Uncovering the Invisible: The Role of High-density Catheters in Recognizing Fractionated Signals in Pulmonary Vein Isolation
Harini Lakshman, Ammar Ahmed, Steven Coutteau, Dipak Shah

TL;DR
High-density catheters help detect hidden signals in heart procedures, improving success rates for treating atrial fibrillation.
Contribution
The HD Grid catheter reveals fractionated signals missed by conventional tools, enhancing pulmonary vein isolation effectiveness.
Findings
Fractionated signals at the LAA–LSPV junction are detectable only with high-density catheters.
HD Grid catheter improves identification of ablation gaps and low-voltage isthmus.
Ablation success depends on catheter stability, signal quality, and ridge thickness.
Abstract
The HD Grid multipolar mapping catheter has emerged as an invaluable tool for greater effectiveness of pulmonary vein isolation (PVI). In the cases described here, fractionated signals seen with the HD Grid catheter at the left atrial appendage (LAA) and left superior pulmonary vein (LSPV) junction were ablated. These signals are not likely to be visualized with conventional catheters and may cause recurrences due to incomplete PVI. The directional sensitivity limitations of bipolar electrogram recordings and the unique anatomy of the LAA–LSPV ridge further contribute to the challenge of evaluating PVI. The HD Grid catheter’s ability to record bipoles parallel and perpendicular to the catheter splines and its high-density mapping capabilities provide a superior means for identifying gaps in ablation and detecting the low-voltage isthmus. Furthermore, factors such as ablation quality,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
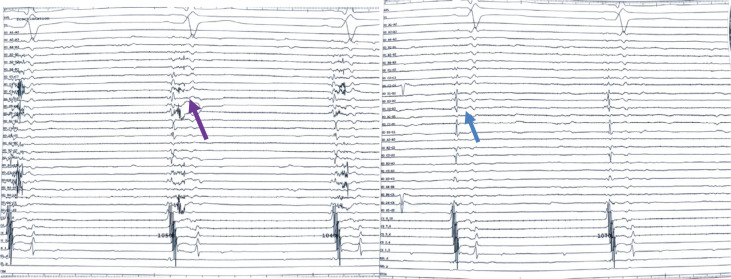 Figure 1
Figure 1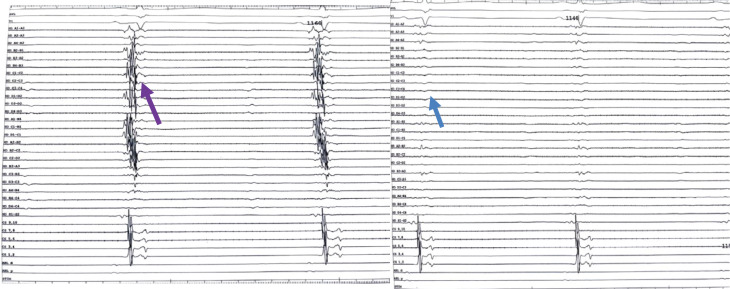 Figure 2
Figure 2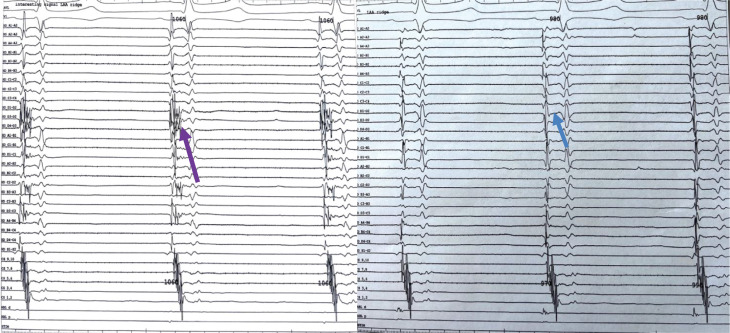 Figure 3
