Lowest instrumented vertebrae in early onset scoliosis: is there a role for a more selective approach?
Michael J. Heffernan, Claudia Leonardi, Lindsay M. Andras, Bailli Fontenot, Luke Drake, Joshua M. Pahys, John T. Smith, Peter F. Sturm, George H. Thompson, Michael P. Glotzbecker, Tyler A. Tetreault, Benjamin D. Roye, Ying Li

TL;DR
This study examines how surgeons choose the lowest instrumented vertebra in children with early onset scoliosis and finds that most have a lower LIV than expected.
Contribution
The study identifies patterns in LIV selection and shows a lack of selective thoracic fusion potential in most EOS patients.
Findings
Most patients had an LIV at L3 or below, with smaller spinal height and larger curves linked to more caudal LIVs.
The LIV was often below the TV in patients with a TV at L2 or above, suggesting limited selective fusion potential.
Implant type and MCGR actuator length did not influence LIV selection.
Abstract
This purpose of this study was to assess the impact of patient and implant characteristics on LIV selection in ambulatory children with EOS and to assess the relationship between the touched vertebrae (TV), the last substantially touched vertebrae (LSTV), the stable vertebrae (SV), the sagittal stable vertebrae (SSV), and the LIV. A multicenter pediatric spine database was queried for patients ages 2–10 years treated by growth friendly instrumentation with at least 2-year follow up. The relationship between the LIV and preoperative spinal height, curve magnitude, and implant type were assessed. The relationships between the TV, LSTV, SV, SSV, and the LIV were also evaluated. Overall, 281 patients met inclusion criteria. The LIV was at L3 or below in most patients with a lumbar LIV: L1 (9.2%), L2 (20.2%), L3 (40.9%), L4 (29.5%). Smaller T1 − T12 length was associated with more caudal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1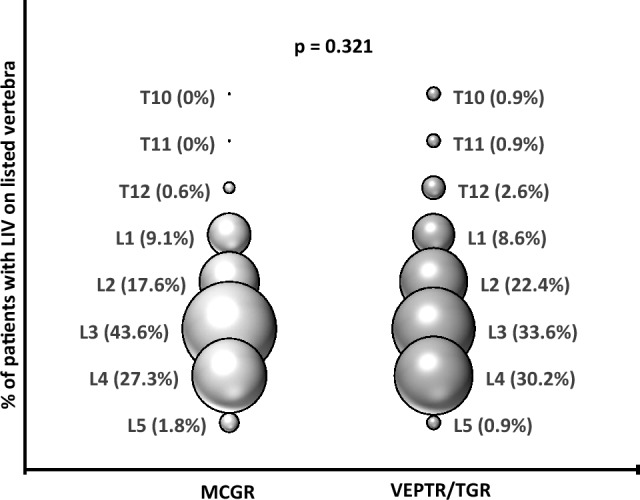 Figure 2
Figure 2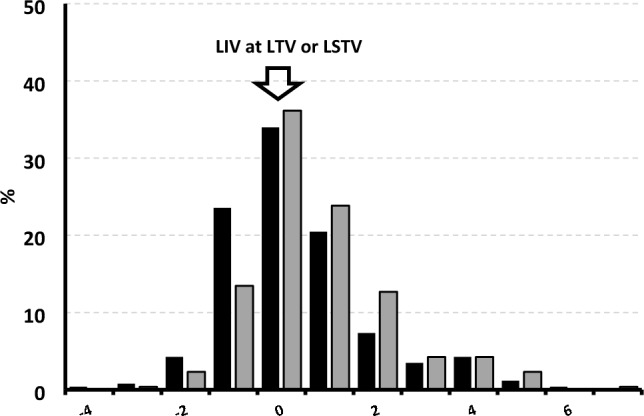 Figure 3
Figure 3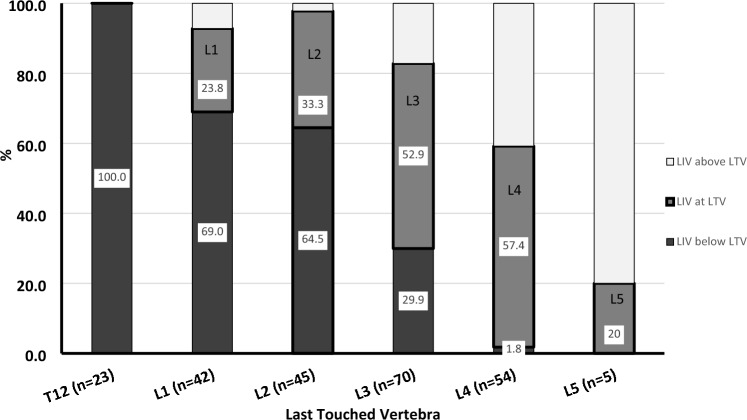 Figure 4
Figure 4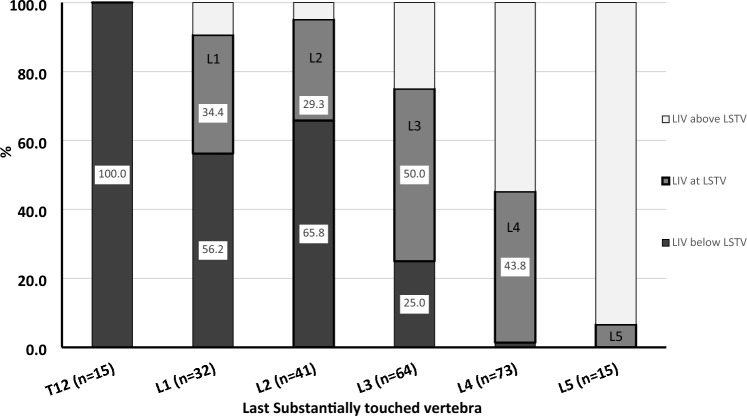 Figure 5
Figure 5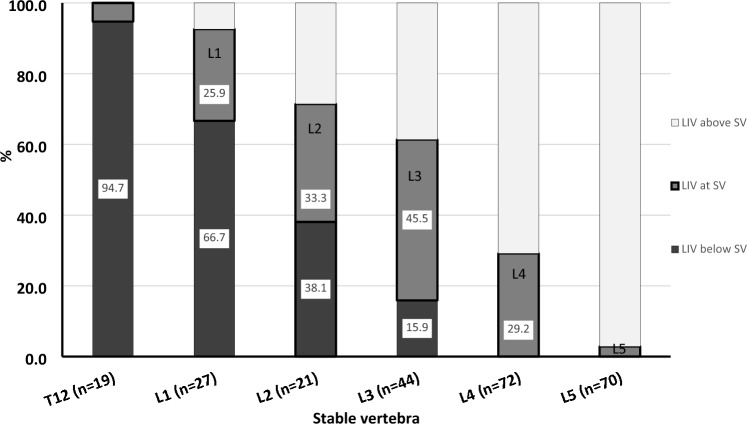 Figure 6
Figure 6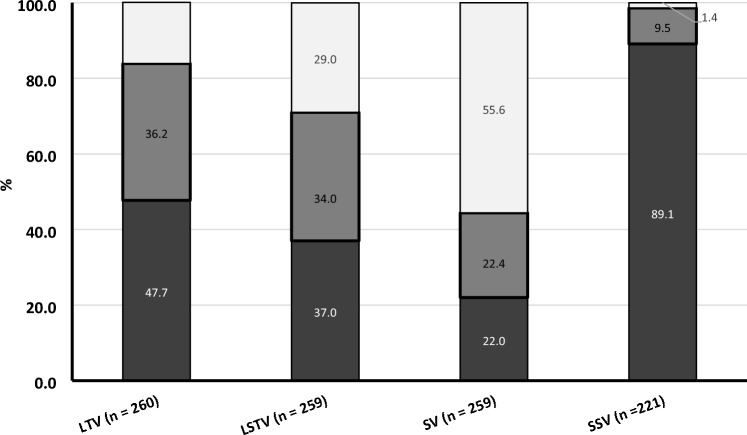 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsScoliosis diagnosis and treatment · Spinal Fractures and Fixation Techniques · Spine and Intervertebral Disc Pathology