Neoadjuvant Immunotherapy Effectiveness in Patients With Microsatellite Instability-High (MSI-H) Gastric Cancer
Viacheslav A Chubenko, Alexander Y Navmatulya, Ivan A Gerk, Artem A Sarmatov, Vitaliy V Egorenkov, Ksenia A Shelekhova, Evgeny N Zykov, Vera V Chernobrivceva, Nikita M Volkov, Vladimir M Moiseyenko

TL;DR
This study shows that using immunotherapy before surgery is effective and safe for patients with a specific type of advanced stomach cancer.
Contribution
The study demonstrates the effectiveness of checkpoint inhibitor monotherapy as a neoadjuvant treatment for MSI-H gastric cancer.
Findings
77.8% of patients showed objective response to neoadjuvant CPI treatment.
100% of patients who underwent surgery had complete margin-free resection.
No disease progression was observed with a median follow-up of 33.7 months.
Abstract
Purpose This research work evaluates monotherapy with checkpoint inhibitors (CPI). as a neoadjuvant treatment for patients with Microsatellite Instability-High (MSI-H) locally advanced gastric cancer. Methods Here we present the results of the retrospective study from Napalkov Cancer Center over 4.5 years on patients with MSI-H locally advanced gastric cancer. A total of 566 patients were analyzed, 18 of whom were included in the research, focusing on clinical response rate, surgical pathology, ‘watch and wait’ strategy, and safety outcomes on an exploratory basis. Patients were assigned to four to eight neoadjuvant cycles of CPI, followed by surgery. Results The objective response to neoadjuvant CPI in patients with MSI-H gastric cancer was 77.8%. Complete response was achieved in five (27.8%) and partial response in nine (50%) patients, accordingly. Surgery was performed on 14…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
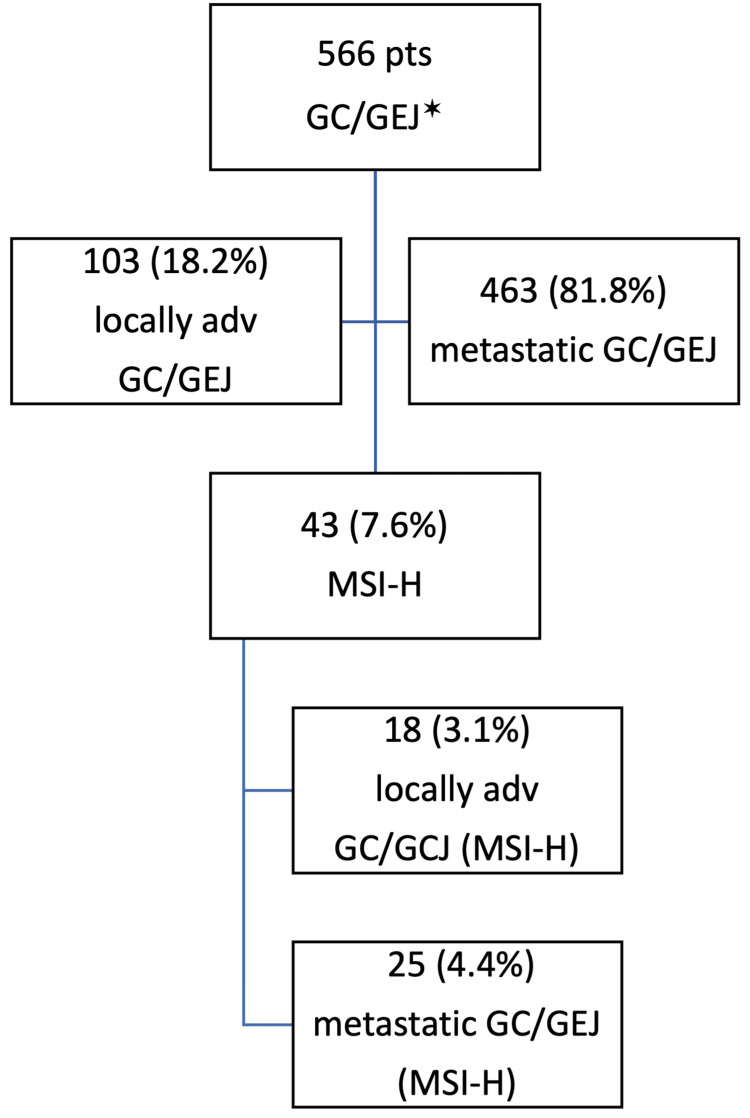 Figure 1
Figure 1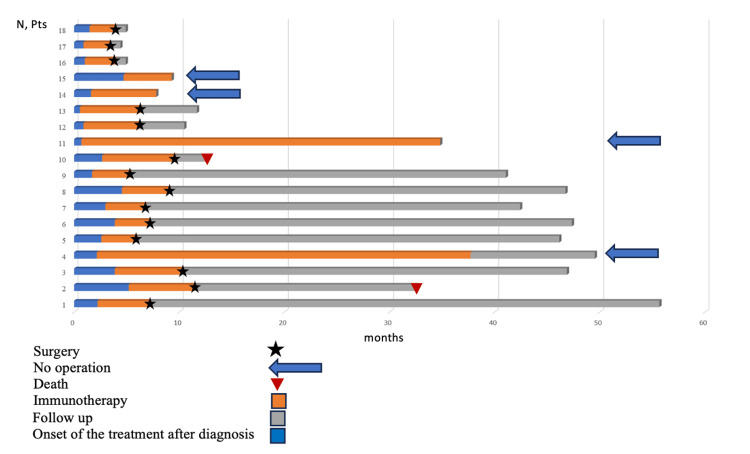 Figure 2
Figure 2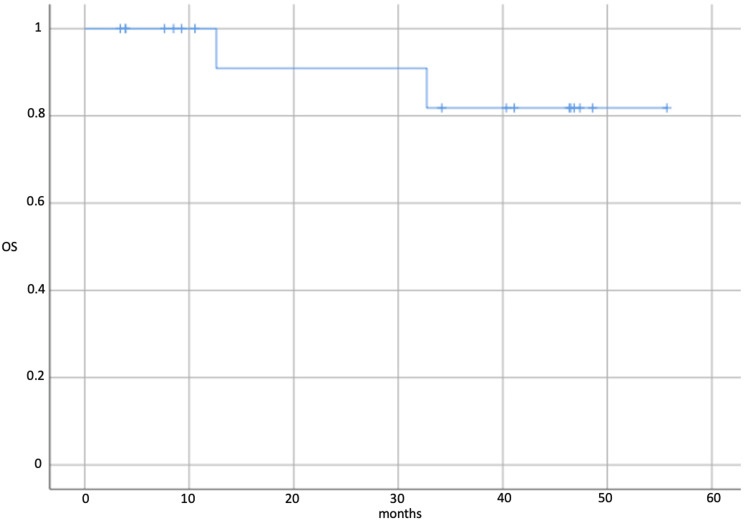 Figure 3
Figure 3| Data | N (%) |
| Sex | |
| Male | 11 (61.1%) |
| Female | 7 (38.9%) |
| Age, median | 65 (56-81) |
| Diagnosis | |
| GEJ | 3 (16.7%) |
| GC, body | 8 (44.4%) |
| Distal GC | 7 (38.9%) |
| Stage | |
| IIA | 2 (11.1%) |
| IIB | 13 (72%) |
| IIIA | 3 (16.7%) |
| T clinical | |
| Т2 | 1 (5.6%) |
| Т3 | 14 (77.8%) |
