Total hip arthroplasty with porous tantalum trabecular metal pads in patients with Crowe IV developmental dysplasia of the hip: a midterm followup study
Cheng Yang, Donghai Li, Shuo Sun, Zhouyuan Yang, Pengde Kang

TL;DR
This study shows that using porous tantalum metal pads in hip replacement surgery for severe hip deformity provides good mid-term results.
Contribution
The study presents mid-term clinical outcomes of using porous tantalum trabecular metal pads in THA for Crowe IV DDH patients.
Findings
87.5% of hips showed mild or no limping after surgery.
Survivorship of the TM construct was 90.6% at 5 years and 87.5% at 10 years.
Harris Hip Score improved significantly from preoperative to postoperative evaluations.
Abstract
Crowe IV developmental dysplasia of the hip (DDH) is a catastrophic hip disease. Moreover, obtaining ideal clinical efficacy in conventional total hip arthroplasty (THA) is often difficult. In this study, we aimed to assess the mid-term clinical results of THA with porous tantalum trabecular metal (TM) pads for acetabular reconstruction in the treatment of Crowe IV DDH. A cohort of 28 patients (32 hips) diagnosed with Crowe type IV DDH who underwent acetabular reconstruction during THA using TM pads with scheduled follow-up between 2011 and 2018, were included in this study. Eight cases were men and 24 were women, with a mean age of 48.4 years (range, 36–72 years) and a mean follow-up was 74.3 months (range, 42–132 months). All patients underwent acetabular reconstruction using TM pads and total hip replacement with subtrochanteric osteotomy. At the final follow-up, 28 hips (87.5%)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
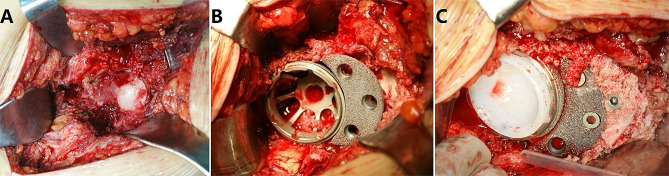 Figure 1
Figure 1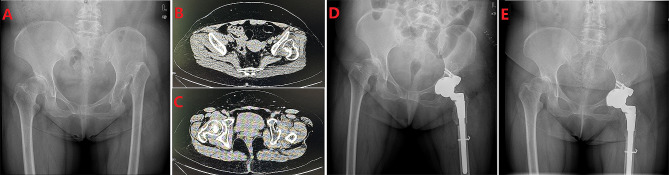 Figure 2
Figure 2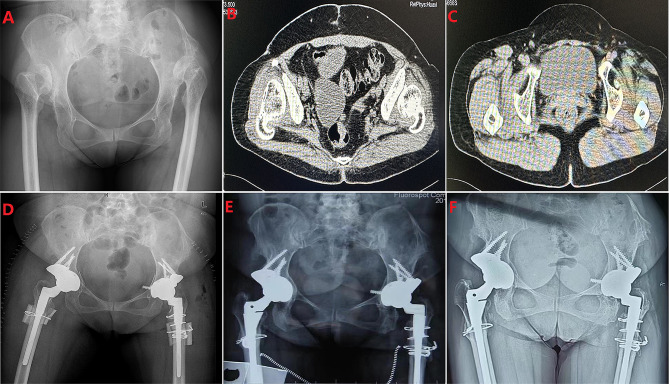 Figure 3
Figure 3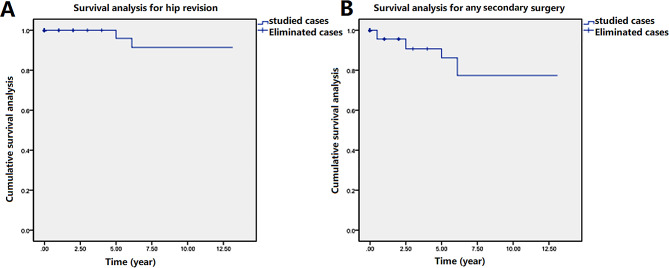 Figure 4
Figure 4- —Natural Science Fundation of Sichuan Province
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopaedic implants and arthroplasty · Hip disorders and treatments · Bone and Joint Diseases
Introduction
Type IV developmental dysplasia of the hip (DDH) is one of the most complex hip deformities that requires reconstruction [1]. DDH is the main cause of degenerative arthritis of the hip and valgus deformity of the knee and eventually necessitates total hip arthroplasty (THA) [2–4]. Moreover, THA is regarded as the optimal treatment choice for DDH and is associated with a high rate of functional improvement and pain relief [5–9]. THA has proven to be successful in the reconstruction of advanced DDH with functional impairments [10–12]. However, THA for Crowe IV DDH is technically challenging due to extensive distortions of the native anatomy. Patients with DDH may have a shallow acetabulum, a straight narrow femoral canal, and associated circumferential soft tissue deformities [13].
