Penetrating hypopharyngeal foreign body impalement of the thyroid gland: A case report of rare complication of ingested fish bone
Marwa AlTarayra, Khalil N.M. Abuzaina, Ahmed M.I. Aljodi, Sulaiman Fakhouri, Ammar W.M. Hassouneh

TL;DR
A 60-year-old woman had a rare complication where a fish bone pierced her thyroid gland after being swallowed, requiring surgery to remove it and highlighting the need for early detection.
Contribution
First reported case of a fish bone penetrating the thyroid gland after hypopharyngeal perforation.
Findings
A fish bone was found lodged in the left thyroid lobe after hypopharyngeal wall perforation.
Surgical removal via left hemithyroidectomy was necessary for successful treatment.
Early recognition and advanced imaging are critical to avoid severe complications like abscess or mediastinitis.
Abstract
Foreign body ingestion complicated by hypopharyngeal perforation is an uncommon but potentially life-threatening condition. Early recognition and appropriate management are crucial to prevent serious complications. We present an extremely rare case highlighting the importance of this clinical entity. A 60-year-old female presented with odynophagia 10 days after ingesting fish and chicken. Imaging revealed a linear foreign body penetrating through the left lateral hypopharyngeal wall into the left thyroid lobe, with surrounding inflammatory changes. The patient underwent neck exploration, which identified a