| Т4а | 2 (11.1%) |
| Т4b | 1 (5.6%) |
| N clinical | |
| N0 | 3 (16.7%) |
| N1 | 15 (83.3%) |
| Regimen (N=18) | N (%) |
| Nivolumab | 11 (61.1%) |
| Pembrolizumab | 6 (33.3%) |
| Nivolumab/Pembrolizumab | 1 (5.6%) |
| Number of cycles before surgery (N=14) | N (%) |
| 4 | 6 (42.9%) |
| 6 | 5 (35.7%) |
| 7 | 1 (7.1%) |
| 8 | 2 (14.3%) |
| Regimen (N=14) | N (%) |
| XELOX | 5 (35.7%) |
| FLOT | 1 (7.1%) |
| FOLFOX | 1 (7.1%) |
| Nivolumab | 1 (7.1%) |
| Objective response (N=18) | N (%) |
| PET-CT scan | |
| CR | 5 (27.8%) |
| PR | 9 (50%) |
| SD | 3 (16.7%) |
| PD | 1 (5.6%) |
| Esophagogastroscopy | |
| CR | 7 (38.9%) |
| PR | 5 (27.8%) |
| SD | 2 (11.1%) |
| PD | 0 |
| ND | 4 (22.2%) |
| Grade (N=14) | N (%) |
| Ryan degree | |
| TRG0 | 6 (42.9%) |
| TRG1 | 2 (14.3%) |
| TRG2 | 5 (35.7%) |
| TRG3 | 1 (7.1%) |
| ypTNM | |
| ypT0N0 | 6 (42.9%) |
| ypT1aN0 | 2 (14.3%) |
| ypT1bN0 | 1 (7.1%) |
| ypT2N0 | 1 (7.1%) |
| ypT0N1 | 1 (7.1%) |
| ypT2N1 | 1 (7.1%) |
| ypT4bN1 | 1 (7.1%) |
| ypT4bN3 | 1 (7.1%) |
| № | Age, y | cTNM | Neoadjuvant phase | PET-CT | EGDs | ypTNM | TRG | Adjuvant phase | Censor | Follow-up, months |
| 1 | 63 | cT3N1 | Nivolumab 6 cycles | PR | CR | ypT0N0 | TRG0 | Nivolumab 3 cycles | No | 55.7 |
| 2 | 72 | cT3N1 | Nivolumab 8 cycles | CR | CR | ypT0N1 | TRG1 | - | Comorb | 32.7 |
| 3 | 64 | cT3N1 | Nivolumab 4 cycles | PR | PR | ypT0N0 | TRG0 | XELOX 2 cycles | No | 46.5 |
| 4 | 71 | cT3N1 | Pembrolizumab 4 cycles | PR | PR | ypT1bN0 | TRG2 | XELOX 4 cycles | No | 46.4 |
| 5 | 65 | cT4aN1 | Pembrolizumab 4 cycles | CR | PR | ypT1aN0 | TRG2 | XELOX 2 cycles | No | 47.4 |
| 6 | 59 | cT3N1 | Pembrolizumab 4 cycles | PR | ND | ypT1aN0 | TRG1 | FLOT 1 cycle | No | 40.4 |
| 7 | 73 | cT3N0 | Pembrolizumab 4 cycles | PR | PR | ypT0N0 | TRG0 | XELOX 1 cycle | No | 46.8 |
| 8 | 68 | cT4aN1 | Pembrolizumab 4 cycles | SD | CR | ypT0N0 | TRG0 | XELOX 2 cycles | No | 41.1 |
| 9 | 57 | cT3N0 | Nivolumab 8 cycles | PD | PR | ypT2N1 | TRG2 | FOLFOX 1 cycle | COVID | 12.6 |
| 10 | 67 | cT3N1 | Pembrolizumab 6 cycles | PR | ND | ypT4bN1 | TRG2 | - | No | 10.5 |
| 11 | 56 | cT3N1 | Nivolumab 3 cycles, Pembrolizumab 3 cycles | CR | CR | ypT0N0 | TRG0 | - | No | 9.2 |
| 12 | 65 | cT3N1 | Nivolumab 7 cycles | SD | SD | ypT4bN3 | TRG3 | - | No | 4.9 |
