A simple technique using a Venflon to fix fractures of the glenoid
A Kapasi, C Uzoigwe, D Barlow, A McMurtrie

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
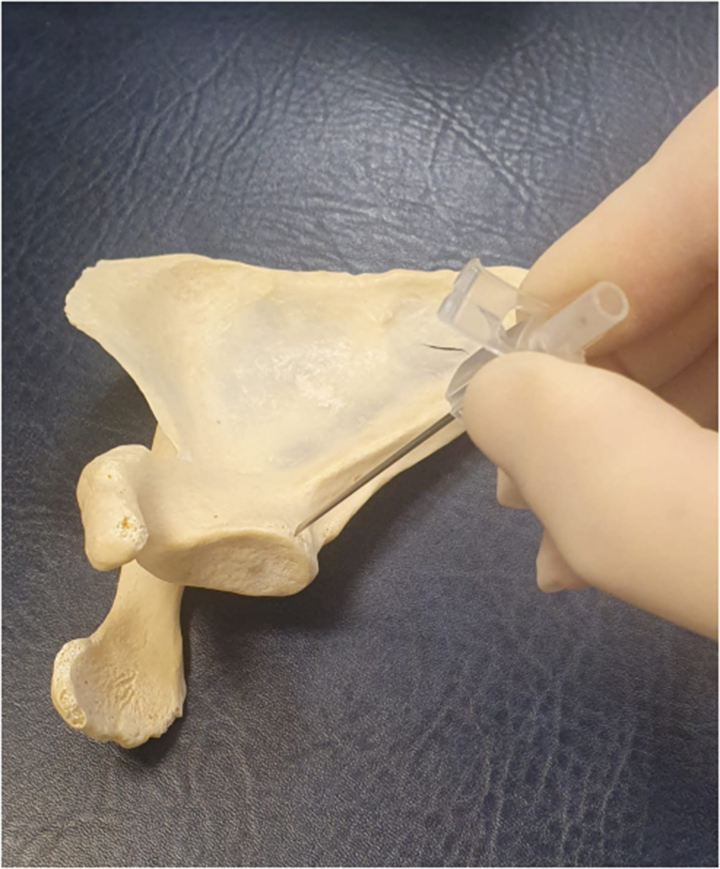 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3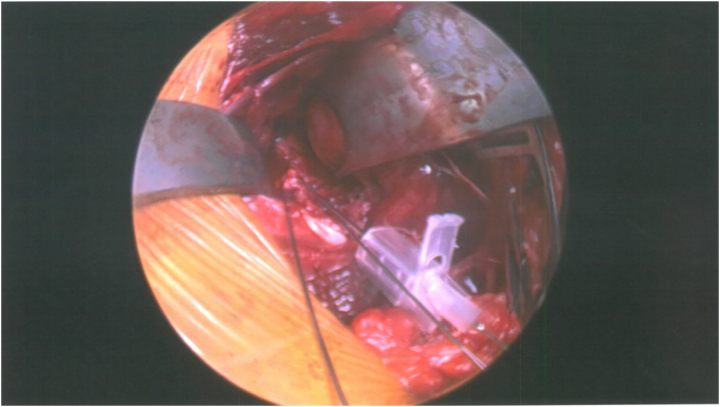 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsShoulder Injury and Treatment · Shoulder and Clavicle Injuries · Nerve Injury and Rehabilitation
Background
Glenoid fractures account for 10%–48% of scapular fractures.^1^ Fractures representing more than 25% of the articular surface are associated with shoulder instability. Surgical fixation is indicated in these circumstances.^1,2^ This can be challenging given the glenoid size, its relation to the humeral head and the proximity of neurovascular structures.
By necessity, fixation instrumentation is of small calibre. The surrounding soft tissues can impede achieving the optimum trajectory of fixation devices. This is compounded by the orientation of the glenoid and the position of fracture fragments.^3^ We describe a technique for facilitating the positioning of screws during glenoid fixation.
Technique
Glenoid fracture fixation can be achieved with narrow-diameter cannulated-screw systems. This employs preliminary non-rigid guide K-wires of between 0.9 and 1.2mm in size, to ensure correct screw positioning. To aid in achieving the correct wire orientation, the wire can be passed through an orange (14-gauge) cannula needle, which has an internal diameter of 1.6mm. The cannula needle can be used to both place and orient the K-wire in the most appropriate position to achieve optimum fixation (Figures 1–4).
Discussion
The needle point sinks into the bone and therefore is less likely to displace during passing of the K-wire. Furthermore, the cannula needle is much more rigid than the K-wire, which allows the surgeon to direct the wire with greater ease. The cannula also acts as a tissue guide, preventing soft tissue entanglement in the rotating wire. This technique we describe is particularly useful given the limited accessibility of the glenoid.
Orange cannula with sleeve removed positioned against glenoid rim
Guidewire passed down cannula
Cannula used to position and orientate the guidewire
Intraoperative photograph of left glenoid fixation using cannula technique
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ström P. Glenoid fractures of the shoulder. EFORT Open Rev 2020; 5: 620–623.33204504 10.1302/2058-5241.5.190057 PMC 7608577 · doi ↗ · pubmed ↗
- 2Itoi E, Lee SB, Berglund LJ et al. The effect of a glenoid defect on anteroinferior stability of the shoulder after Bankart repair: a cadaveric study. J Bone Joint Surg Am 2000; 82: 35–46.10653082 10.2106/00004623-200001000-00005 · doi ↗ · pubmed ↗
- 3Ao R, Jian Z, Zhou J et al. A comparison of deltopectoral versus Judet approach for glenoid exposure. J Shoulder Elbow Surg 2020; 29: 370–373.31466892 10.1016/j.jse.2019.06.015 · doi ↗ · pubmed ↗