Anti-neutrophil Cytoplasmic Antibody-Negative Rapid Progressive Glomerulonephritis With Mild Pathological Presentation in an Older Patient: A Case Report
Ryuichi Ohta, Keita Inoue, Chiaki Sano

TL;DR
This case report describes a rare instance of a kidney disease in an older man without typical biomarkers, highlighting the challenges in diagnosis and treatment.
Contribution
The case emphasizes the importance of tailored treatment approaches for ANCA-negative RPGN in resource-limited settings.
Findings
The patient showed significant renal function recovery after intensive immunosuppressive therapy.
The case illustrates the complexity of managing RPGN with coexisting nephritic and nephrotic syndromes.
Successful treatment required a dynamic and persistent approach despite initial treatment failure.
Abstract
This case report discusses the management of anti-neutrophil cytoplasmic antibodies (ANCA)-negative rapid progressive glomerulonephritis (RPGN) in a 68-year-old man with a complex medical history, presenting with fatigue, edema, and acute renal failure. Despite the absence of positive biomarkers for specific RPGN types, the clinical progression suggested microscopic polyangiitis, leading to intensive immunosuppressive therapy with cyclophosphamide and rituximab. The patient's condition was further complicated by the coexistence of nephritic and nephrotic syndromes, requiring nuanced management strategies, including prolonged hemodialysis. After initial treatment failure, remission was eventually achieved, allowing cessation of dialysis and significant recovery of renal function. This case highlights the challenges of diagnosing and managing ANCA-negative RPGN, particularly the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
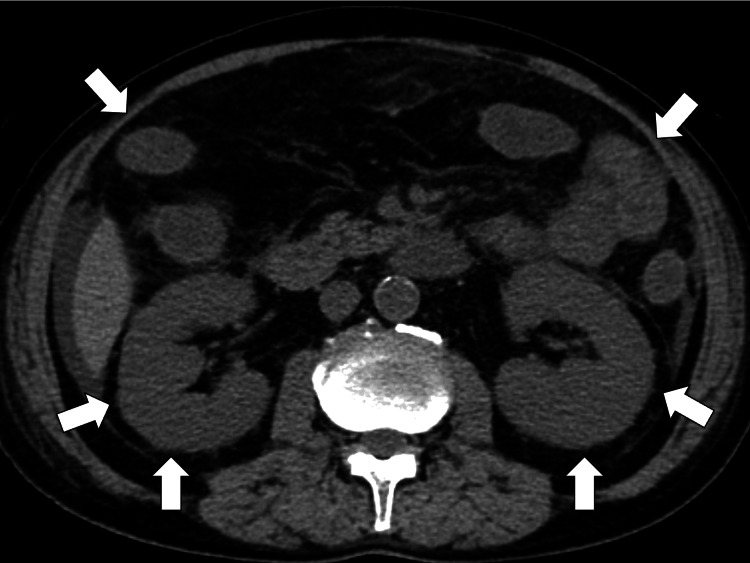 Figure 1
Figure 1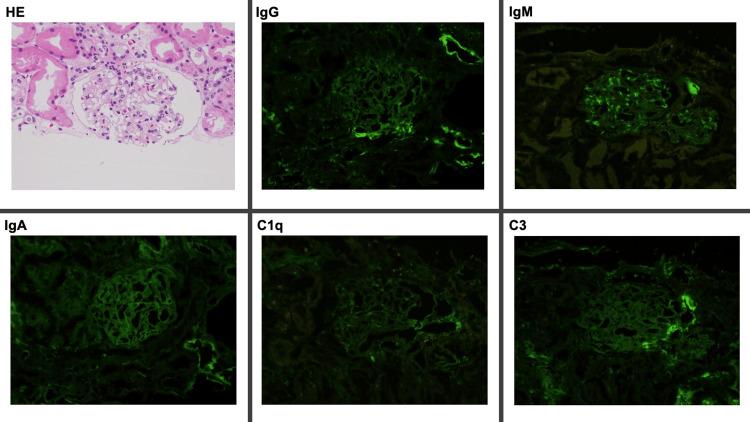 Figure 2
Figure 2| Parameter | Level | Reference |
| White blood cells | 10.50 | 3.5-9.1×103/μL |
| Neutrophils | 82.7 | 44.0-72.0% |
| Lymphocytes | 9.9 | 18.0-59.0% |
| Monocytes | 6.2 | 0.0-12.0% |
| Eosinophils | 0.6 | 0.0-10.0% |
| Basophils | 0.6 | 0.0-3.0% |
| Red blood cells | 5.02 | 3.76-5.50×106/μL |
| Hemoglobin | 16.2 | 11.3-15.2 g/dL |
| Hematocrit | 46.7 | 33.4-44.9% |
| Mean corpuscular volume | 92.9 | 79.0-100.0 fL |
| Platelets | 24.4 | 13.0-36.9×104/μL |
| Erythrocyte sedimentation rate | 82 | 2-10 mm/hour |
| Total protein | 4.5 | 6.5-8.3 g/dL |
| Albumin | 1.5 | 3.8-5.3 g/dL |
