Simultaneous Ablation of Ventricular Tachycardia and Hemodynamic Improvement of Mid-ventricular Obstructive Hypertrophic Cardiomyopathy by Coronary Venous Ethanol Ablation
Serkan Topaloglu, Veysel Kutay Vurgun, Ahmet Korkmaz, Meryem Kara, Elif Hande Ozcan Cetin, Duygu Kocyigit Burunkaya, Firat Ozcan, Serkan Cay, Ozcan Ozeke, Sedat Kose, Miguel Valderrábano

TL;DR
A new technique uses coronary venous ethanol ablation to treat both ventricular tachycardia and improve heart function in hypertrophic cardiomyopathy.
Contribution
The paper introduces a novel application of ethanol ablation for simultaneous arrhythmia treatment and hemodynamic improvement.
Findings
Ethanol ablation can treat ventricular arrhythmias in hypertrophic cardiomyopathy.
Venous ethanol administration may improve left ventricular obstructive physiology.
This technique offers potential dual therapeutic benefits in a single procedure.
Abstract
Transvenous coronary ethanol ablation may be successfully applied to simultaneously treat ventricular arrhythmia superimposed within a segment of hypertrophic cardiomyopathy. This presentation nicely describes this emerging technique for ventricular tachycardia ablation and identifies potential additional benefits of venous ethanol administration in patients with left ventricular obstructive physiology.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1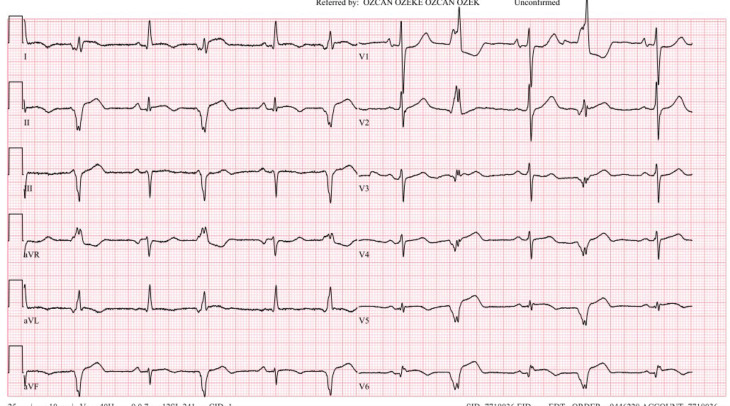 Figure 2
Figure 2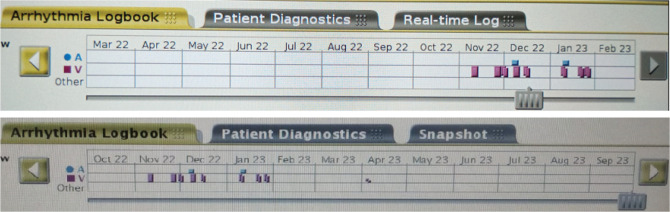 Figure 3
Figure 3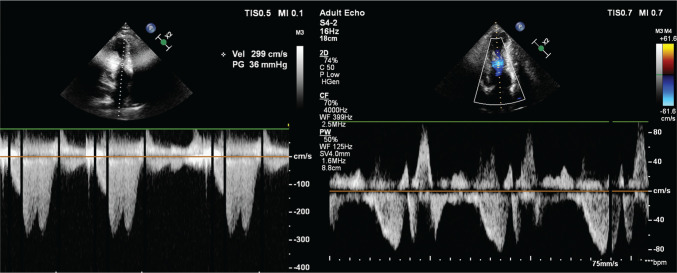 Figure 4
Figure 4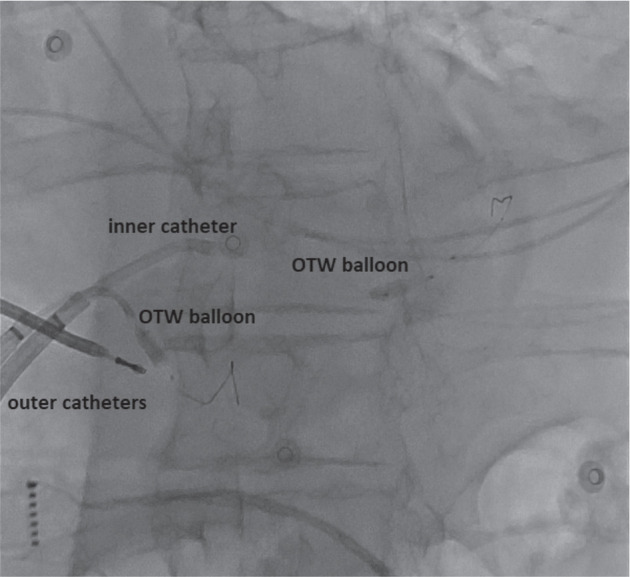 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiomyopathy and Myosin Studies · Cardiac Arrhythmias and Treatments · Cardiovascular Effects of Exercise
Case presentation
A 51-year-old man with hypertrophic cardiomyopathy (HCM), mid-ventricular obstruction (MVO), and an apical aneurysm was referred to our center for stereotactic body radiation therapy (SBRT) after a protracted history of ventricular tachycardia (VT).