The distorted anatomy of the acetabulum and proximal femur poses a major challenge during THA [14–16]. Various methods and techniques have been proposed to restore the normal anatomical relations of the distorted hip joint in Crowe IV DDH. Additionally, previous studies have described several strategies to reconstruct the abnormal acetabulum using autogenous femoral head grafts, embedded bone grafts, and porous tantalum cups plus granular bone grafts during THA [16, 17]. However, the optimal treatment remains unclear. For more than a decade, we have used trabecular metal (TM) pads and augmentation techniques for acetabular reconstruction in hip revision or complex THA [18].
However, the application of TM pads in the treatment of Crowe type IV DDH has not been well reported. This study aimed to evaluate the clinical efficacy of mid-term THA combined with porous TM pads for acetabular reconstruction in patients with Crowe type IV DDH.
Materials and methods
After obtaining approval from the Institutional Review Board of West China Hpsital, we conducted a retrospective review of a consecutive series of adult patients with Crowe type IV DDH who underwent THA with porous TM pads and femoral shortening osteotomy at our institution. Written informed consent was obtained from all patients when they came back for follow-up. Patients were identified from a senior surgeon’s database between May 2011 and April 2018. The inclusion criteria encompassed preoperative radiographic evidence of Crowe type IV DDH, treatment with THA using a porous TM pad, femoral shortening osteotomy with a minimum follow-up of 3 years, and records of patient-reported outcomes (Harris Hip Score and Western Ontario and McMaster Universities Arthritis Index (WOMAC)) both preoperatively and postoperatively.
Surgical technique
Preoperative surgical planning and template measurements were performed. All surgeries were performed using a posterolateral approach, with the patient in the lateral decubitus position. The femoral head was resected after hip dislocation. Extended trochanteric osteotomy was then performed in the hips, if necessary. The false and true acetabulae were identified after removing the obscuring osteophytes. After confirming the rotational centre, the true acetabulum was meticulously debrided and reamed to expose the robust, vascularized bone. When the acetabular has poor bone mass and provides less than 70% bone coverage of the acetabular component, we choose the acetabular component more than 48 mm. Simultaneously, autologous and artificial bone substitutes were then applied to the acetabulum combined with uncemented porous tantalum acetabular pads (TM Acetabular Revision System; Zimmer) for acetabular reconstruction. The tantalum pad was then impacted into the acetabulum, and fixation was performed using two to four cancellous screws. An appropriately sized acetabular cup was precisely implanted (Fig. 1). Fluoroscopic assessment of position and stability was performed intraoperatively. The hips were subjected to subtrochanteric osteotomy, and the femur was prepared by broaching the proximal region of the femoral component. The transverse shortening osteotomy level was identified as 1 cm distal to the lesser trochanter, and a longitudinal mark was made on the femur as a reference to reestablish femoral rotation after osteotomy. Subsequently, a transverse osteotomy was performed, and the trial S-Rom prosthesis was inserted into the proximal femur to confirm the appropriate size of the selected femoral component. Following osteotomy, hip range of motion and stability were evaluated, and trial implants were adjusted accordingly. The cylindrical segment of the femur removed during shortening osteotomy was split into two or three segments and used as onlay grafts to reinforce the osteotomy site secured with a titanium wire. The patients were instructed to limit their weight-bearing activities and adhere to posterior hip precautions for 12 weeks after surgery.