| Total bilirubin | 0.3 | 0.2-1.2 mg/dL |
| Aspartate aminotransferase | 20 | 8-38 IU/L |
| Alanine aminotransferase | 11 | 4-43 IU/L |
| Alkaline phosphatase | 98 | 106-322 U/L |
| γ-Glutamyl transpeptidase | 36 | <48 IU/L |
| Lactate dehydrogenase | 356 | 121-245 U/L |
| BUN | 51.8 | 8-20 mg/dL |
| Creatinine | 1.76 | 0.40-1.10 mg/dL |
| eGFR | 31.1 | >60.0 mL/min/1.73m2 |
| Serum Na | 142 | 135-150 mEq/L |
| Serum K | 3.8 | 3.5-5.3 mEq/L |
| Serum Cl | 108 | 98-110 mEq/L |
| Serum Ca | 7.0 | 8.8-10.2 mg/dL |
| Serum P | 3.8 | 2.7-4.6 mg/dL |
| Serum Mg | 1.9 | 1.8-2.3 mg/dL |
| CK | 36 | 56-244 U/L |
| CRP | 3.02 | <0.30 mg/dL |
| TSH | 2.77 | 0.35-4.94 μIU/mL |
| Free T4 | 0.7 | 0.70-1.48 ng/dL |
| IgG | 601 | 870-1700 mg/dL |
| IgM | 56 | 35-220 mg/dL |
| IgA | 351 | 110-410 mg/dL |
| IgE | 135 | <173 mg/dL |
| HBs antigen | 0.0 | IU/mL |
| HBs antibody | 0.67 | mIU/mL |
| HBc antibody | 0.00 | S/CO |
| HCV antibody | 0.00 | S/CO |
| Syphilis treponema antibody | 0.00 | S/CO |
| SARS-CoV-2 antigen | Negative | Negative |
| Anti-nuclear antibody | 40 | <40 |
| Homogeneous | 40 | <40 |
| Speckled | 40 | <40 |
| C3 | 177 | 86-164 mg/dL |
| C4 | 61 | 17-45 mg/dL |
| Urine test | - | - |
| Leukocyte | Negative | Negative |
| Nitrite | Negative | Negative |
| Protein | (4+) | Negative |
| Glucose | Negative | Negative |
| Urobilinogen | Negative | Negative |
| Bilirubin | Negative | Negative |
| Ketone | Negative | Negative |
| Blood | (2+) | Negative |
| pH | 6.0 | - |
| Specific gravity | 1.050 | - |
| Granule cast | >10/LPF | Negative |
| Epithelial cast | >10/LPF | Negative |
| 24-hour urinary protein excretions | 17.41 g/day | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVasculitis and related conditions · Neutrophil, Myeloperoxidase and Oxidative Mechanisms · Renal Diseases and Glomerulopathies
Introduction
Rapid progressive glomerulonephritis (RPGN) is a critical renal disease that causes significant morbidity and mortality, necessitating immediate intervention to prevent irreversible kidney damage and dependency on hemodialysis [1]. The disease's varied etiology underscores the importance of prompt treatment initiation, even before the complete assessment of biomarkers and renal biopsy results [2]. The anti-neutrophil cytoplasmic antibodies (ANCA) biomarker plays a crucial role in diagnosing and managing RPGN, guiding clinicians in the prognosis and intensifying treatment with cyclophosphamide and rituximab in ANCA-positive cases [3,4].