| 13 | 68 | cT4bN0 | Nivolumab 6 cycles | PR | CR | ypT0N0 | TRG0 | - | No | 4.3 |
| 14 | 57 | cT3N1 | Nivolumab 6 cycles | PR | PR | ypT2N0 | TRG2 | - | No | 4.9 |
| 15 | 56 | cT3N1 | Nivolumab 30 cycles | CR | CR | - | - | - | No | 49.6 |
| 16 | 57 | cT3N1 | Nivolumab 37 cycles | CR | CR | - | - | - | No | 34.6 |
| 17 | 73 | cT3N1 | Nivolumab 13 cycles | PR | ND | - | - | - | No | 8.0 |
| 18 | 81 | cT2N1 | Nivolumab 9 cycles | SD | ND | - | - | - | No | 9.3 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Gastrointestinal Tumor Research and Treatment · Colorectal and Anal Carcinomas
Introduction
Currently, gastric cancer ranks among the leading morbidity and mortality causes worldwide [1]. Unfortunately, 5-year survival in patients after surgical treatment does not exceed 20-30%, with a recurrence risk reaching 80% [2]. In this regard, the standard treatment strategy for locally advanced gastric cancer involves the usage of perioperative chemotherapy with surgery, which can achieve a 5-year survival rate of 45% [3]. On the other hand, molecular and biological subtypes of stomach cancer are actively researched with the aim of personalized selection of various treatment options. The Cancer Genome Atlas (TCGA) classified gastric cancer into four groups: EBV (Epstein-Barr virus) - 9%, MSI (microsatellite instability) - 21%, CIN (chromosomal instability) - 20%, and GS (genomically stable) - 50% [3]. One of the subtypes is characterized by defects in the mismatch repair genes (Microsatellite Instability-High (MSI-H)). According to literature data, its frequency ranges from 1% to 32% depending on various factors such as geographic region, localization of the primary tumor, histological subtype, age, and gender of the patients [4]. Overall, this subtype is characterized by a favorable prognosis, low risk of disease recurrence, and early-stage diagnosis [5]. However, this tumor subtype has low sensitivity to cytostatic drugs, which necessitates the search for pathogenetic treatment strategies [6]. One of these strategies is the usage of checkpoint inhibitors due to the higher tumor immunogenicity [7]. To date, checkpoint inhibitors demonstrate high efficacy in various solid tumors. In the case of MSI-H metastatic tumors, the objective response