Intra-operative Risk Factors Affecting Mortality after Heart Transplantation: A Referral Center Experience in Iran
Ali Sadeghpour Tabaei, Parham Hashemi

TL;DR
This study from Iran identifies intra-operative risk factors that increase mortality after heart transplants in both children and adults.
Contribution
The study provides new insights into specific intra-operative risk factors affecting post-transplant mortality in a single-center, long-term cohort.
Findings
Reoperation due to bleeding and defibrillation significantly increased one-month mortality risk in both children and adults.
ECMO use and ICU stay were associated with higher one-year mortality.
Readmission had a protective effect against one-month mortality.
Abstract
Heart transplantation is the preferred treatment for end-stage heart failure. This study investigated the intra-operative risk factors affecting post-transplantation mortality. This single-center retrospective cohort study examined 239 heart transplant patients over eight years, from 2011-2019, at the oldest dedicated cardiovascular center, Shahid Rajaee Hospital (Tehran, Iran). The primary evaluated clinical outcomes were rejection, readmission, and mortality one month and one year after transplantation. For data analysis, univariate logistic regression analyses were conducted. In this study, 107 patients (43.2%) were adults, and 132 patients (56.8%) were children. Notably, reoperation due to bleeding was a significant predictor of one-month mortality in both children (OR=7.47, P=0.006) and adults (OR=172.12, P<0.001). Moreover, the need for defibrillation significantly increased the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
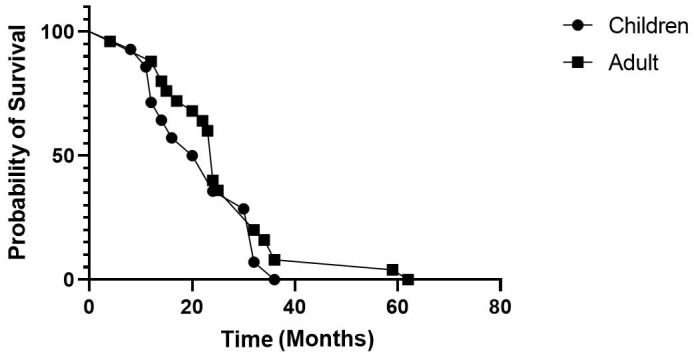 Figure 1
Figure 1| Variable | Children | Adult | |
|---|---|---|---|
| Mean±SD | Mean±SD | ||
| n (%) | n (%) | ||
| Age (years) | 10.7±4.3 | 31.2±9.9 | |
| Cross clamp time (minutes) | 82.5±32.0 | 81.3±26.8 | |
| LVEF (%) | 49.4±5.4 | 49.7±5.4 | |
| PAP (mmMg) | 38.4±8.4 | 38.4±9.2 | |
| Follow-up (months) | 28.7±15.4 | 36.6±18.0 | |
| Hospital stay (days) | 25.9±18.6 | 33.1±26.1 | |
| Intensive care unit stay (days) | 10.2±9.4 | 10.9±6.6 | |
| Sex | Male | 74 (56.1) | 73 (68.2) |
| Female | 58 (43.9) | 34 (31.8) | |
| Smoking | No | - | 96 (89.7) |
| Yes | - | 11 10.3) | |
| High blood pressure (BP>125/85) | No | - | 99 (92.5) |
| Yes | - | 8 (7.5) | |
| Diabetes mellitus (FBS>126) | No | - | 99 (92.5) |
| Yes | - | 8 (7.5) | |
| Right ventricular dysfunction (semi-quantitatively) | Non | 5 (3.8) | 8 (7.5) |
| Mild | 63 (47.7) | 47 (43.9) | |
| Moderate | 60 (45.5) | 47 (43.9) | |
| Sever | 4 (3.0) | 5 (4.7) | |
| Balloon pump | No | - | 106 (99.1) |
| Yes | - | 1 (0.9) | |
| ECMO | No | 119 (90.2) | 91 (85.0) |
| Yes | 13 (9.8) | 16 (15.0) | |
| Infection | No | 127 (96.2) | 104 (97.2) |
| Yes | 5 (3.8) | 3 (2.8) | |
| Re-operation for postoperative bleeding | No | 122 (92.4) | 88 (82.2) |
| Yes | 10 (7.6) | 19 (17.8) | |
| Re-transplantation | No | 131 (99.2) | 106 (99.1) |
| Yes | 1 (0.8) | 1 (0.9) | |