Fig. 1. Intraoperative surgical picture of acetabular reconstruction. (A) The true acetabulum was meticulously debrided and reamed. (B) Autologous bone was applied to the acetabulum combined with uncemented porous tantalum acetabular pads for acetabular reconstruction. (C) The tantalum pad was impacted into the acetabulum, and fixation was performed using three cancellous screws
Outcome evaluation
All patients underwent postoperative follow-up at 1, 3, and 6 months and annually thereafter. At each visit, functional outcomes were assessed using the WOMAC [19], Harris Score [20], and SF-12 score [21]. Radiographic evaluation was performed at each visit using standard anteroposterior radiographs of the pelvis and full-length radiographs of the lower extremities. Osteolysis of the acetabulum and femur was performed as described previously [22, 23]. The criteria described by Engh et al. were used to assess femoral implant loosening [24].
Statistical analysis
SPSS 26.0 (IBM Corp., Armonk, NY, USA) was used for all statistical analyses. Demographic data are presented as mean and range values, and percentages are used to describe categorical variables. Data were analyzed using Student’s t-test and are presented as the mean ± standard error of the mean. Kaplan-Meier survival analysis with 95% confidence interval (CI) was used to evaluate overall survival of the acetabular reconstruction and THA with failure defined as revision for any cases. Statistical significance was set at P < 0.05.
Results
A total of 32 hips in 28 patients who underwent surgery between May 2011 (when our use of tantalum pads began) and April 2018, were included in the final analysis. Basic characteristics of the patients, preoperative and postoperative radiographs, and porous TM pad information were collected and reviewed. The average operation time was 176.5 min and the mean blood loss was 224 mL. The mean hospital stay was 7.5 days (Table 1).
Table 1. Basic characteristics of the included patientsParametersOutcomesInclunded cases (n, hips)n = 32Age (years)48.4 ± 10.5Gender (male/female)8/24Side (right/left)17/15BMI (kg/m^2^)23.2 ± 4.3Preoperative Harris hip score58.4 ± 10.6Leg length discrepancy, cm4.6 ± 1.1Mean pads diameter, mm55.8 ± 5.4Hospital stay (day)7.5 ± 2.8Operative time (min)176.5 ± 31.6Intraoperative blood loss (mL)224.6 ± 89.6Acetabular components (Median, mm)52 (48 to 56)Follow up (months)74.3 ± 16.8
At a mean follow-up of 74.3 months (42 to 132 months), the pelvic radiographs displayed that the mean hip centre position was 2.92 ± 0.51 cm horizontally and 2.12 ± 0.48 cm vertically, and the mean acetabular inclination was 37.8 ± 7.2° (Table 2). Two patients who underwent single hip reconstruction (6.25%) had severe limping, two (6.25%) had moderate limping, and 13 (40.6%) had mild postoperative limping (Figs. 2 and 3). The Harris Hip Score improved from 58.4 ± 10.6 preoperatively to 85.6 ± 8.9 at the last follow-up (P < 0.01). The Mean WOMAC scores were 86.5 ± 10.2 for pain, 87.3 ± 12 for stiffness, and 85.4 ± 11.6 for function with a score of 90.4 ± 7.6 for patient satisfaction. The mean scores of patient satisfaction were 90.4 ± 7.6, indicating a good level of satisfaction regarding pain relief, function, and recreational activities (Table 2). SF-12 physical summary score was 41.8 ± 5.6 and SF-12 mental summary score was 51.6 ± 5.4 (Table 2).