rate reaches more than 50% [3]. The combination of checkpoint inhibitors (CPI) with chemotherapy is included in the standards of care for patients with metastatic gastric cancer, leading to increased frequency of objective response and progression-free survival (with Combined Positive Score (CPS)≥ 5) [5]. Undoubtedly, their effectiveness in the neoadjuvant setting in patients with locally advanced disease is of interest, given the presence of a predictive biomarker, potential achievement of complete pathomorphological response, low clinical significant toxicity, and impact on overall survival. The aim of this study is to investigate the effectiveness of neoadjuvant monotherapy in patients with locally advanced MSI-H gastric cancer.
Materials and methods
A retrospective analysis of the medical records from the information system of Napalkov State Budgetary Healthcare Institution, Saint Petersburg Clinical, Scientific, and Practical Center for Specialised Types of Medical Care (Oncological) was conducted from June 2019 to December 2023 (4.5 years). Eligible criteria for patients in the study were locally advanced (stage II-III) gastric cancer or gastroesophageal junction cancer (GC/GEJ) and evidence of defects in the mismatch repair genes (microsatellite instability-high (MSI-H)) detected by immunohistochemistry or molecular-genetic methods. All patients provided voluntary informed consent before the study began. Statistical analysis was performed using SPSS Statistics (IBM Corp., Armonk, USA).
A total of 566 patients who underwent testing for defects in the mismatch repair genes were analyzed. Among them, 103 (18.2%) were diagnosed with locally advanced disease. MSI-H was detected in 43 (7.6%) patients. Among them, 18 (41.8%) had locally advanced disease and were included in the study (Figure 1).
Flow-chart of the patients in the studyGC/GEJ - gastric cancer/gastroesophageal junction cancer; locally adv - locally advanced; MSI-H - microsatellite instability-high; pts - patients.*
All patients underwent the esophagogastroscopy with biopsy, CT, or PET-CT scan - five (27.8%) and 13 (72.2%) patients, respectively, and diagnostic laparoscopy and peritoneal lavage with cytological examination (12 out of 18 patients) before the treatment onset.