sharp fishbone lodged in the postero-medial aspect of the left thyroid lobe, necessitating a left hemithyroidectomy for removal. To our knowledge, this is the first reported case of hypopharyngeal perforation by an ingested foreign body penetrating the thyroid gland itself. Despite…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
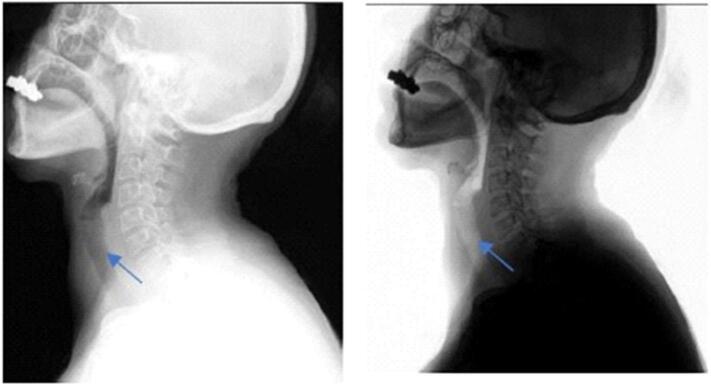 Figure 1
Figure 1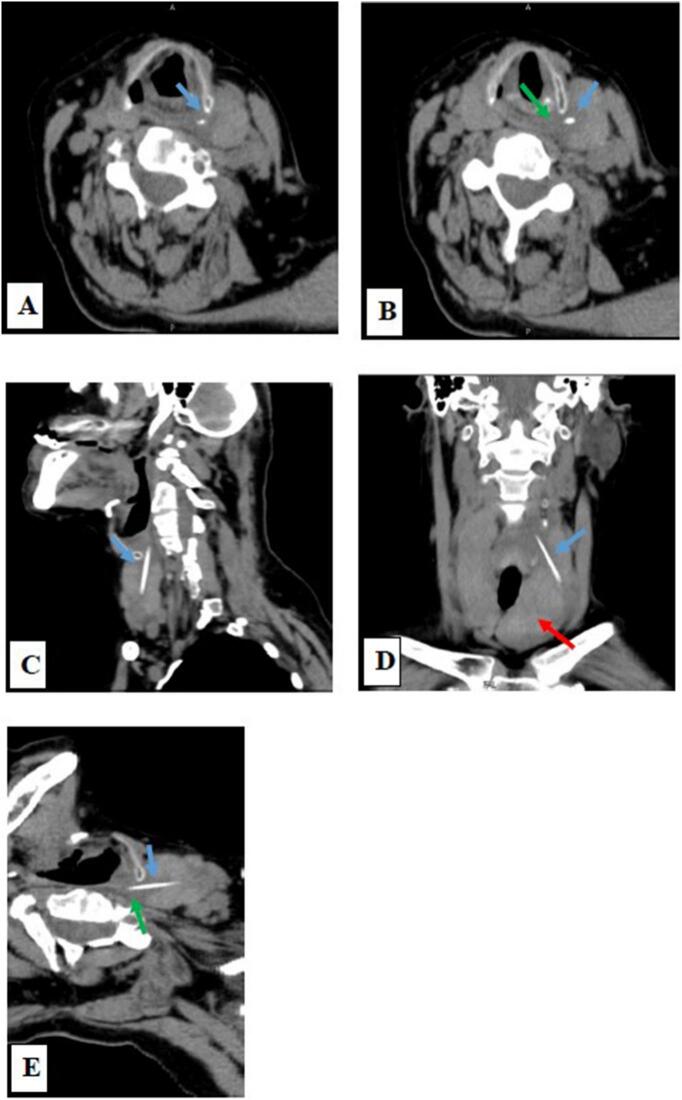 Figure 2
Figure 2 Figure 3
Figure 3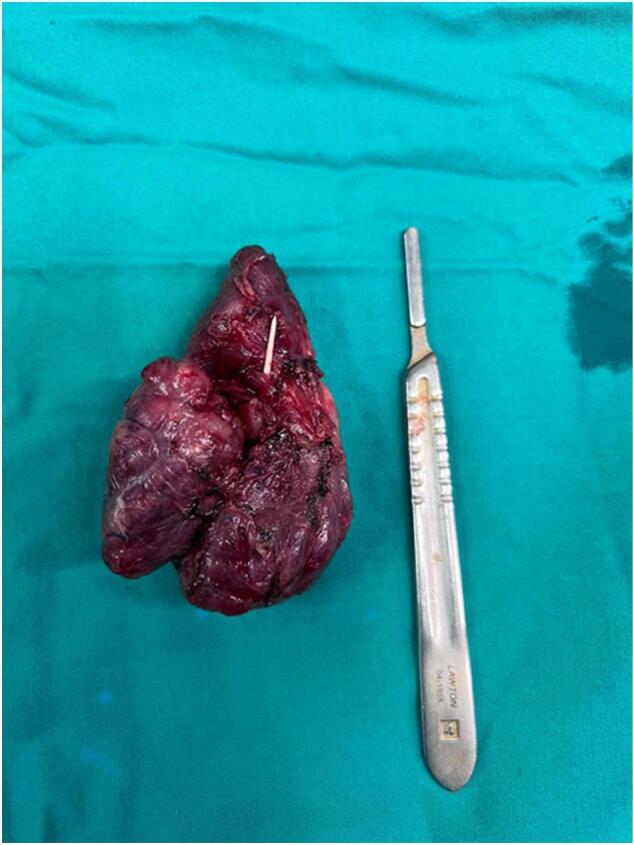 Figure 4
Figure 4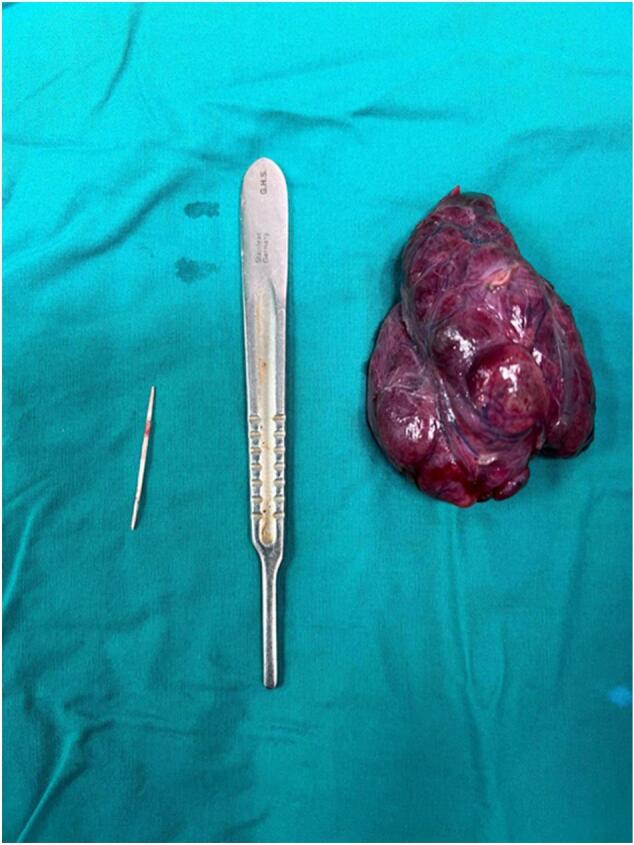 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsForeign Body Medical Cases · Restraint-Related Deaths · Airway Management and Intubation Techniques
Introduction
1
Foreign body ingestion is a common complaint frequently seen in the emergency department. Which, sharp objects may get lodged in the aerodigestive tract and subsequently cause a perforation. Although perforation of the hypopharynx is rare, early recognition and treatment is crucial to decrease the associated morbidity [1,2].
This case report presents an extremely rare case of hypopharyngeal perforation piercing the left thyroid lobe in a 60-year-old female 10 days after fish bone ingestion. A neck CT scan showed a foreign body penetrating the hypopharyngeal wall throughout the left thyroid lobe. She underwent neck exploration to remove the sharp object and subsequently a left hemithyroidectomy was performed.