Table 2. Clinical and radiological resultsVariableOutcomesHip centre horizontally (cm)2.92 ± 0.51Hip centre vertically (cm)2.12 ± 0.48Acetabular inclination (°)37.8 ± 7.2Leg length discrepancy (cm)1.14 ± 1.04Postoperative Limping Levels Severe, n (%) Moderate, n (%) Mild, n (%) None, n (%)2(6.25%)2(6.25%)13(40.63%)15(46.88%)Harris hip score85.6 ± 8.9WOMAC* scores Pain Stiffness Function86.5 ± 10.287.3 ± 12.485.4 ± 11.6SF-12* physical summary scoreSF-12* mental summary score41.8 ± 5.651.6 ± 5.4Patient satisfaction score90.4 ± 7.6*WOMAC and SF-12 scores are normalized to a range of 0 to 100 points, with 0 being worst and 100 being best. Satisfaction score: 0 is worst, 100 is best
Fig. 2. Pre- and postoperative radiographs of a woman with left Crowe type IV DDH. (A) Preoperative pelvic radiograph of a 60-year-old female patient with left Crowe type IV developmental dysplasia of the hip (DDH). (B) CT image shows the position of the left false acetabulum. (C) CT image shows bilateral true acetabulum position. (D) Postoperative pelvis radiograph demonstrating left acetabular reconstruction using a TM pads, and femoral shortening osteotomy on each side. (E) six years post-surgery, the pelvic X-ray revealed no evidence of loosening or absorption on the acetabular side and complete osseous integration on the femoral side without any subsidence
Fig. 3. Pre- and postoperative radiographs of a woman with Crowe type IV DDH. (A) Preoperative pelvis radiograph of a 44-year-old woman with bilateral Crowe type IV DDH. (B) CT image shows the position of the bilateral false acetabulum. (C) CT image shows the bilateral true acetabulum position. (B) Postoperative pelvis radiograph demonstrating bilateral acetabular reconstruction using a tanium mesh cup, cemented liner, and femoral shortening osteotomy on each side. (C) Three years post-surgery, the pelvic X-ray revealed no evidence of either hip socket loosening or absorption.(D)After a post-surgical period of 11 years, the pelvic X-ray revealed no evidence of loosening or absorption on the acetabular side and complete osseous integration on the femoral side without any subsidence
No intraoperative complications occurred during the acetabular placement in any patient. However, intraoperative femoral fracture occurred in two patients who underwent transverse subtrochanteric osteotomy. Six cases of postoperative intramuscular thrombosis were observed, and two patients experienced sciatic nerve palsy after surgery. However, both cases resolved with no residual deficits at the 6-month follow-up visit. Additionally, one case of subtrochanteric osteotomy bone nonunion and another of postoperative prosthesis dislocation, both of which underwent secondary surgery. Two patients developed painful aseptic loosening of the acetabular component and TM pads. The previous large-diameter cup was replaced with pads of appropriate dimensions and contours, resulting in two patients undergoing allogeneic granular bone grafts in conjunction with the replacement procedure. Postoperative follow-up revealed favourable outcomes. No pulmonary emboli, deep venous thromboses, or cardiac or cerebrovascular complications were observed during the follow-up period (Table 3).
Table 3. Complications occorrenceComplicationships, nPulmonary embolismNoneDeep vein thrombosisNonePeriprosthesis infectionNoneCardio-cerebrovascular complicationsNoneComponent looseningNoneIntraoperative fracture2Dislocation1Nonunion1Leg length discrepancy1Nerve palsy2Intermuscular vein thrombosis6stem aseptic loosening1Cup and pads migration1Hip revision2
TM construct Kaplan-Meier survivorship at a mean follow-up of 6.2 years, the TM construct survivorship due to all-cause failure was 90.6% at 5 years with 3 hips at risk, 87.5% at 10 years with 4 hips at risk. The survivorship due to failure from aseptic loosening was 96.9% at 5 years with 1hips at risk and 93.75% at 10 years with 2 hips at risk. (Figs. 4)
Fig. 4. Survival analysis based on the cases of hip revision (A) and any secondary surgery (B)
Discussion
The technique of using porous tantalum TM pads for acetabular reconstruction during complex revision THA has been providing increasing evidence of excellent early to long-term outcomes as reported in the published series [25–29]. We have been utilising this technology for several years to manage Crowe type IV DDH with acetabular insufficiency.
THA for Crowe type IV DDH is widely acknowledged to have a higher incidence of complications and failure rates than routine THA for primary osteoarthritis [10]. The preoperative assessment of the acetabular and proximal femoral anatomy, in conjunction with surgical techniques and expertise, are pivotal factors for achieving successful outcomes (Table 4). The current retrospective study presents the mid-term outcomes of a series of patients. with Crowe type IV DDH who underwent THA using a tantalum pad and subtrochanteric femoral shortening osteotomy.