After preoperative therapy, follow-up examinations (CT or PET-CT scan, esophagogastroscopy, and repeated biopsy) were performed. The next step was surgical treatment. At the time of analysis, 14 out of 18 patients (77.8%) had undergone surgery, while four patients (22.2%) refused. The post-surgery therapeutic pathomorphosis degree was evaluated by the Ryan scale.
Subsequently, all patients were scheduled for follow-up with examinations every 3 months.
Results
Characteristics of patients included in the study are presented in Table 1. In nine (50%) of the patients, MSI-H was determined by immunohistochemistry, while in the remaining cases, the polymerase chain reaction (PCR) method was used.
As a preoperative treatment, all patients received immunotherapy. The treatment regimens are presented in Table 2.
Adjuvant treatment was prescribed in the postoperative period. The treatment regimens are presented in Table 3.
The effectiveness of preoperative immunotherapy is presented in Table 4.
During the preoperative immunotherapy in patients with MSI-H locally advanced gastric cancer, an objective response was achieved in 14 pts (77.8%). Stable of the disease was observed in three patients and disease progression was noted in one patient. It is noteworthy that no correlation was found between the results of radiological and endoscopic examinations. In one patient, there was an increase in metabolic activity in the primary tumor observed on PET-CT. However, clinically and based on endoscopic data, positive dynamics were noted, including regression of the pain in the epigastric area and reduction in the size of the primary tumor, respectively.
Out of 18 patients, 14 (77.8%) underwent surgery. All operated patients achieved R0 resection. Assessment of the tumor pathomorphological response was performed using the Ryan scale. As a result of the preoperative immunotherapy, a complete pathological response (pCR) was observed in six patients (42.9%). A near-complete pathological response was detected in two (14.3%) patients The degree of therapeutic pathomorphosis is presented in Table 5. The pathomorphological stage changed in all patients receiving preoperative immunotherapy. Primary tumor size reduction was observed in 12 patients (85.7%). In two cases (14.3%), the size of the primary tumor increased and corresponded to ypT4b. In another case, an increase in the size of the lesion on PET-CT scan was accompanied by a change in the disease stage from cT3N0 to ypT2N1. It is important to note that regional lymph node involvement persisted in four (28.5%) patients. Thus, we did not observe a correlation between the metabolic and pathomorphological response of the tumor to treatment.
The overall characteristics of the patients are presented in Table 6.
Nowadays, the median follow-up in the study is 33.7 months (ranging from 4.4 to 55.7 months). Disease progression was not registered (Figure 2). Two patients died as a result of concomitant cardiac pathology and the novel coronavirus disease infection (COVID-19). The median overall survival has not been reached (Figure 3). The 3-year overall survival rate was 88.9%.
Duration of response in patients during preoperative immunotherapy.pts - patients
Kaplan-Meier plot of overall survival in patients during the preoperative immunotherapy.OS - overall survival
Special interest is represented by four (22.2%) patients who did not undergo surgical treatment. Two achieved complete and one achieved partial metabolic response, and one achieved stable disease according to PET-CT data. Among the two patients who showed complete response on PET-CT scan, one had no tumor detected on esophagogastroduodenoscopy, and the other had no tumor cells detected on repeat biopsy at the site of the primary tumor. Immunotherapy was discontinued after 30 infusions in one of them due to achieving maximum effect. He continues to be monitored without signs of disease progression for 11 months to date. The others continue therapy (Figure 2).
Despite long-term use of the immunotherapy, no clinically significant immune-mediated toxicity was detected. One patient reported autoimmune hyperthyroidism with grade 2.
Discussion
The study's comprehensive analysis underscores the potential of preoperative immunotherapy in patients with locally advanced gastric cancer characterized by MSI-H [3]. The observed outcomes, including significant objective response rates and disease stabilization, suggest a promising avenue for further exploration and clinical application of immunotherapy in this setting. These findings emphasize the importance of continued research efforts to elucidate the role of immunotherapy in the management of gastric cancer, highlighting the need for tailored treatment approaches and ongoing monitoring to optimize patient outcomes [4-6].
