Case report of increased left ventricular end-diastolic pressure with pulsatile left ventricular assist device
Mauricio Felippi de Sá Marchi, Sarah Verhemel, Rutger-Jan Nuis, Nicolas M Van Mieghem

TL;DR
A patient on a pulsatile LVAD experienced increased left ventricular pressure during a heart procedure, likely due to aortic valve issues.
Contribution
This case highlights a rare complication where LVAD use may cause aortic regurgitation and elevated LVEDP.
Findings
LVAD use during TAVI and PCI led to unexpected increases in LVEDP and shortness of breath.
LVAD across the aortic valve may immobilize aortic leaflets, causing acute aortic regurgitation.
Symptoms resolved immediately after LVAD removal.
Abstract
Left ventricular assist devices (LVADs) are increasingly utilized in cardiogenic shock and high-risk percutaneous coronary interventions (PCIs). These devices aspirate and expel blood from the left ventricle (LV) into the aorta, consequently reducing left ventricular end-diastolic pressure (LVEDP). We report a case of unexpected LVEDP rise under LV-to-aorta LVAD in the context of transcatheter aortic valve implantation (TAVI) and concomitant multi-vessel PCI. A patient with acute heart failure, severely depressed systolic LV function, severe aortic stenosis, and multi-vessel coronary artery disease underwent TAVI and concomitant PCI under pulsatile LVAD. Notably, the patient experienced unexpected shortness of breath and elevated LVEDP while under LVAD, which normalized immediately upon LVAD removal. Pulsatile LVAD enhances cardiac output by providing pulsatile support through a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1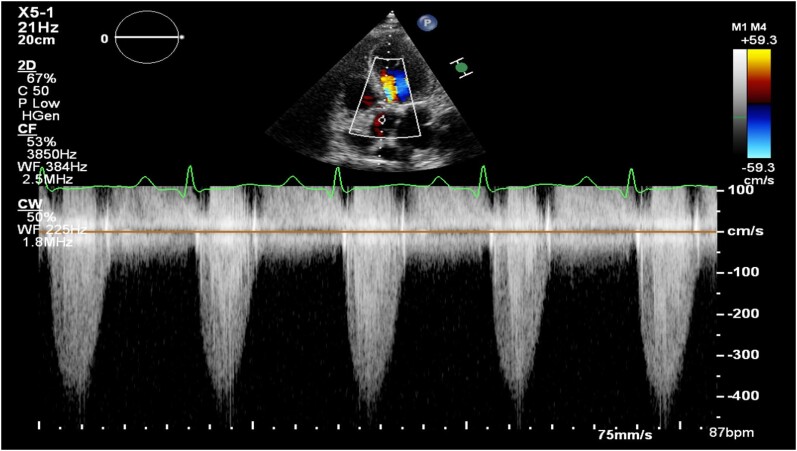 Figure 1
Figure 1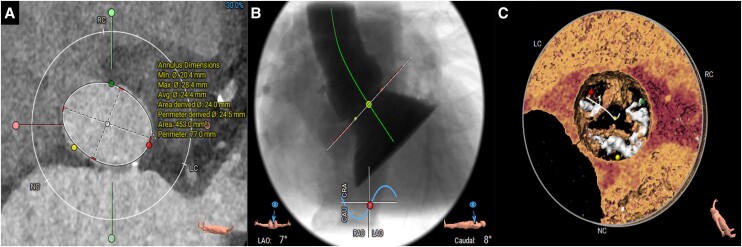 Figure 2
Figure 2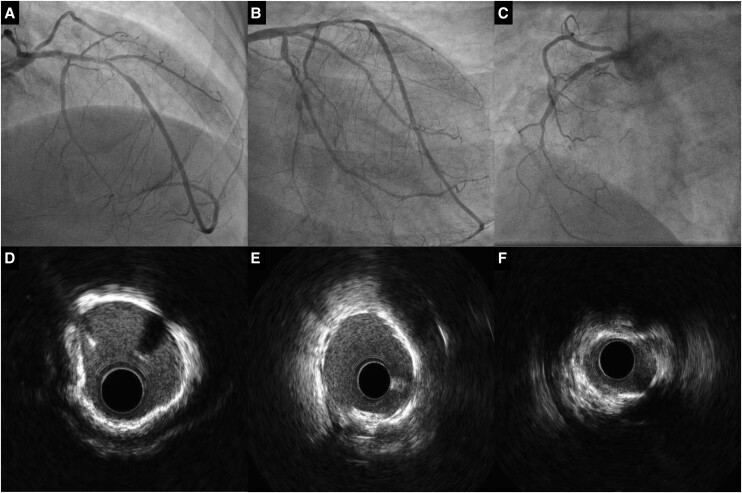 Figure 3
Figure 3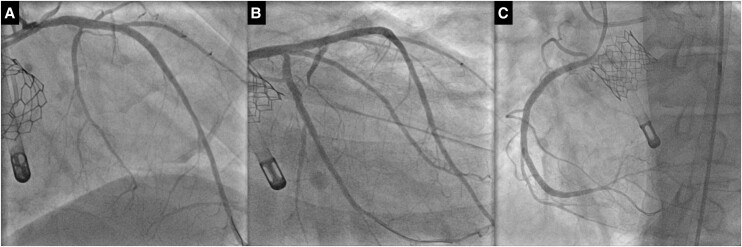 Figure 4
Figure 4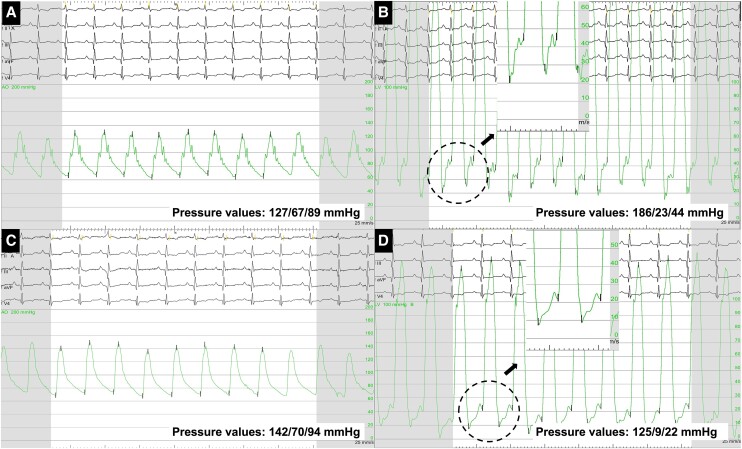 Figure 5
Figure 5- —International Research
- —Conselho Nacional de Desenvolvimento Científico e Tecnológico-Brasil10.13039/501100003593
- —Abbott10.13039/100001316
- —Boston Scientific10.13039/100008497
- —Biotronik10.13039/501100005035
- —Edwards Lifesciences10.13039/100006520
- —Medtronic10.13039/100004374
- —PulseCath BV