| Cardiac defibrillation | No defibrillation needed | 120 (90.9) | 89 (83.2) |
| Heart was defibrillated | 12 (9.1) | 18 (16.8) | |
| Re-admission | No | 17 (12.9) | 27 (25.2) |
| Yes | 115 (87.1) | 80 (74.8) | |
| Transplant rejection | No | 60 (45.5) | 36 (33.6) |
| At least mild rejection | 72 (54.5) | 71 (66.4) | |
| One month death | Survived more than 30 days | 118 (89.4) | 82 (76.6) |
| Death within 30 days | 14 (10.6) | 25 (23.4) | |
| One year death | Survived more than one year | 114 (86.4) | 82 (76.6) |
| Died in the first year | 18 (13.6) | 25 (23.4) | |
| Total | 132 (100) | 107 (100) | |
| Variable | Class | Class | OR | 95% CI | P value |
|---|---|---|---|---|---|
| Sex | Children | Male | Reference group | - | 0.630 |
| Female | 1.31 | (0.43-3.98) | |||
| Adult | Male | Reference group | - | 0.315 | |
| Female | 1.61 | (0.64-4.09) | |||
| Smoking | Children | No | - | - | |
| Yes | - | - | |||
| Adult | No | Reference group | - | 0.747 | |
| Yes | 1.26 | (0.31-5.16) | |||
| High blood pressure (BP>125/85) | Children | No | - | - | |
| Yes | - | - | |||
| Adult | No | Reference group | - | 0.461 | |
| Yes | 0.45 | (0.05-3.81) | |||
| Diabetes mellitus (FBS>126) | Children | No | - | - | |
| Yes | - | - | |||
| Adult | No | Reference group | - | 0.910 | |
| Yes | 1.10 | (0.21-5.83) | |||
| Right ventricular dysfunction (semi-quantitatively) | Children | None | 0.00 | (0.00-0.00) | >0.999 |
| Mild | 0.38 | (0.03-4.12) | 0.422 | ||
| Moderate | 0.33 | (0.03-3.73) | 0.373 | ||
| Sever | Reference group | - | - | ||
| Adult | None | 0.00 | (0.00-0.00) | >0.999 | |
| Mild | 0.31 | (0.04-2.15) | 0.235 | ||
| Moderate | 0.70 | (0.11-4.66) | 0.715 | ||
| Sever | Reference group | - | - | ||
| ECMO | Children | No | Reference group | - | 0.002 |
| Yes | 7.64 | (2.07-28.25) | |||
| Adult | No | Reference group | - | <0.001 | |
| Yes | 12.10 | 3.64-40.20 | |||
| Infection | Children | No | Reference group | - | 0.054 |
| Yes | 6.39 | 0.97-42.10 | |||
| Adult | No | Reference group | - | 0.682 | |
| Yes | 1.67 | 0.14-19.19 | |||
| Re-operation for postoperative bleeding | Children | No | Reference group | - | 0.006 |
| Yes | 7.47 | 1.80-30.92 | |||
| Adult | No | Reference group | - | 0.132 | |
| Yes | 2.27 | 0.78-6.59 | |||
| Defibrillation | Children | No | Reference group | - | <0.001 |
| Yes | 38.00 | 8.88-162.67 | |||
| Adult | No | Reference group | - | <0.001 | |
| Yes | 172.12 | 20.18-188.25 | |||
| Re-admission | Children | No | Reference group | - | <0.001 |
| Yes | 0.02 | 0.003-0.07 | |||
| Adult | No | Reference group | - | <0.001 | |
| Yes | 0.004 | 0.001-0.03 | |||
| Cross clamp time (min) | Children | No | Reference group | - | 0.960 |
| Yes | 1.00 | 0.97-1.03 | |||
| Adult | No | Reference group | - | 0.066 | |
| Yes | 1.06 | 0.99-1.12 | |||
| Follow-up (months) | Children | 1.02 | 0.96-1.10 | 0.501 | |
| Adult | 1.01 | 0.95-1.08 | 0.783 | ||
| LVEF (%) | Children | 0.98 | 0.89-1.09 | 0.748 | |
| Adult | 0.96 | 0.89-1.04 | 0.328 | ||
| PAP (mmMg) | Children | 0.97 | 0.90-1.04 | 0.409 | |
| Adult | 0.98 | 0.93-1.04 | 0.559 | ||