However, managing ANCA-negative RPGN presents a considerable challenge, especially in settings with limited access to diagnostic resources like renal biopsies, often seen in rural areas [5,6]. This time, we experienced a case of ANCA negative RPGN in an older man. Based on the rapid clinical course, we suspected microscopic polyangiitis and used cyclophosphamide and rituximab intensively, leading to remission and avoiding constant hemodialysis. In addition, the treatment process was complicated due to the mixture of nephritic and nephrotic syndromes, needing nuanced treatments and prolonged hemodialysis. This case underscores the difficulties in diagnosing ANCA-negative RPGN and the importance of basing treatment decisions on the clinical course. It emphasizes the critical need for early and decisive intervention and waiting time for remission of RPGN from acute to chronic phrases, particularly in resource-limited settings, to achieve positive patient outcomes.
Case presentation
A 68-year-old man came to a rural community hospital with chief complaints of fatigue, bilateral lower leg edema, watery diarrhea, and dyspnea. One month before admission, he noticed bilateral edema of the lower legs. Severe days before admission, the patient had fatigue and exacerbation of the edema of lower legs progressing to ankles to thighs. At the same time, he began to have watery diarrhea several times a day without abdominal pain. On the day of admission, he felt dyspnea in the night and came to the hospital. He did not have headaches, fever, rash, joint pain, other infectious symptoms, or travel histories to other countries. The past medical histories were hypertension and dyslipidemia. The medications were lisinopril 5 mg daily and atorvastatin 5 mg daily. He smoked one pack a day for 30 years and drank alcohol daily for 40 years.
The vital signs at the visit were as follows: blood pressure, 167/97 mmHg; pulse rate, 65 beats/min; body temperature, 36.8°C; respiratory rate, 16 breaths/min; and oxygen saturation, 98% on room air. The patient was alert to time, place, and person. Physical examination showed slow pitting edema of bilateral lower legs without petechiae and purpura. No other abnormal neurological findings were noted. There were no apparent abnormalities in the chest or abdomen and no skin eruptions. The laboratory tests showed a high creatinine and blood urea nitrogen (BUN) level and a low serum albumin level with proteinuria, hematuria, and granular casts (Table 1).
Abdominal computed tomography (CT) showed the swelling of bilateral kidneys and diffuse edematous change of the small intestine and colon (Figure 1).
Abdominal CT showing the swelling of bilateral kidneys and diffuse edematous change of the small intestine and colon (white arrows)CT, computed tomography
Based on the clinical findings, the patient was diagnosed tentatively with RPGN, complicated with nephritic and nephrotic syndrome. The patient was treated with methylprednisolone 1000 mg intravenously for three days, followed by prednisolone 60 mg orally. Three days later, the additional laboratory data investigating the etiologies of RPGN showed negative results of anti-nuclear antibodies, ANCA, and anti-glomerular basement membrane antibodies. The same day, the renal biopsy was performed for further investigation. The patient’s creatinine and BUN elevated progressively, so intravenous cyclophosphamide of 500 mg was used for the remission of RPGN symptoms.
In the initial week of the admission, the patient’s diarrhea disappeared. Still, edema on the extremities was progressive, and his creatine and BUN increased gradually to creatinine levels of 6.62 mg/dL and 136 mg/dL. His dyspnea was exacerbated, and emergent hemodialysis was performed. The pathological findings of the kidneys showed mild infiltration of Immunoglobin M and G without any crescent formation (Figure 2).