Case presentation
2
A 60-year-old female presented to the ER complaining of odynophagia. These symptoms developed 10 days after ingestion of fish and chicken. There were no other related complaints (i.e., hematemesis, drooling, vomiting, choking, cyanosis, cough, dyspnea, or hemoptysis). The patient's medical and surgical histories were only significant for bronchial asthma.
On physical examination, she was hemodynamically stable and unremarkable except for mild tenderness over the left anterior neck above the level of the thyroid cartilage. A complete blood count and C-reactive protein level were obtained. The complete blood showed hemoglobin of 12.2 g/dL and a white blood cell count of 10.6 × 109/L. C-reactive protein was elevated at 9.4 mg/L.
The lateral neck radiograph showed a linear radiopacity in the region of the oropharynx suggestive of a foreign body; Normal thickness of retropharyngeal and retrotracheal space as shown in Fig. 1.Fig. 1. Lateral neck radiograph showed a linear radiopacity in the region of cricopharynx suggestive of a foreign body; Normal thickness of retropharyngeal and retrotracheal space.Fig. 1. Fig. 2Multiplanar CT images for the neck without IV contrast in the axial section (A and B) revealed a radiodense foreign body shown in Fig. 2. (blue arrow) lodged in the left lobe of the thyroid gland, its upper end abutting the left lateral wall of the hypopharynx at C5 vertebral body level which showed surrounding hypodensity representing the inflammatory reaction of surrounding soft tissue (green arrow) and lower end in the left lobe of the thyroid, no abscess collection or emphysema was noted.C and D: Sagittal and coronal section showed the linear radiodense foreign body (blow arrow) lodged in the left thyroid lobe; the Thyroid gland is enlarged and shows features of multinodular goiter (red arrow).E: The reformatted axial image showed the full length of the foreign body (blue arrow) with surrounding hypodensity along its course representing the inflammatory reaction of surrounding soft tissue (green arrow). (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)Fig. 2
She underwent neck exploration through a neck collar incision to remove the sharp object. Upon exposing the field; no foreign objects were noted and therefore ligation of the left thyroid lobe vessels was performed to expose the sharp object posteriorly. As expected, it was lodged in the posteromedial aspect of the left thyroid lobe (as shown in Fig. 3), and subsequently, a left hemithyroidectomy was performed as the offending object was located posteriorly behind the upper pole of the left thyroid lobe near the left superior thyroid artery. Careful dissection around pertinent anatomic structures facilitated the identification and removal of the fishbone without complications (Fig. 4, Fig. 5). There were no esophageal, tracheal, or vascular injuries. The patient had an uneventful postoperative course in terms of hypocalcemia, hoarseness, or even wound hematoma. She was discharged home 2 days after the operation. One week later, she followed up in the outpatient clinic with no complaints or further complications.Fig. 3A sharp object is lodged in the postero-medial aspect of the left thyroid lobe after ligation of the left thyroid lobe vessels.Fig. 3. Fig. 4A sharp object penetrating the left thyroid lobe in the posteromedial aspect is shown after left thyroidectomy was performed.Fig. 4. Fig. 5Shows the size of the sharp object.Fig. 5
Discussions
3
Hypopharyngeal perforation is uncommon and early recognition is important to avoid its serious complications. The most common causes are extraluminal including penetrating and blunt trauma, or endoluminal from an iatrogenic cause such as diagnostic or therapeutic endoscopy and endotracheal intubation. Foreign body ingestion resulting in hypopharyngeal perforation however is a rare cause [[3], [4], [5]].
The majority of cases of hypopharyngeal perforation due to foreign body ingestion have reported a fishbone as the causative object [4], which is among the most common foreign bodies reported in the upper aerodigestive tract [6].
Signs and symptoms of hypopharyngeal perforation include mostly odynophagia, subcutaneous emphysema, chest or neck pain, hoarseness, stridor, or hemoptysis [7]. Patients may also present with sore throat, dysphagia, and fever as late symptoms of the injury. Fever is often accompanied by retropharyngeal abscess, and subsequently carotid artery pseudoaneurysm formation if left untreated. Serious complications include mediastinitis, pleural empyema, septic shock, and death [8].
The diagnostic approach is unclear for hypopharyngeal perforation in the literature. Clinical assessment along with endoscopy are sometimes enough to make a definitive diagnosis in some cases [9]. Plain radiographs, CT, and contrast swallow scans can be used in combination if there is clinical suspicion of the diagnosis [10]. Neck and chest X-rays are essential initially for the evaluation of foreign bodies or emphysema [11,12]. A CT scan can detect small air collection and is often used to plan an appropriate surgical approach [11,13]. Moreover, Endoscopy helps to detect the presence, site, and extent of the perforation as well as inspects the involved area for pharyngeal edema or hematoma.