| Intensive care unit stay (days) | Children | 1.07 | 1.01-1.13 | 0.029 | |
| Adult | 1.04 | 0.97-1.10 | 0.297 |
| Variable | Class | Class | OR | 95% CI | P value |
|---|---|---|---|---|---|
| Sex | Children | Male | Reference group | - | 0.578 |
| Female | 1.33 | 0.49-3.59 | |||
| Adult | Male | Reference group | - | 0.315 | |
| Female | 1.61 | 0.64-4.09 | |||
| Smoking | Children | No | - | - | |
| Yes | - | - | |||
| Adult | No | Reference group | - | 0.747 | |
| Yes | 1.26 | 0.31-5.16 | |||
| High blood pressure (BP>125/85) | Children | No | - | - | |
| Yes | - | - | |||
| Adult | No | Reference group | - | 0.461 | |
| Yes | 0.45 | 0.05-3.81 | |||
| Diabetes mellitus (FBS>126) | Children | No | - | - | |
| Yes | - | - | |||
| Adult | No | Reference group | - | 0.910 | |
| Yes | 1.10 | 0.21-5.83 | |||
| Right ventricular dysfunction (semi-quantitatively) | Children | None | 0.25 | 0.01-4.73 | 0.355 |
| Mild | 0.12 | 0.02-1.03 | 0.054 | ||
| Moderate | 0.15 | 0.02-1.25 | 0.080 | ||
| Sever | Reference group | - | |||
| Adult | None | 0.00 | (0.00-0.00) | >0.999 | |
| Mild | 0.31 | 0.04-2.15 | 0.235 | ||
| Moderate | 0.70 | 0.11-4.66 | 0.715 | ||
| Sever | Reference group | - | - | ||
| ECMO | Children | No | Reference group | - | 0.001 |
| Yes | 7.64 | 2.20-26.49 | |||
| Adult | No | Reference group | - | <0.001 | |
| Yes | 12.10 | 3.64-40.20 | |||
| Infection | Children | No | Reference group | - | 0.107 |
| Yes | 4.62 | 0.72-29.84 | |||
| Adult | No | Reference group | - | 0.682 | |
| Yes | 1.67 | 0.14-19.19 | |||
| Re-operation for postoperative bleeding | Children | No | Reference group | - | 0.020 |
| Yes | 5.14 | 1.29-20.49 | |||
| Adult | No | Reference group | - | 0.132 | |
| Yes | 2.27 | 0.78-6.59 | |||
| Defibrillation | Children | No | Reference group | - | <0.001 |
| Yes | 22.00 | 5.63-86.03 | |||
| Adult | No | Reference group | - | <0.001 | |
| Yes | 172.12 | 20.18-186.25 | |||
| Re-admission | Children | No | Reference group | - | <0.001 |
| Yes | 0.04 | 0.01-0.12 | |||
| Adult | No | Reference group | - | <0.001 | |
| Yes | 0.004 | 0.001-0.026 | |||
| Cross clamp time (min) | Children | No | Reference group | - | 0.645 |
| Yes | 1.01 | 0.98-1.03 | |||
| Adult | No | Reference group | - | 0.066 | |
| Yes | 1.06 | 0.99-1.12 | |||
| Follow-up (months) | Children | 0.96 | 0.90-1.04 | 0.337 | |
| Adult | 1.01 | 0.95-1.08 | 0.783 | ||
| LVEF (%) | Children | 0.96 | 0.88-1.04 | 0.291 | |
| Adult | 0.96 | 0.89-1.04 | 0.328 | ||
| PAP (mmMg) | Children | 0.96 | 0.90-1.03 | 0.252 | |
| Adult | 0.98 | 0.93-1.04 | 0.559 | ||
| Intensive care unit stay (days) | Children | 1.06 | 1.01-1.12 | 0.033 | |
| Adult | 1.04 | 0.97-1.10 | 0.297 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTransplantation: Methods and Outcomes · Organ Transplantation Techniques and Outcomes · Mechanical Circulatory Support Devices
What’s Known
- Predictors of long-term survival after heart transplantation include a recipient age of less than 55 years, a younger donor age, a shorter ischemic period, a white race, and an annual center volume of more than nine heart transplantations.