The pathological findings of the kidneys showing mild infiltration of Immunoglobin M and G without any crescent formationC, complement; HE, hematoxylin & eosin
Based on the progressiveness of RPGN, the possibility of ANCA-negative microscopic polyangiitis was considered. On day 11, through a discussion with the patient and families, rituximab of 500 mg/week for four weeks was started.
After the remission of systemic inflammation from RPGN, considering a lower level of C-reactive protein (CRP), the persistency of urinary casts and proteinuria from nephritic and nephrotic syndrome continued and caused intravascular hypovolemic status, leading to persistent prerenal kidney injury. For the increase in the colloid osmotic pressure in vessels, intravenous albumin infusion started from day 10 of admission for five days. In addition, to increase the urine output, furosemide of 100 mg per day was started intravenously. However, on day 21 of the admission, his urine output completely stopped and depended on hemodialysis.
His treatment for RPGN was continued with hemodialysis and tapering prednisolone every two weeks. In addition, systemic management such as blood glucose level, blood pressure, and anemia continued through calorie intake control, anti-hypertensive medication (lisinopril 10 mg and amlodipine 10 mg daily), and hypoxia-inducible factor prolyl-hydroxylase inhibitor (daprodustat 6 mg daily). On day 52, his urine output restarted from 40 to 100 mL/day and gradually increased the following days. By day 60 of admission, his urine output increased by 1000 mL/day, and his hemodialysis was ended. On day 72 of admission, his renal functions improved to serum creatinine of 1.02 mg/dL and BUN of 21 mg/dL (estimated glomerular filtration rate of 49.2 mL/min/1.73 m^2^). He was discharged to his home with his usual lifestyle. His CRP fluctuated from 0.3 mg/dL to 2.1 mg/dL in outpatient department follow-up with no change of renal function.
Discussion
The management of ANCA-negative RPGN remains a formidable challenge, demanding a nuanced understanding of its pathophysiology and a strategic approach to treatment. As this case shows, the criticality of timely and aggressive treatment should be balanced, given the disease's potential for rapid progression to end-stage renal disease (ESRD) without appropriate intervention. In addition, as the initial intensive treatments are ineffective, the delay in the recovery of renal functions should be considered in the next few months. This case emphasizes the importance of a multifaceted treatment strategy that is dynamic and responsive to the patient's evolving clinical condition and the possibility of delayed recovery of renal functions in ANCA-RPGN.
The essence of treating ANCA-negative RPGN involves the integration of immunosuppressants and biological agents tailored to the individual patient's disease activity and clinical presentation [7]. The rationale behind this approach is grounded in the understanding that the pathogenesis of ANCA-negative RPGN, while still fully elucidated, involves an aberrant immune response leading to glomerular injury [8]. As this case shows, immunosuppressants, such as corticosteroids and cyclophosphamide, have been foundational in inducing remission, particularly in the early stages of the disease [6]. However, the advent of biological therapies offers a targeted approach to modulate specific pathways of the immune system involved in the disease process, potentially offering a more favorable side effect profile and improved outcomes to particular subsets of patients [9]. In this case, considering the progression of RPGN, cyclophosphamide and rituximab were used consecutively, eventually remitting the inflammation of ANCA-negative RPGN. Even if the initial pathological findings are mild, the speed of the progression of ANCA-negative RPGN demands intensive treatments through clinically assessing patients' conditions [10].
An essential advancement in the management of ANCA-negative RPGN is the emerging focus on the changes in laboratory and urinary findings, focusing on various clinical courses with a wide range of recovery [11]. This approach seeks to optimize therapeutic efficacy while minimizing toxicity, which is particularly important in a narrow therapeutic window [11]. For example, the use of rituximab, a monoclonal antibody targeting CD20+ B cells, has shown promise in some instances of RPGN where traditional therapies have failed [12]. However, the appearance of signs of recovery varies, regardless of patients' backgrounds and treatment [13]. As this case shows, patients' recovery could start two months after the initial intensive therapies. Predicting clinical courses in RPGN necessitates ongoing research and clinical trials to better understand the disease's molecular underpinnings and identify novel therapeutic targets [14]. General physicians should not give up on the possibility of recovering the renal function of ANCA-negative RPGN, even if the initial intensive treatments show no effects in several weeks [15,16].