The management plan depends on many aspects, including the size and location of the perforation, the patient's hemodynamic status, and the presence or absence of complications [14]. The literature recommends conservative management in patients who are hemodynamically stable with a perforation less than 2 cm in size [14]. Conservative management includes intravenous broad-spectrum antibiotics, parenteral nutrition, and NGT feeding [14] and patients should be followed up to rule out serious complications. Surgical management is performed when there's systemic toxicity, perforations greater than 2 cm, extension to the esophagus, and penetrating injuries [14]. Our patient was managed surgically as she had a foreign body penetrating through the left thyroid lobe perforation.
Conclusion
4
This extremely rare case of hypopharyngeal perforation by an ingested fish bone penetrating the thyroid gland itself underscores the importance of maintaining a high index of clinical suspicion and pursuing timely diagnostic imaging in patients presenting with odynophagia or cervical symptoms following foreign body ingestion. Prompt surgical intervention was critical to prevent potentially life-threatening complications like abscess, mediastinitis or vascular injury. Increased clinician awareness regarding this unusual manifestation is essential, and documentation of such rare cases may guide future management strategies to optimize patient outcomes.
Methods
5
This work has been reported in line with the SCARE criteria [15].
Consent
Written informed consent was obtained from the patient for publication and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethical approval
Ethical approval was not applicable for this study, as there is no formal institutional ethical review board or committee overseeing research activities in the region where the work was conducted.
Funding
Self-funding, asking for a waive.
Author contribution
Khalil Abuzaina (1): study concept or design, editor, reviewer, corresponding author.
Sulaiman Fakhouri (2): study concept or design.
Guarantor
Khalil Abuzaina.
Conflict of interest statement
There is no conflict of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Noon E.Stapleton E.Hypopharyngeal perforation caused by blunt trauma during consensual fellatio: an expectant management approach BMJ Case Rep.148Aug 10 2021 e 24284610.1136/bcr-2021-242846(PMID: 34376415; PMCID: PMC 8356189)PMC 835618934376415 · doi ↗ · pubmed ↗
- 2Alsalamah R.K.Alaraifi A.K.Alsalem A.A.Waheed K.Hypopharyngeal perforation following foreign body ingestion: a case report Cureus 1311 Nov 18 2021 e 1970810.7759/cureus.19708(PMID: 34934574; PMCID: PMC 8684363)PMC 868436334934574 · doi ↗ · pubmed ↗
- 3Canji K.MitrovićS.M.JovancevićL.Complicated hypopharyngeal perforation caused by a foreign body Med. Pregl.607–8Jul-Aug 200739139610.2298/mpns 0708391 c(English, Serbian. PMID: 17990808)17990808 · doi ↗ · pubmed ↗
- 4Hinojar A.G.Díaz Díaz M.A.Pun Y.W.Hinojar A.A.Management of hypopharyngeal and cervical oesophageal perforations Auris Nasus Larynx 302May 200317518210.1016/s 0385-8146 (03)00042-7(PMID: 12753990)1275399010.1016/s 0385-8146(03)00042-7 · doi ↗ · pubmed ↗
- 5van Looij M.A.Feenstra L.Twee patiënten met een perforatie van de slokdarm respectievelijk hypofarynx door een botje in het eten [Two patients with a perforation of the esophagus and hypopharynx, respectively, caused by a bone in their food]Ned. Tijdschr. Geneeskd.14715 Apr 12 2003714717(Dutch. PMID: 12722535)12722535 · pubmed ↗
- 6Shishido T.Suzuki J.Ikeda R.Kobayashi Y.Katori Y.Characteristics of fish-bone foreign bodies in the upper aero-digestive tract: the importance of identifying the species of fish P Lo S One 168Aug 17 2021 e 025594710.1371/journal.pone.0255947(PMID: 34403441; PMCID: PMC 8370622)PMC 837062234403441 · doi ↗ · pubmed ↗
- 7Goudy S.L.Miller F.B.Bumpous J.M.Neck crepitance: evaluation and management of suspected upper aerodigestive tract injury Laryngoscope 1125 May 200279179510.1097/00005537-200205000-00005(PMID: 12150608)12150608 · doi ↗ · pubmed ↗
- 8Woodcock S.A.Bird H.Siriwardena A.K.Ellenbogen S.Hypopharyngeal perforation: an uncommon cause of pneumoperitoneum Emerg. Med. J.185Sep 200139639810.1136/emj.18.5.396(PMID: 11559620; PMCID: PMC 1725666)11559620 PMC 1725666 · doi ↗ · pubmed ↗