What’s New
- The present study revealed that intra-operative events, such as the need for reoperation due to bleeding after heart transplantation, were associated with a higher risk of early and one-year mortality. Additionally, the requirement for intra-operative defibrillation was found to significantly increase the risk of mortality in heart transplant recipients both after one month and one year.
Introduction
Cardiovascular diseases are the leading cause of death and mortality in many societies worldwide. ^ 1 ^ Despite significant advancements in durable mechanical circulatory support (MCS), heart transplantation (HTx) remains the most valuable therapeutic option for patients with end-stage heart failure. ^ 2 , 3 ^ The main limitation of this treatment option is the scarcity of donor organs. The most common indications for heart transplantation are ischemic and non-ischemic cardiomyopathy (92%), valvular heart disease (2-3%), adult congenital heart disease (2%), retransplantation (2%), and other types of end-stage heart disease. ^ 4 ^ More than 6,000 heart transplantation procedures are performed annually worldwide, with an average post-transplant survival exceeding 12 years. ^ 5
The highest risk of death occurs during the first year following heart transplantation. Early 30-day mortality is predominantly due to infection, graft failure, and multi-organ failure, which is frequently caused by graft failure. ^ 9 ^ Major long-term causes of death include coronary allograft vasculopathy (CAV) and malignancies. In Iran, reported survival rates for heart transplant recipients were 80% for one month, 59.5% for one year, and 50% for five years. ^ 10 ^ In comparison, global statistics from western countries showed that one-month mortality was approximately 5-10%, and one-year survival rate was about 85%. ^ 11 ^
Several studies reported that the quality of life for heart transplant recipients increased following the transplantation procedure. ^ 12 , 13 ^ However, this improvement is often accompanied by an increased risk of complications and, ultimately, mortality. ^ 14 , 15 ^ Research indicated that the majority of deaths following heart transplantation occurred within the first 6-12 months, after which the risk of death decreased to 3% per year, and the quality of life typically enhanced after the first year. ^ 13 ^ According to the findings of a study, acute rejection of heart transplants due to antibodies (AMR) accounted for 8% of post-transplantation mortalities. ^ 9 ^ Infections are a common complication following heart transplantation, primarily due to immunosuppression. A previous study reported that up to 13.4% of deaths within the first month after transplantation were attributed to non-cytomegalovirus (CMV) infections, with the predominant infection being septicemia caused by bacteria. ^ 6 ^
In the first year after transplantation, the mortality rate due to infection remains high at 31.3% but subsequently decreases to 10-13% per year. ^ 6 ^ After the first year, CAV is the leading cause of death. ^ 16 ^ Five years following transplantation, malignancy becomes the fourth leading cause of death. ^ 6 ^ Some studies reported that up to 28% of patients would develop malignancies within ten years after transplantation. ^ 6 , 17 ^ Predictors of long-term survival include recipient age under 55 years, younger donor age, shorter ischemic time, white race, and an annual center volume of more than nine heart transplants. ^ 18 ^
As the number of heart transplant recipients continues to rise, it is imperative to conduct comprehensive research and planning to identify potential risk factors related to graft rejection and post-transplant mortality. This will enhance survival rates, reduce complications, and improve the quality of life for these individuals. Therefore, this study aimed to identify the risk factors associated with one-month and one-year mortality following transplantation, with a special emphasis on intra-operative events. Additionally, it sought to determine the survival rate following transplantation.
Patients and Methods
This retrospective cohort study was conducted at a single center, involving 239 patients, including both adults and children, over eight years (2011-2019). It was a part of the heart transplantation program at Iran’s oldest specialized cardiovascular center, Shahid Rajaee Cardiovascular Center, Tehran, Iran. The inclusion criteria were extremely debilitated pediatric and adult patients who underwent heart transplantation and had irreversible heart failure, which was defined as having a cardiac output of less than 2.2 L/min, an ejection fraction of less than 20%, maximal oxygen consumption of less than 14 mL/Kg/min, and a pulmonary capillary wedge pressure higher than 25 mmHg.
The exclusion criteria included heart transplant patients from earlier years (before 2011), when the annual number of transplantations was limited, and the center may not have fully mastered the procedure’s learning curve.