Figure 3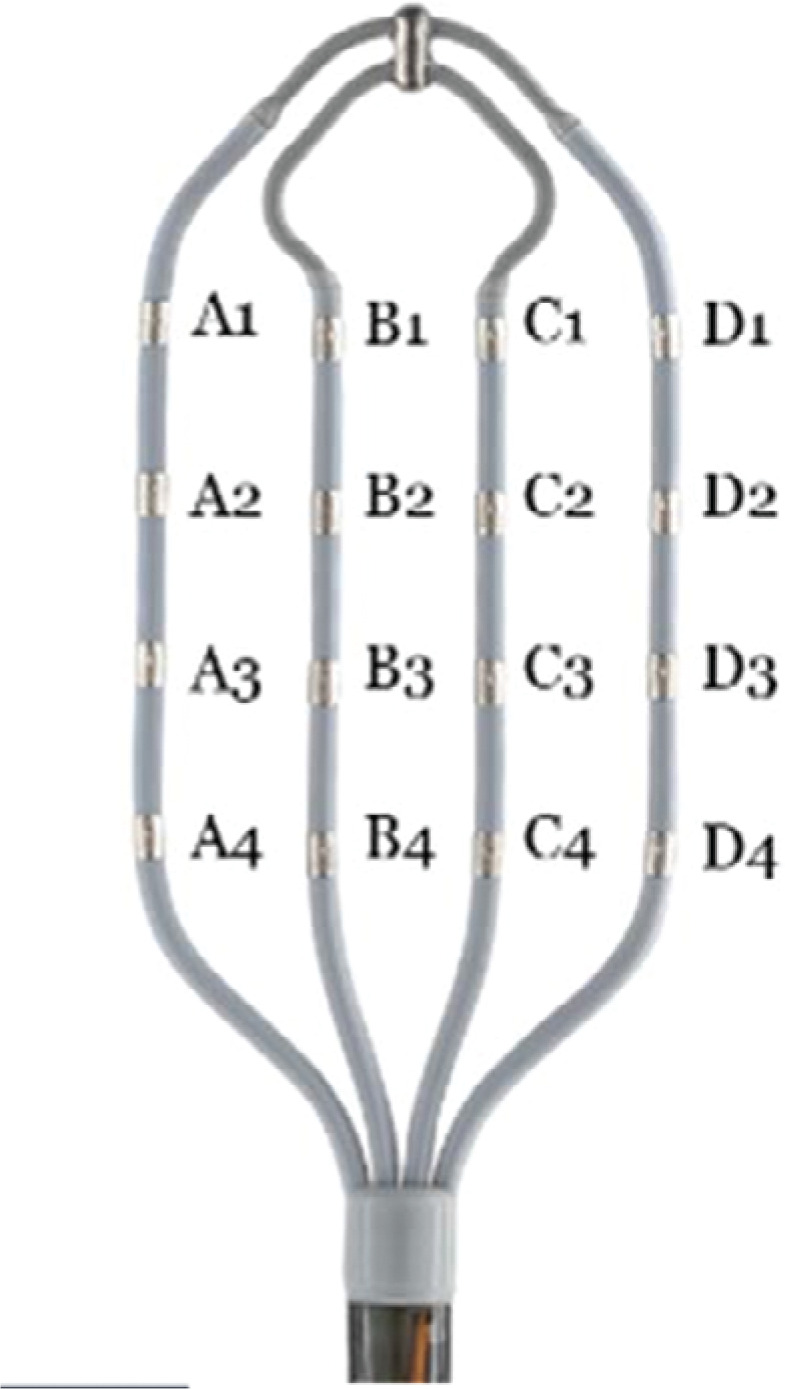 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Arrhythmias and Treatments · Atrial Fibrillation Management and Outcomes · Cardiac electrophysiology and arrhythmias
Introduction
Atrial fibrillation (AF) ablation has significant recurrence rates, which vary from 35%–60% in the literature.^1^ In 98% of patients with recurrence, pulmonary vein (PV) reconnection is the likely mechanism.^2^ The entrance block is the most common endpoint signifying PV isolation (PVI), and circular mapping catheters are often used to confirm this. With the advent of higher-fidelity catheters, such as the high-density grid (HD Grid) catheter, the entrance block previously seen with circular catheters is often not present.^3^
We present a case series of fractionated signals at the ridge between the left superior pulmonary vein (LSPV) and the left atrial appendage (LAA), which were detected by the HD Grid catheter, which would likely be overlooked by circular mapping catheters, leading to recurrence of AF.
Case presentations
As seen in Figures 1–3, each of the included cases underwent paroxysmal AF ablation with PVI after ensuring contact forces of >8 g. The baseline characteristics are provided in Table 1.
After ensuring that all the PVs were isolated, by demonstrating an entrance block, the Advisor™ HD Grid Mapping Catheter, Sensor Enabled™ (Abbott, Chicago, IL, USA) was used to map and confirm the exit block. There was the presence of fractionated signals between the LSPV and LAA in each of these cases, which would not be uncovered if using a conventional circular mapping catheter.
Ethical approval was not required given the retrospective nature of the essential procedures.
Discussion
In the series of cases described (Figures 1–3), fractionated signals seen with the HD Grid catheter at the LAA and LSPV junction were ablated. These signals would not likely have been visualized with conventional catheters and may cause recurrences due to incomplete PVI.