MSI-H gastric and gastroesophageal junction tumors represent a distinct type of disease characterized by high mutational burden and severe immune infiltration [5]. These data provide a basis for research immunotherapy in patients with advanced, chemotherapy-refractory tumors. To date, a high frequency of objective responses (up to 57%) and prolonged survival are demonstrated when checkpoint inhibitors are prescribed in this population [8].
As for locally advanced gastric cancer, the standard approach is perioperative chemotherapy followed by surgical treatment [9, 10, 11]. However, the appropriateness of this strategy in MSI-H patients is not always justified. This is explained by the fact that this type of tumor has a better prognosis [9], but a lower frequency of Pathologic complete response(pCR), as demonstrated with ECF chemotherapy (epirubicin, cisplatin, 5-fluorouracil) [10]. Meanwhile, perioperative chemotherapy with the FLOT regimen (oxaliplatin, paclitaxel, 5-fluorouracil) resulted in a 16% pCR in the overall population [11] and 42% in the MSI-H population [12]. However, treatment regimens involving cytostatics are highly toxic, necessitating the development of new precision therapy methods for this patient’s subgroup [12].
Neoadjuvant immunotherapy has demonstrated high efficacy in skin melanoma and lung cancer treatment. Currently, its effectiveness is known in MSI-H locally advanced rectal and colon cancer [13, 14]. The rationale for early prescription of checkpoint inhibitors in resectable disease is the increased number of neoantigens and tumor-infiltrating lymphocytes, as well as the potential for memory cell formation, which theoretically can prevent disease recurrence [4, 5]. Therefore, examination of neoadjuvant immunotherapy in patients with locally advanced MSI-H gastric cancer is of significant interest [8].
According to the literature, in the past 5 years, 13 studies including checkpoint inhibitors in neoadjuvant therapy regimens for gastric cancer have been published [12]. However, only four of them conducted subgroup analysis in the MSI-H population, and two of them investigated monotherapy [15-18].
In our analysis, a group of patients with locally advanced gastric cancer and MSI-H were treated with neoadjuvant monoimmunotherapy. The median follow-up for this population was 33.7 months, which is the longest reported in the literature.
In the phase II GERCOR NEONIPIGA study, 27 patients received neoadjuvant immunotherapy with ipilimumab+nivolumab, the median follow-up was 14.9 months. In this study, a pCR was observed in 58.6% of patients, while the frequency of grade 3-4 adverse events was 19%, likely due to the combination of checkpoint inhibitors [15]. In our analysis, with monotherapy, a pCR was achieved in 42.9% of patients, and no grade 3-4 adverse events were reported.
Although complete pathologic response is a surrogate marker for survival in locally advanced disease, our study did not find its correlation [15]. None of the patients, regardless of postoperative Pathologic Tumor-Node-Metastasis (ypTNM) stage or Tumor Regression Grade (TRG)pathologic response according to Ryan's classification, showed disease progression during the long follow-up period (over 3 years).
Currently, most published clinical studies on gastric cancer analyze the effectiveness of combination therapy in the neoadjuvant regimen, which includes chemotherapy and checkpoint inhibitors [2, 8, 12, 18]. It is expected that such a combination will increase the frequency of complete pathologic tumor response and impact patient survival. However, the 10% difference in achieving pCR, the lack of influence on disease-free survival, and the increase in clinically significant toxicity raise doubts about the choice of this approach in treating patients with locally advanced MSI-H gastric cancer [12].
Further research is needed to determine the optimal assessment of the tumor response to immunotherapy [17]. Contrast-enhanced computed tomography does not always accurately characterize the dynamics of lesions in hollow organs during treatment [16, 17]. PET-CT allows the evaluation of tumor metabolism in addition to size [17]. However, our study showed that PET-CT results sometimes do not correspond to the endoscopic findings and do not predict pathologic response. According to the literature, the concordance between instrumental and pathologic response is only 49%.
Additionally, our study did not determine the optimal number of immunotherapy cycles before surgery. Some ongoing studies propose a short course of immunotherapy, such as two cycles, as seen in the GERCOR NEONIPIGA study, or prolonged treatment for 6 months [15]. We prescribed four to eight cycles of immunotherapy before surgery, which is standard practice for perioperative chemotherapy, but did not observe differences in treatment outcomes.