The outcome measures included the occurrence of one-month death or early postoperative mortality, which was defined as death occurring during the procedure or within the first 30 days after the operation. One-year death, which included both early mortality and death within the first year infection, as defined by the presence of purulent wound drainage, was another outcome measure. ICU and hospital stay were additional outcome measures assessed in terms of days. Any hospital admission lasting more than 6 hours following post-operative hospital discharge was considered a readmission. The presence of positive pathological findings, such as mild, moderate, or severe, which were obtained from endocardial biopsies, characterized rejection as an outcome measure. The initial endocardial biopsy was performed 7-10 days after the operation and subsequently every 4 months, as well as whenever any clinical deterioration was observed. Patients were typically discharged, while they were on a regimen of corticosteroids, mycophenolate mofetil, and tacrolimus. Any episode of rejection was managed by administering bolus doses of methylprednisolone as well as modifying or increasing the doses of oral immunosuppressants.
This study was approved by the Ethics Committee of Iran University of Medical Sciences (IR.IUMS.FMD.REC.1400.407). The Research Ethics Committee did not require the patient’s written informed consent due to the retrospective nature of the study, and the anonymous confidential use of the data.
Statistical Analysis
The data were analyzed using SPSS software version 16 (SPSS Inc., Chicago, Illinois, United States). The results were expressed as number, percentage, mean±SD, and minimum-maximum, where required. A univariate logistic regression model was employed to investigate the correlations between dependent and predictive variables, with the calculation of odds ratios (OR) and confidence intervals (CI). Additionally, Kaplan-Meier analysis was used to compare survival probabilities between children and adult patients. P≤0.05 was considered statistically significant.
Results
Table 1 displays the study variables. Out of a total of 239 patients, 147 (61.5%) were males, and 92 (38.5%) were females. There was no significant sex difference in rejection rates, 59.2% for males and 60.9% for females (P=0.796). Re-transplantation was required in 2 (0.8%) of the patients. Of all patients, 20 (8.3%) patients required permanent pacemakers, while 29 (12.1%) underwent reoperation for postoperative hemorrhage. Eight (3.3%) patients experienced sternal wound infections, which resulted in a longer mean hospital stay (42.88 vs. 29.10 days). In total, 143 patients (59.8%) had at least one biopsy that revealed rejection. To maintain normal sinus rhythm, 30 (12.6%) patients had cardiac defibrillation after aortic cross-clamp removal. At least one readmission post-transplantation was reported in the records of 195 (81.6%) patients. Three (1.25%) patients were diagnosed with post-transplant lymphoproliferative disorder. There were no reports of skin or other types of malignancies. Additional demographic and clinical findings of children and adults are presented in table 1.
Within 30 days, 39 (16.3%) patients passed away. Adults exhibited a higher one-month mortality rate (23.4% vs. 10.6%) than children (P=0.008). A logistic regression model analysis for one-month mortality is shown in table 2. The OR for the use of extracorporeal membrane oxygenation was 7.64 for children (P=0.002), and for adults was (OR=12.10, P<0.001). Children had an OR of 7.47 for re-operation for postoperative bleeding (P=0.006), and the OR for administering defibrillation was 38.00 and 172.12 for children and adults, respectively (P<0.001 for both children and adults). Furthermore, the ICU stay OR was 1.07 days (P=0.029) in children. Readmission showed a weak protective effect (OR=0.02; P<0.001) for children and (OR=0.004; P<0.001) for adults (table 2).
In the first year, 43 (18.0%) deaths were reported. The results indicated that the use of extracorporeal membrane oxygenation had an odds ratio of 7.64 in children (P=0.001) and OR=12.10 (P<0.001) in adults. As indicated in table 3, reoperation due to postoperative bleeding had an odds ratio of 5.14 in children (P=0.020). Patients undergoing intra-operative defibrillation had odds ratios of 22.00 and 172.12 for children and adults, respectively (P<0.001 for both children and adults). Furthermore, the OR of ICU stay was 1.06 in children (P=0.033).
According to the results of the Kaplan-Meier analysis, the median survival after surgery was found to be 22 months for children and 24 months for adults. As indicated in figure 1, the difference in survival medians between the two groups was not statistically significant (P=0.284).