The directional sensitivity of bipolar electrogram recordings is a limitation. When the wavefront is propagating parallel to the electrode pair, higher amplitudes are recorded than when it moves perpendicularly.^1^ Considering that previous research demonstrated that myocardial fibers infiltrate the PVs longitudinally, circumferentially, and obliquely, this limitation of typical bipoles may be crucial for evaluating PVI.^4^
In contrast to conventional multipolar mapping catheters and ablation catheters, which only permit bipole recording parallel to the splines, the HD Grid multipolar mapping catheter is a novel and one-of-a-kind multipolar mapping catheter that permits bipole recording parallel and perpendicular to the splines via 16 electrodes (Figure 4).^4^
Studies comparing the HD Grid catheter with circular mapping catheters, cryoablation catheters, and pacing the ablation line found the HD Grid catheter to be superior in identifying the gaps in ablation.^4–7^ Approximately 52.5% of patients with recurrent AF had gaps in ablation detected by HD Grid compared to traditional catheters. The HD Grid offers the capability to perform high-density mapping to identify the anatomical substrate and low-voltage isthmus, which previously would have been missed.^8^
Other factors that could have resulted in these fractionated signals include the quality of ablation.
In our case series, at these locations, we had contact forces of >8 g and ablated with high-power, short-duration radiofrequency ablation (RFA) of 45 W for 10–25 s, targeting a lesion size index (LSI) of 6. Despite these standard RFA parameters, these signals were still present.^9^
The potential reasons why these signals were realized in our cases is that the HD Grid allows for excellent anterior flexion around the LAA and LSPV interface, which maximizes tissue contact. If flexion is not applied along the ridge, these signals will not likely be visualized. Future developments in the HD Grid technology potentially involving a contact force measure during mapping may allow operators to appreciate this more clearly.
The PV and LA junction is a complex interface surrounded by a wide range of heterogeneous tissue types.^1^ The location of the LAA in relationship to the LSPV as well as the thickness of the LAA–LSPV ridge make this area of ablation unique for each patient. Often, catheter stability in this region limits how antrally one can deliver RF. If the ablation is too ostial, these antral signals will be missed.
No preprocedural imaging was done in our cases. Possibly, computed tomography or magnetic resonance imaging could quantify the thickness of this region, and then a more tailored approach could be taken. Also, intracardiac echocardiography could potentially be used in real time to delineate the LAA–LSPV ridge. Depending on the anatomic issues visualized, possible options include a longer duration of RFA targeting a higher force–time integral or LSI, allowing for a transmural lesion or RFA on both the PV and LAA side of the ridge as a sandwich technique.
Our case series demonstrates a detailed interrogation of the LAA–LSPV ridge with the HD Grid as a culprit for incomplete PVI.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Szegedi N Simon J Szilveszter B Abutting left atrial appendage and left superior pulmonary vein predicts recurrence of atrial fibrillation after point-by-point pulmonary vein isolation Front Cardiovasc Med 2022970829810.3389/fcvm.2022.70829835242821 PMC 8885731 · doi ↗ · pubmed ↗
- 2Porterfield C Gora PJ Wystrach A Confirmation of pulmonary vein isolation with high-density mapping: comparison to traditional workflows J Atr Fibrillation 2020126236110.4022/jafib.236133024494 PMC 7533127 · doi ↗ · pubmed ↗
- 3Crandall B Kanuri S Cutler M High power ultra short duration ablation with HD grid improves freedom from atrial fibrillation and redo procedures compared to circular mapping catheter J Atr Fibrillation 2020132241410.4022/jafib.241434950298 PMC 8691311 · doi ↗ · pubmed ↗
- 4Takigawa M Relan J Kitamura T Impact of spacing and orientation on the scar threshold with a high-density grid catheter Circ Arrhythm Electrophysiol 2019129 e 00715810.1161/CIRCEP.119.00715831446771 · doi ↗ · pubmed ↗
- 5Okubo K Frontera A Bisceglia C Grid mapping catheter for ventricular tachycardia ablation Circ Arrhythm Electrophysiol 2019129 e 00750010.1161/CIRCEP.119.00750031500436 · doi ↗ · pubmed ↗
- 6Takigawa M Relan J Martin R Effect of bipolar electrode orientation on local electrogram properties Heart Rhythm 201815121853186110.1016/j.hrthm.2018.07.02030026016 · doi ↗ · pubmed ↗
- 7Fiedler L Roca I Lorgat F Characterization of high-density mapping in catheter ablation for persistent atrial fibrillation: results from the Advisor™ HD Grid Mapping Catheter Observational study J Interv Card Electrophysiol 20226661411142110.1007/s 10840-022-01442-336481832 PMC 9735148 · doi ↗ · pubmed ↗
- 8Papageorgiou N Karim N Williams J Initial experience of the High-Density Grid catheter in patients undergoing catheter ablation for atrial fibrillation J Interv Card Electrophysiol 202263225926610.1007/s 10840-021-00950-y 33638777 · doi ↗ · pubmed ↗