Table 4. Review the literature on treatment techniques of crowe type IV DDHAuthorCases(n, hips)Follow-upAcetabulum TechniquesFemur techniqueSuccess rate (%)Harris scoresOrs C [2]1278.4 yearsTrilogy IT acetabular ComponentWagner cone stem + TSO94.5%94.2 ± 6.9Caylak R [3]67> 10 yearsCementlessacetabular componentCeramic-on-ceramic bearing + TSO94%94.1 ± 8.1Ma HY [6]11671.3 monthsPinnacle acetabular cupCeramic-on-ceramic bearing + modular S-ROM stem + TSO98.3%91.3 ± 4.2Krych AJ [9]274.8 yearsPorous-coated acetabular componentExtensively porous-coatedstems/S-ROM + TSO77.8%89Farrell CM [30]288–15 yearsUncemented/cemented acetabular component + FHSANot reported82.1%not reportedZhao HY [31]502 yearsPorous-coat acetabular componentsTSO98%96.5 ± 9.6Pei L [32]1242.2 monthsAllofit biologic acetabulum components + FHSAML wedge femoral stem91.7%89.7 ± 3.9TSO: transverse subtrochanteric osteotomy; FHSA: ipsilateral femoral head structural autograf
Reconstruction of acetabulum in Crowe type IV DDH is always the challenges for surgeons, for example, the acetabulum was undeveloped or poorly developed, acetabular bone mass is limited, acetabular component placed in the true acetabulum position has poor coverage of the acetabular roof and severe bone defect. Reconstructing the acetabulum to its true anatomical position has previously been demonstrated to enhance hip biomechanics in cases of DDH [33, 34]. Many different strategies have been used to reconstruct the acetabulum. These include autogenous femoral head transplantation, impacted bone grafting, and the use of metal cups with particle bone grafting [17]. Our previous study used porous-coat acetabular components and transverse subtrochanteric osteotomy to manage patients with Crowe type IV DDH. The clinical outcomes of our initial study were encouraging, although acetabular reconstruction was difficult in several patients [31]. In the current study, stable acetabular component fixation was obtained using tantalum metal blocks to reconstruct dysplastic acetabular defects exceeding 30%. In our mid-term study, no obvious signs of implant migration or subsidence were observed.
Porous tantalum, also known as trabecular metal, is a popular choice for managing bone loss in acetabular reconstruction due to its exceptional mechanical properties. Firstly, tantalum exhibits a higher porosity, approximately two to three times that of cobalt, chromium, and titanium, thereby promoting significant bone and fibrous ingrowth potential [35, 36]. Secondly, the elastic modulus of porous tantalum (also known as trabecular metal) closely resembles that of trabecular bone. Consequently, porous tantalum facilitates the physiological transfer of load from the implant to the host bone, minimizes stress-shielding effects, and preserves the bone stock [37]. Thirdly, biomechanical testing demonstrated that porous tantalum possesses a high coefficient of friction, which imparts superior implant stability compared to that of traditional cementless implants [38]. The attainment of intraoperative stability of the acetabular components is crucial for achieving successful mid-term outcomes [39]. Hence, porous tantalum metal has been used for acetabular bone defect reconstruction in hip revision for some time. However, the application of porous tantalum TM pads for acetabular reconstruction in patients with Crowe type IV DDH has not yet been widely reported.
The available reconstructive techniques for DDH are extensive, and this series cannot compare our results with those of alternative approaches. Other techniques for reconstructing DDH involve the utilisation of acetabular reinforcement devices in conjunction with structural bone grafting, autogenous femoral head grafting, and alternative metal cups combined with allogenic structural bone grafting. However, graft healing and stability are crucial technical factors. The assimilation of an autogenous femoral head bone graft into the pelvis occurs slowly and incompletely, rendering it susceptible to collapse and resorption [30]. The other reconstruction methods, such as incarcerated and granular bone grafting, fail to provide sufficient initial stability for the acetabulum alone for rapid absorption, thereby compromising long-term stability [32]. The stability of other bone grafts fixed with metal mesh and cups attached with bone cement can be deemed sufficient; however, their long-term survival rate is unsatisfactory, and the incidence of aseptic loosening is high [40]. In the current study, we used porous TM pads for acetabular reconstruction and achieved promising mid-term follow-up clinical results with a 6.2-year success rate of 93.75% and a mean Harris score of 85.6. The results of our study were comparable to the results obtained from previous studies (Table 4).