Survival probability curve of children and adult patients is indicated over time by age groups.
Discussion
In the present study, the proportion of male to female patients was 61.5% to 38.5%, with a greater number of female patients than in a recent study in Iran that reported 20.8% female patients. ^ 8 ^ The one-month mortality rate was 16.3%, which was higher than the rates reported in other previous studies, typically ranged from 5% to 10%. ^ 4 , 19 ^ This variance in our 30-day mortality rate, which was higher than in previous studies, could be attributed to the unique structure of the studied center. While a large number of heart transplantations were performed in this center annually (over 15 Htx per year), it includes approximately eight different surgical teams. Therefore, the diversity in teams could lead to variations in transplant outcomes due to the differences in their methodologies and experiences.
The present study found no significant differences in the outcomes between male and female recipients. Although we initially hypothesized that female recipients might experience better outcomes, based on the fact that many organ donors are young male motorcycle accident victims, potentially resulting in a higher cardiac mass per body surface area, and the theory that a weaker immune system might reduce rejection intensity, this study did not substantiate this hypothesis.
There were significant differences in one-month mortality rates between adults and children. Adults had higher one-month mortality rates (23.4% vs. 10.6%). However, there were no significant differences between adult and child patients in other key outcomes, including one-year mortality and transplant rejection rates. A study conducted by Foroutan and others revealed that recipient age, congenital etiology, creatinine levels, MCS beats, donor age, and sex mismatch (specifically, from female donor to male recipient) were all associated with one-year mortality after heart transplantation. ^ 20 ^
The objective of the present study was to investigate the impact of intra-operative variables on patient mortality following heart transplantation, which differed from previous studies that focused primarily on recipient or donor demographic factors. While there has been limited research on the risk factors associated with patient mortality after heart transplantation, the present study was the first of its kind in Iran, which addressed this crucial issue.
According to the findings of the research, the potential risk factors associated with early 30-day mortality were the use of extracorporeal membrane oxygenation, re-operation for postoperative hemorrhage, heart defibrillation, ICU stay, and readmission. This was in contrast with previous studies, which found an association between early post-heart transplantation (Htx) mortality and other factors such as graft failure, infection, and multi-organ failure. ^ 4 , 21 ^
The findings of the present study indicated that re-operation for postoperative bleeding in children and heart defibrillation in both children and adults significantly increased the likelihood of one-month mortality after heart transplantation by 7.47, 38.00, and 172.12 times, respectively. Concerning the relationship between postoperative hemorrhage and increased mortality, it was found that transfusion blood components, especially non-irradiated packed red blood cells (RBC), could result in rejection. However, the strong association observed in this study could be attributed to the selection of poorly conditioned end-stage heart failure patients with multi-organ failure, such as coagulopathy. In contrast to the study conducted by Doumouras and colleagues, ^ 22 ^ which reported a higher frequency of bleeding after transplantation in the adult congenital heart group, this wasn’t the case in our study.
The use of ECMO in the present study was a strong predictor of early mortality, presumably due to its predominant use in patients with severe right ventricle (RV) failure, indicating inadequate myocardial protection. Interestingly, ECMO was also associated with higher one-year mortality, which might be attributed to the long-term immunologic effects of ECMO-related transfusions.
Readmission had a protective effect in this study, as it reduced the 30-day and one-year mortality rates in both children and adults. This finding was in contrast with the findings of Lopez-Sainz and others. ^ 23 ^ It was important to emphasize that readmission in our center did not always indicate clinical deterioration. It might include scenarios such as biopsies or visits lasting more than 6 hours, which could contribute to its protective effect.
These findings also indicated that the use of extracorporeal membrane oxygenation, re-operation for postoperative bleeding, heart defibrillation, ICU stay, and readmission were identified as potential risk factors associated with one-year mortality. Similar to early mortality, re-operation for postoperative bleeding and heart defibrillation, in particular, significantly increased the likelihood of one-year mortality after heart transplantation. In contrast, readmission had a protective effect by reducing the one-year mortality rate.