- —Abiomed10.13039/100020297
- —Daiichi Sankyo10.13039/501100002973
- —JenaValve10.13039/100019998
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMechanical Circulatory Support Devices · Cardiac pacing and defibrillation studies · Cardiac Structural Anomalies and Repair
Introduction
Percutaneous left ventricular assist devices (LVADs) are occasionally used for mechanical circulatory support during cardiogenic shock or high-risk percutaneous coronary interventions.^1^ Since its conception, LVAD has grown from a rescue strategy for cardiogenic shock patients to a bridging tool in various cardiovascular procedures.^1^ Current AHA/ACC guidelines suggest elective insertion of LVAD to facilitate percutaneous coronary intervention (PCI) in selected high-risk patients (class IIb, level of evidence B).^1,2^
Percutaneous LVADs are introduced across the aortic valve to aspirate and expel blood from the LV into the ascending aorta, which typically unloads the LV and reduces the left ventricular end-diastolic pressure (LVEDP).^1^ In this report, we describe a case in which LVEDP increased during LVAD support and immediately normalized upon device removal.
Summary figure
**
Case presentation
A 57-year-old man with a history of hypercholesterolaemia, type 2 non-insulin dependent diabetes mellitus, and obstructive sleep apnoea was admitted with dyspnoea and peripheral oedema, secondary to decompensated heart failure (NYHA class IV). On physical examination, auscultation revealed a parasternal holosystolic murmur over the right 2nd intercostal space and bilateral pulmonary crepitations. Laboratory tests showed a serum creatinine of 105 mmol/L, GFR 68 mL/min, NT-pro-BNP value of 664 pmol/L, and maximum high-sensitive troponin 345 ng/L. Transthoracic echocardiography (TTE) revealed reduced LVEF (29%) and severe aortic stenosis (AS), with a mean gradient of 36 mmHg, peak velocity of 4.3 m/s, and aortic valve area of 0.49 cm2 (Figure 1). Multi-slice computed tomography exhibited an Agatston score of 3194 AU and an annulus area of 453 mm^2^ (Figure 2). Coronary angiography showed significant left anterior descending artery (LAD) stenosis, intermediate left circumflex artery (LCx) stenosis, and chronic total occlusion of the right coronary artery (RCA) (Figure 3).
