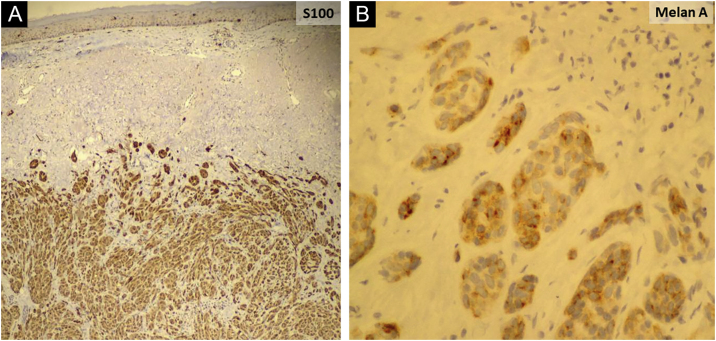 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCutaneous Melanoma Detection and Management · Animal testing and alternatives · Melanoma and MAPK Pathways
Dear Editor,
Amelanotic/hypomelanotic melanoma (AHM) is a subtype of cutaneous melanoma with little or no pigment on macroscopic inspection and dermoscopic evaluation, or absence of melanin on histopathology. It is a rare entity, with variable frequency, between 0.4% and 27.9%, but possibly underestimated.1
The absence of pigmentation and clinical criteria for suspected melanoma, and the morphological variability of AHM possibly lead to erroneous and late diagnosis.1, 2 AHM can mimic a variety of benign and malignant diseases of different etiologies, whether inflammatory or infectious, in addition to neoplasias.1, 2
An 81-year-old woman was referred with suspected leprosy due to loss of strength and dropping of her left hand two months before and asymptomatic lesions on her left elbow three years before. The examination showed a group of pink papules and nodules, slightly shiny, not adhered to deeper planes, with polymorphic vessels on dermoscopy, on the side of the elbow (Fig. 1A); a deficit in arm abduction and extension of the left elbow, wrist and fingers; and a palpable 5-cm mass in the left armpit. Magnetic resonance imaging showed an expansive lesion involving the left axillary vascular-nervous bundle (Fig. 1B); electroneuromyography showed severe damage to the radial nerve. Histopathological analysis showed lentiginous proliferation of atypical melanocytes, arranged in confluent nests in the epithelium and in pagetoid migration to the upper layers of the epidermis. The dermis was infiltrated by a neoplasm of pleomorphic cells with vesicular nuclei and basophilic cytoplasm with evident nucleoli, arranged in nests and blocks, compatible with nodular melanoma of the skin (Fig. 2), presenting satellite, and in-transit metastases in the left arm. Regional metastasis was confirmed by biopsy of the mass involving the left axillary neurovascular bundle, thus defining the initial staging in TxN3cM1. Immunohistochemistry was positive for S100, CEA, and Melan-A (Fig. 3), and negative for HMB-45 and tyrosinase. Treatment with interferon was started (3,000,000 IU, three times a week), axillary radiotherapy was refused by family members, and survival was ten months.Figure 1(A) Shiny pink nodules and papules in the left elbow area, representing and in-transit metastases; (B) Magnetic resonance imaging showing a nodular image next to the left axillary vascular-nervous bundle, suggestive of neoplasm.Figure 1. Figure 2(A) Neoplasm consisting of basophilic cells, forming well-developed nests and masses that infiltrate the dermis, without affecting the epidermis (Hematoxylin & eosin, ×40 and ×100); (B) Cells with eosinophilic cytoplasm and pleomorphic nuclei, vesicular chromatin (red arrow), evident nucleoli (blue arrows) and frequent atypical mitoses (black arrows); (Hematoxylin & eosin, ×40 and ×100).Figure 2. Figure 3Immunohistochemistry revealing positive staining for S100 (A) and Melan-A (B).Figure 3
Clinically, red, pink or erythematous lesions represent almost 70% of AHMs, but they may be normochromic.1 The papulonodular form predominated in 58% of cases.1 Among other clinical forms of AHM, there is the erythematous macule with epidermal changes on skin exposed to the sun, and the normochromic dermal plaque without epidermal changes.3 All histopathological subtypes can be found among AHMs: nodular, acral lentiginous and subungual, superficial spreading and lentigo maligna.1, 2, 3, 4
Despite the absence of melanin-containing structures, in some cases, it is possible to observe residual pigmentation and a vascular pattern on dermoscopy, not perceptible to the naked eye.1, 5 Different vascular morphologies have been recognized in AHMs: irregular linear, serpentine (polymorphic), dotted and staple-shaped vessels, as well as milky-red areas, and white structures and lines.5 However, the vascular pattern in association with the history and clinical findings, and particularly the histopathological and immunohistochemical analyses are necessary for diagnosis.1
Female gender, nodular and unclassified histopathological subtypes, increased Breslow thickness, presence of mitoses, severe solar elastosis, and absence of coexisting nevus have been associated with AHM.2 The presence of mitoses, regardless of Breslow thickness, suggests that AHMs may grow more quickly presenting more advanced tumor stages and shorter survival, when compared to pigmented melanoma.2 Notably, patients with AHMs were more likely to be misdiagnosed compared to those with pigmented melanomas.4 These aspects require a high index of suspicion to potentially minimize late diagnosis at advanced stages of the disease.
Financial support
None declared.
Authors’ contributions
Andrezza Telles Westin: Design and planning of the study; data collection, or analysis and interpretation of data; drafting and editing of the manuscript or critical review of intellectual content; collection, analysis and interpretation of data; intellectual participation in the propaedeutic and/or therapeutic conduct of the studied case; approval of the final version of the manuscript.
Sebastião Antônio de Barros Junior: Data collection, or analysis and interpretation of data; collection, analysis and interpretation of data; approval of the final version of the manuscript.
Cacilda da Silva Souza: Design and planning of the study; data collection, or analysis and interpretation of data; drafting and editing of the manuscript or critical review of intellectual content; collection, analysis and interpretation of data; intellectual participation in the propaedeutic and/or therapeutic conduct of the studied case; critical review of the literature; approval of the final version of the manuscript.
Conflicts of interest
None declared.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gong H.Z.Zheng H.Y.Li J.Amelanotic melanoma Melanoma Res 2920192212303067288110.1097/CMR.0000000000000571 · doi ↗ · pubmed ↗
- 2Thomas N.E.Kricker A.Waxweiler W.T.Dillon P.M.Busman K.J.From L.Genes, Environment, and Melanoma (GEM) Study Group. Comparison of clinicopathologic features and survival of histopathologically amelanotic and pigmented melanomas: a population-based study JAMA Dermatol 1502014130613142516229910.1001/jamadermatol.2014.1348 PMC 4262611 · doi ↗ · pubmed ↗
- 3Adler M.J.White C.R.Jr Amelanotic malignant melanoma Semin Cutan Med Surg 161997122130922055110.1016/s 1085-5629(97)80006-5 · doi ↗ · pubmed ↗
- 4Strazzulla L.C.Li X.Zhu K.Okhovat J.P.Lee S.J.Kim C.C.Clinicopathologic, misdiagnosis, and survival differences between clinically amelanotic melanomas and pigmented melanomas J Am Acad Dermatol 802019129212983065407510.1016/j.jaad.2019.01.012 · doi ↗ · pubmed ↗
- 5Dawood S.Altayeb A.Atwan A.Mills C.Dermoscopic features of amelanotic and hypomelanotic melanomas: a review of 49 cases Dermatol Pract Concept 122022 e 202206010.5826/dpc.1202 a 60PMC 911651235646464 · doi ↗ · pubmed ↗