Several studies investigated the role of implantable cardiac defibrillators (ICDs) in preventing mortality in heart failure patients. ^ 24 , 25 ^ However, the present study focused on a different aspect. Intra-operative cardiac defibrillation is a procedure that might be required shortly after graft anastomosis and within minutes of initiating blood perfusion into the graft’s coronary arteries. Its purpose is to restore the normal sinus rhythm of the newly implanted heart. In the present research, defibrillation was required in 30 of the transplanted hearts (12.80%) to maintain normal sinus rhythm. Interestingly, this finding was not correlated with ischemic time, patient age, or other patient factors; yet, it had an adverse impact on mortality. Several studies recommended primary cardiac defibrillation during cardiopulmonary resuscitation (rather than post-heart surgery) as a measure to prevent the depletion of myocardial glycogen reserves. ^ 26
- 28 ^ While many surgeons advocate early defibrillation to prevent left ventricular distention, a study conducted by Xie and colleagues demonstrated that heart defibrillation could lead to myocardial membrane damage and disrupt calcium homeostasis pumps. ^ 29 ^ Therefore, it remained unclear to us whether the need for defibrillation was a result or cause of an adverse event.
While the demographic characteristics of donors and recipients were frequently discussed in the literature, the importance of intra-operative events in heart transplantation outcomes was overlooked. Hence, there is an obvious need for further research in this area in the future. One of the main strengths of the present study was its pioneering nature in Iran, with a large sample size and two distinct groups of children and adults. However, it is crucial to highlight that due to differences in surgical team expertise, the present data might lack homogeneity.
Conclusion
No specific sex was associated with poorer outcomes. The use of extracorporeal membrane oxygenation, reoperations for bleeding, defibrillation after cross-clamp removal, and ICU stay were risk factors for both one-month and one-year mortality. Interestingly, readmission had a modest protective effect.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Veen KM Zijderhand CF Caliskan K Schoonen T Mokhles MM Bekkers J Aetal Biatrial vs Bicaval orthotopic Heart Transplantation: A Systematic Review and Meta-Analysis Determinants of outcome in patients with tricuspid valve 202027110.1016/j.athoracsur.2019.12.04832035050 · doi ↗ · pubmed ↗
- 2Ponikowski P Voors AA Anker SD Bueno H Cleland JGF Coats AJ Setal 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC Eur Heart J 201637212920010.1093/eurheartj/ehw 12827206819 · doi ↗ · pubmed ↗
- 3Jasseron C Lebreton G Cantrelle C Legeai C Leprince P Flecher Eetal Impact of Heart Transplantation on Survival in Patients on Venoarterial Extracorporeal Membrane Oxygenation at Listing in France Transplantation 201610019798710.1097/TP.000000000000126527306536 · doi ↗ · pubmed ↗
- 4Taylor DO Stehlik J Edwards LB Aurora P Christie JD Dobbels Fetal Registry of the International Society for Heart and Lung Transplantation: Twenty-sixth Official Adult Heart Transplant Report-2009 J Heart Lung Transplant 20092810072210.1016/j.healun.2009.08.01419782283 · doi ↗ · pubmed ↗
- 5Bhatia DS Bowen JC Money SR Van Meter CH Jr.Mc Fadden PM Kot J Betal The incidence, morbidity, and mortality of surgical procedures after orthotopic heart transplantation Ann Surg 199722568693-4[ PMC Free Article ]10.1097/00000658-199706000-000069230809 PMC 1190870 · doi ↗ · pubmed ↗
- 6Yusen RD Edwards LB Dipchand AI Goldfarb SB Kucheryavaya AY Levvey B Jetal The Registry of the International Society for Heart and Lung Transplantation: Thirty-third Adult Lung and Heart-Lung Transplant Report-2016; Focus Theme: Primary Diagnostic Indications for Transplant J Heart Lung Transplant 20163511708410.1016/j.healun.2016.09.00127772669 · doi ↗ · pubmed ↗
- 7Mc Cartney SL Patel C Del Rio JM Long-term outcomes and management of the heart transplant recipient Best Pract Res Clin Anaesthesiol 2017312374810.1016/j.bpa.2017.06.00329110796 · doi ↗ · pubmed ↗
- 8Ahmadi ZH Shafaghi S Mandegar MH Salehi M Sharif Kashani B Naghashzadeh Fetal The Cost of Heart Transplant in Iran: A Multicenter Analysis Int J Organ Transplant Med 202112239[ PMC Free Article ]35509719 PMC 9013497 · pubmed ↗