He had a transvenous implantable cardioverter-defibrillator (ICD) implanted in 2019 after syncopal events. Three years after ICD implantation, he was admitted with a refractory electrical storm. After failed oral treatments with propranolol, amiodarone, sotalol, and mexiletine, he underwent an endo-epicardial VT ablation in December 2022 at another tertiary center, in which a tachycardia with a cycle length (CL) of 350 ms was ablated using both bipolar ablation and half-normal saline (HNS) irrigation. However, 1 month later, his VT recurred slowly with a CL of 420 ms and did not respond to oral disopyramide therapy. Then, he was referred for a possible evaluation of SBRT.
His functional capacity was New York Heart Association (NYHA) class III. He had no family history of HCM. Echocardiography revealed HCM with an MVO and an apical aneurysm (Videos 1 and 2). A hemodynamic assessment revealed a significant intraventricular pressure gradient of 35 mmHg. Despite the maximal dose of a β-blocker and amiodarone reloading, VT recurred. We proceeded with a repeat endo-epicardial VT ablation, which showed an apparent mid-lateral left ventricular (LV) focal activation pattern with simultaneous endo-epicardial timing, suggesting a mid-myocardial substrate (Video 3). With two THERMOCOOL SMARTTOUCH™ SF catheters (Biosense Webster, Diamond Bar, CA, USA), we delivered sequential unipolar and bipolar endocardial and epicardial ablation at a power of 35 W, prolonged up to 3 min, using HNS irrigation. Despite this, the following day, VT recurred, both sustained and non-sustained and with the same morphology (Figure 1), and remained nearly incessant for the following 2 weeks.
We then performed a venous ethanol ablation. A deflectable sheath (Agilis; Abbott, Chicago, IL, USA) was engaged in the coronary sinus. Venograms identified a lateral vein in the region of the mapped endo-epicardial exit area (Video 4). The lateral vein was cannulated with a 0.0014″ floppy guidewire (Boston Scientific, Marlborough, MA, USA) and an angioplasty balloon (over-the-wire balloon; Boston Scientific). We first deployed a single-balloon technique in the lateral vein using a peripheral balloon distal to the lateral vein. Then, a smaller balloon (Gateway over-the-wire balloon; Boston Scientific) was placed in the proximal portion of the lateral vein (Figure 2). Before injection of alcohol, the position of the balloon was verified by myocardial contrast echocardiography (Video 5). Each vessel was occluded by injection of 5 mL of absolute alcohol in portions of 1 mL/min, and we applied a total of 45 mL of alcohol for ablation via the posterolateral branch (Videos 6 and 7) and the middle cardiac vein (MCV) targeting the apical aneurysm (Video 8). The patient had slight chest pain during the procedure, and we detected a 1-mm inferolateral ST-segment elevation without coronary artery compromise. Programmed ventricular stimulation after ablation revealed non-inducibility.
The following day, he had bigeminal ventricular extrasystoles, which normalized the subsequent day (Figure 3). The patient was discharged after an uneventful hospital stay of 5 days. Medication with 100 mg of metoprolol was continued at discharge without anti-arrhythmics. At an 11-month follow-up, the patient had no ICD shock or therapy, with only one non-sustained VT episode not requiring ICD therapy (Figure 4). His functional capacity was dramatically improved (NYHA class II). The control echocardiographic examination showed a reduction in the interventricular gradient from 36 to 6 mmHg (Figure 5), without apparent wall motion abnormalities (Video 9).
Discussion
HCM is a common inherited cardiac disease with a prevalence of approximately 0.2%–0.5% in the general population. The majority of HCM patients have a left ventricular outflow tract obstruction (LVOTO) at rest or with provocation.^1^ MVO is a less-common subtype of HCM, but it is associated with ventricular arrhythmia (VA) and a worse prognosis.^2–6^ Septal reduction therapy is recommended in patients with obstructive HCM who remain symptomatic under maximally tolerated optimal medical treatment.^7^ Alcohol septal ablation is a favorable option, especially in LVOTO-type patients with a high surgical risk or who refuse surgery.^8^ The procedure causes a controlled myocardial infarction of the basal portion of the interventricular septum by the injection of absolute alcohol to reduce LVOTO and improve the patient’s hemodynamics and symptoms.