Our study had several limitations. The sample size was relatively small, which limited the ability of our dataset to draw definitive conclusions regarding patient outcomes. The technique described in this study was initially used at our institution a decade ago. The initial number of treated patients was lower than the current practice volume. The small number of patients treated in the past limited the number of patients who met the length of follow-up required for inclusion in this study. Future studies should incorporate a large sample size of patients with adequate follow-up duration. The patients included in our study were relatively young, with a mean age of 48.4 years (range 34–85) at the time of the revision surgery. Consequently, acknowledging that our findings are limited to this specific age group and may not be readily extrapolated to older populations is important. Additionally, we did not investigate the relationship between the spine and pelvis, which is another limitation. Despite the follow-up period spanning from 4 to 10 years (with an average duration of 6.2 years), a significant portion of the data was presented during the mid-term assessment, highlighting the need for future investigations to explore long-term outcomes.
Conclusion
This study demonstrates that the implementation of porous TM pads for acetabular reconstruction in THA for Crowe type IV DDH yields favourable outcomes at mid-term follow-up, thereby potentially serving as a viable therapeutic option for patients affected by this severe deformity.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gharanizadeh K Mahmoudi M Shiva F Ghazavi M Abolghasemian M Assessing Leg length discrepancy is necessary before arthroplasty in patients with Unilateral Crowe type IV hip dislocation Clin Orthop Relat Res 202348191783910.1097/CORR.000000000000261136912864 PMC 10427045 · doi ↗ · pubmed ↗
- 2Ors C Caylak R Togrul E Total hip arthroplasty with the Wagner cone femoral stem in patients with Crowe IV Developmental Dysplasia of the hip: a retrospective study J Arthroplasty 2022371103910.1016/j.arth.2021.09.00734547428 · doi ↗ · pubmed ↗
- 3Caylak R Ors C Togrul E Minimum 10-Year results of Cementless Ceramic-On-Ceramic total hip arthroplasty performed with transverse Subtrochanteric Osteotomy in Crowe Type IV hips J Arthroplasty 2021361035192610.1016/j.arth.2021.05.03534127347 · doi ↗ · pubmed ↗
- 4Harris WH Traumatic arthritis of the hip after dislocation and acetabular fractures: treatment by mold arthroplasty. An end-result study using a new method of result evaluation J Bone Joint Surg Am 196951737 e 5510.2106/00004623-196951040-000125783851 · doi ↗ · pubmed ↗
- 5Du YQ Zhang B Sun JY Ma HY Shen JM Ni M Zhou YG The variation of the Pelvis in Unilateral Crowe Type IV Developmental Dysplasia of the hip Orthop Surg 20211325465210.1111/os.1290333619848 PMC 7957413 · doi ↗ · pubmed ↗
- 6Ma HY Lu Q Sun JY Du YQ Shen JM Gao ZS Lu SB Zhou YG One-stage total hip arthroplasty with modular S-ROM stem for patients with bilateral Crowe type IV Developmental Dysplasia Orthop Surg 202012619132210.1111/os.1284333185022 PMC 7767788 · doi ↗ · pubmed ↗
- 7Tao K Wang SC Ma XY Shao L Di ZL Huang ZY Three-dimensional femur morphology analysis for the optimal location of subtrochanteric osteotomy with an implanted Wagner cone stem in total hip arthroplasty for Crowe type IV developmental dysplasia of the hip J Orthop Surg Res 202318141010.1186/s 13018-023-03901-737277880 PMC 10243028 · doi ↗ · pubmed ↗
- 8Miyazaki T Shimizu T Ohura H Katayama N Iwasaki N Takahashi D Total hip arthroplasty with femoral shortening osteotomy using polished cemented stem vs. modular cementless stem in patients with Crowe type IV developmental dysplasia of the hip Arch Orthop Trauma Surg 2023143634879310.1007/s 00402-022-04518-x 35915263 · doi ↗ · pubmed ↗