The dynamic nature of RPGN, with potential clinical presentation and disease activity fluctuations, underscores the necessity for continuous monitoring and treatment adjustment. This iterative process involves regular assessment of renal function, proteinuria, hematuria, and other relevant biomarkers alongside clinical indicators of disease activity [17]. However, as this case shows, the prediction of the clinical courses from initial presentations may need to be corrected and may be challenged by various exacerbations. The coexistence of nephritic and nephrotic syndromes within the spectrum of RPGN poses particular challenges, necessitating an adjusted approach to management [18]. The differentiation between these syndromes is crucial, as it influences the choice of therapeutic agents and the management of complications [18]. For instance, the presence of significant proteinuria and hypoalbuminemia in nephrotic syndrome may warrant the use of angiotensin-converting enzyme inhibitors or angiotensin receptor blockers to reduce proteinuria, alongside specific measures to address the increased risk of thromboembolism and hyperlipidemia. As this case shows, as system-specific specialists, general physicians should monitor systemic findings such as blood pressure, anemia, and glucose levels and control each clinical finding continually, waiting for signs of recovery for several months [19].
Conclusions
In this case of ANCA-negative RPGN, the management challenges underscore the necessity for early and aggressive interventions to forestall ESRD, even in the absence of specific biomarkers. Our approach, utilizing cyclophosphamide and rituximab based on clinical progression rather than initial laboratory findings, highlights the critical role of dynamic treatment strategies in achieving remission. Despite the patient's complex presentation and prolonged dependency on dialysis, the eventual recovery of renal function emphasizes the importance of adaptability in treatment plans and continuous monitoring. This case reinforces the imperative for ongoing research and innovative therapeutic strategies to enhance outcomes in managing RPGN, particularly in resource-limited settings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Evidence-based clinical practice guidelines for rapidly progressive glomerulonephritis 2014 Clin Exp Nephrol Arimura Y Muso E Fujimoto S 3223412020162709913510.1007/s 10157-015-1218-8PMC 4891375 · doi ↗ · pubmed ↗
- 2What is new in the management of rapidly progressive glomerulonephritis?Clin Kidney J Greenhall GH Salama AD 143150820152581516910.1093/ckj/sfv 008PMC 4370308 · doi ↗ · pubmed ↗
- 3ANCA-associated vasculitis in a patient presenting with rapid progressive glomerulonephritis Cureus Singh A Everest S Nguyen L Kasari M 013202110.7759/cureus.20227 PMC 872931035004044 · doi ↗ · pubmed ↗
- 4Use of rituximab in management of rapidly progressive glomerulonephritis Cureus Cancarevic I Malik BH 012202010.7759/cureus.6820 PMC 705111832181067 · doi ↗ · pubmed ↗
- 5Anca negative pauci-immune crescentic glomerulonephritis and mixed connective tissue disease: a case study J Bras Nefrol Fernandes S Teixeira C Falcão LP 2452494220193089719310.1590/2175-8239-JBN-2019-0003 PMC 7427652 · doi ↗ · pubmed ↗
- 6ANCA-negative pauci-immune necrotizing glomerulonephritis: a case series and a new clinical classification Am J Kidney Dis Ronsin C Georges M Chapelet-Debout A 56687920223411956410.1053/j.ajkd.2021.03.027 · doi ↗ · pubmed ↗
- 7ANCA-negative pauci-immune crescentic glomerulonephritis Nat Rev Nephrol Chen M Kallenberg CG Zhao MH 313318520091939901910.1038/nrneph.2009.67 · doi ↗ · pubmed ↗
- 8Diagnostic and therapeutic approach in ANCA-associated glomerulonephritis: a review on management strategies Front Med (Lausanne) Molnár A Studinger P LedóN 884188920223572109310.3389/fmed.2022.884188 PMC 9205443 · doi ↗ · pubmed ↗