Recently, numerous observations have demonstrated that the MVO type of HCM may also respond favorably to alcohol septal ablation.^9,10^ Fourth septal branch ablation for pressure gradient reduction in patients with the MVO type was reported by Seggewiss and Faber.^9^ In our case, the reduction in the intraventricular gradient was achieved with non-septal alcohol ablation. However, the effect of alcohol ablation of MCV and percutaneous endo-epicardial ablation might also have an impact on this favorable outcome.^11^
Catheter ablation is a useful option for patients with recurrent, drug-refractory, monomorphic VT, as well as device therapy. The success of catheter ablation depends on the ability to reach the anatomic location of the VT substrate. Indications for catheter ablation for VAs in patients with HCM are not clearly defined and need to be tailored for each patient.^12^ Santangeli and colleagues found that epicardial ablation was necessary to treat VT in close to 60% of cases.^13^ Therefore, understanding the location and extent of the substrate can help in guiding the ablation strategy. SBRT, sympathetic denervation, cardiac surgery, bipolar ablation, and alcohol ablation are promising therapies for VT refractory to catheter ablation. As seen in the current case, for some patients with focal ectopies arising from the epicardial or intramural locations, neither endocardial nor epicardial ablation is consistently helpful, as a result of the inadequate power delivery to the mid-myocardial VA origin.^14^ Venous ethanol is emerging as a powerful alternative in cases of unreachable substrate.^15^ Multiballoon, multivein intramural venous alcohol ablation can provide effective substrate ablation in patients with radiofrequency catheter ablation-refractory VT in the setting of structural heart disease over a broad range of LV locations.^16^ Despite a long duration, HNS, and bipolar ablation attempts, the only retrograde alcohol application of the posterolateral branch of the coronary sinus eliminated the patient’s nearly incessant tachycardia in the current case. Coronary arterial alcohol ablation could have achieved a greater reduction in mid-myocardial obstruction in addition to VT elimination; however, it is riskier than ablating the venous system. Therefore, ethanol ablation via the coronary venous anatomy can offer electrophysiologists another option in their armamentarium of treatments against VT.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Maron MS Olivotto I Zenovich AG Hypertrophic cardiomyopathy is predominantly a disease of left ventricular outflow tract obstruction Circulation 2006114212232223910.1161/CIRCULATIONAHA.106.64468217088454 · doi ↗ · pubmed ↗
- 2Efthimiadis GK Pagourelias ED Parcharidou D Clinical characteristics and natural history of hypertrophic cardiomyopathy with midventricular obstruction Circ J 20137792366237410.1253/circj.cj-12-156123728066 · doi ↗ · pubmed ↗
- 3Minami Y Kajimoto K Terajima Y Clinical implications of midventricular obstruction in patients with hypertrophic cardiomyopathy J Am Coll Cardiol 201157232346235510.1016/j.jacc.2011.02.03321636036 · doi ↗ · pubmed ↗
- 4Cui L Tse G Zhao Z Mid-ventricular obstructive hypertrophic cardiomyopathy with apical aneurysm: an important subtype of arrhythmogenic cardiomyopathy Ann Noninvasive Electrocardiol 2019245 e 1263810.1111/anec.1263830737990 PMC 6931486 · doi ↗ · pubmed ↗
- 5Sun D Schaff HV Nishimura RA Geske JB Dearani JA Ommen SR Transapical septal myectomy for hypertrophic cardiomyopathy with midventricular obstruction Ann Thorac Surg 2021111383684410.1016/j.athoracsur.2020.05.18232771468 · doi ↗ · pubmed ↗
- 6Tang Y Song Y Duan F Extended myectomy for hypertrophic obstructive cardiomyopathy patients with midventricular obstruction Eur J Cardiothorac Surg 201854587588310.1093/ejcts/ezy 20329868767 · doi ↗ · pubmed ↗
- 7Gragnano F Pelliccia F Guarnaccia N Working Group of Interventional Cardiology of the Italian Society of Cardiology. Alcohol septal ablation in patients with hypertrophic obstructive cardiomyopathy: a contemporary perspective J Clin Med 2023128281010.3390/jcm 1208281037109147 PMC 10142866 · doi ↗ · pubmed ↗
- 8Ates AH Sener YZ Sahiner ML Kaya EB Aytemir K Single center experience of percutaneous septal ablation in patients with hypertrophic cardiomyopathy with a novel agent: polidocanol Am J Cardiol 20231901710.1016/j.amjcard.2022.11.02236535228 · doi ↗ · pubmed ↗