Of particular interest in our study are the patients who did not undergo surgical treatment. Currently, there are already known groups of patients with MSI-H rectal cancer for whom a watch-and-wait approach is applied [14, 16, 17]. In our analysis, we presented a similar approach for patients with gastric tumors for the first time. The median follow-up in this group of patients (n=4) was 22.0 months, and most importantly, no disease progression was observed during this time. The optimal strategy for managing patients with potentially resectable tumors requires further investigation in terms of survival duration and the search for surrogate markers of complete pathologic tumor regression [18].
Limitations of this study include its retrospective nature, the use of different immunotherapeutic agents, varying numbers of treatment cycles, and the prescription of chemotherapy to some patients after surgery. Nevertheless, our analysis reflects real-world clinical practice and demonstrates the high efficacy of monoimmunotherapy in patients with locally advanced MSI-H gastric cancer. The following unanswered questions remain - the number of neoadjuvant cycles, the need for adjuvant therapy considering the effect of neoadjuvant immunotherapy, and the duration of immunotherapy in cases of complete regression (including pathologic regression) when patients refuse surgery.
Conclusions
The study's comprehensive analysis underscores the potential of preoperative immunotherapy in patients with locally advanced gastric cancer characterized by MSI-H status. The observed outcomes, including significant objective response rates and long disease stabilization, suggest a promising avenue for further exploration and clinical application of immunotherapy in this setting. These findings emphasize the importance of continued research efforts to elucidate the role of immunotherapy in the management of gastric cancer, highlighting the need for tailored treatment approaches and ongoing monitoring to optimize patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cancer statistics, 2023 CA Cancer J Clin Siegel RL Miller KD Wagle NS Jemal A 17487320233663352510.3322/caac.21763 · doi ↗ · pubmed ↗
- 2Perioperative atezolizumab plus fluorouracil, leucovorin, oxaliplatin, and docetaxel for resectable esophagogastric cancer: interim results from the randomized, multicenter, phase II/III DANTE/IKF-s 633 Trial J Clin Oncol Lorenzen S Götze TO Thuss-Patience P 4104204220243796331710.1200/JCO.23.00975 · doi ↗ · pubmed ↗
- 3Recent advances in the management of gastric adenocarcinoma patients F 1000 Res Harada K Lopez A Shanbhag N Badgwell B Baba H Ajani J 7201810.12688/f 1000 research.15133.1PMC 611786130228868 · doi ↗ · pubmed ↗
- 4Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade Science Le DT Durham JN Smith KN 40941335720172859630810.1126/science.aan 6733 PMC 5576142 · doi ↗ · pubmed ↗
- 5Clinical implications of microsatellite instability in early gastric cancer J Gastric Cancer Kim DG An JY Kim H 4274371920193189734510.5230/jgc.2019.19.e 38PMC 6928080 · doi ↗ · pubmed ↗
- 6Prognostic implication of molecular subtypes and response to neoadjuvant chemotherapy in 760 gastric carcinomas: role of Epstein-Barr virus infection and high- and low-microsatellite instability J Pathol Clin Res Kohlruss M Grosser B Krenauer M 227239520193120624410.1002/cjp 2.137PMC 6817827 · doi ↗ · pubmed ↗
- 7The predictive value of tumor mutation burden on survival of gastric cancer patients treated with immune checkpoint inhibitors: a systematic review and meta-analysis Int Immunopharmacol Ke L Li S Huang D 11098612420233774822310.1016/j.intimp.2023.110986 · doi ↗ · pubmed ↗
- 8Assessment of pembrolizumab therapy for the treatment of microsatellite instability-high gastric or gastroesophageal junction cancer among patients in the KEYNOTE-059, KEYNOTE-061, and KEYNOTE-062 clinical trials JAMA Oncol Chao J Fuchs CS Shitara K 895902720213379264610.1001/jamaoncol.2021.0275 PMC 8017478 · doi ↗ · pubmed ↗