Continuous Doppler on native aortic valve. Continuous Doppler shows an aortic valve peak velocity of 4.31 m/s.
Multidetector computed tomography images of the native aortic valve. (A) Measurement of aortic annulus for cross-sectional area and perimeter in end systole. (B) Three-cusp coplanar view. (C) Three-dimensional reconstructions of valve.
Coronary angiographies and intravascular ultrasound (IVUS) evaluation. (A) Cranial angiography showcasing left anterior descending (LAD) severe stenosis in the proximal and medium segment of the vessel. (B) Right caudal angiography showing left circumflex (LCx) severe stenosis in the proximal segment of the vessel. (C) Left oblique angiography displaying diffuse severe right coronary artery (RCA) stenosis. (D) IVUS of the LAD presenting a 360° calcification arch. (E) IVUS of the LCx revealing a 180° calcification arch. (F) IVUS of the RCA showing diffuse calcification and vessel sub-occlusion.
The multidisciplinary heart team deemed the patient at high operative risk because of the decompensated AS, severely depressed LV function, and multi-vessel coronary disease, calculated STS PROM 4.2% and reached consensus for transcatheter aortic valve implantation (TAVI) with concomitant PCI under pulsatile LVAD. This decision was in accordance with the joint Dutch cardiology society (NVVC) and Dutch cardiothoracic surgeons society (NVT) consensus statement for the indication of TAVI in 2020.^3^
The procedure was performed under local anaesthesia and filter based cerebral embolic protection (Sentinel®, Boston Scientific, Marlborough, USA). A 14 F re-collapsible sheath was introduced in the right common femoral artery and a 6 F sheath in the ipsilateral superficial femoral artery. Invasive pressures were measured using a pig-tail catheter positioned at the LV apex and the aorta. Initial LVEDP was 43 mmHg, and the transvalvular mean aortic pressure gradient was 67 mmHg. A 0.035″ pre-shaped stiff wire (Safari®, Boston Scientific, Marlborough, USA) was advanced and positioned in the LV. Aortic valve balloon valvuloplasty with a 22 mm balloon and TAVI with a 26 mm Sapien 3 Ultra® (Edwards Lifesciences, Irvine, USA) was performed under rapid pacing on the 0.035″ pre-shaped stiff wire (Safari®, Boston Scientific, Marlborough, USA) in the LV. The valve was subsequently post-dilated with a 24 mm balloon due to angiographic evidence of aortic regurgitation. After TAVI LVEDP dropped to 24 mmHg and final aortography showed no signs of residual aortic insufficiency.
After TAVI, a 17 F pulsatile LVAD device (iVAC 2L®, PulseCath BV, Amsterdam, The Netherlands) was introduced over the 0.035″ LV wire to provide support for PCI. The patient noticed respiratory discomfort upon iVAC2L insertion. Intravascular ultrasound (IVUS)-guided complete revascularization was performed including calcium modification with a 3.0 mm Shockwave balloon® (Shockwave Medical, Santa Clara, USA) and a 3.5 × 40 mm drug-eluting stent (DES) in the LAD, a 2.5 × 26 mm DES in the LCx, and successful recanalization of the RCA with four (4.0 × 9 mm, 3.5 × 40 mm, 3.5 × 40 mm, and 2.5 × 15 mm) DES (Figure 4). Left ventricular end-diastolic pressure after multi-vessel PCI completion under LVAD support was 44 mmHg. After its removal, LVEDP immediately dropped to 22 mmHg (Figure 5 and Supplementary material online, Video S1). Large bore common femoral arteriotomy closure was successfully achieved with two Perclose ProStyle (Abbott, Abbott Park, USA) devices and one 8 F Angio-Seal (Terumo Interventional Systems, Tokyo, Japan). After confirmation of patent haemostasis by angiography through the SFA sheath, superficial femoral arteriotomy was closed with one perclose prostyle device.
Final coronary angiographies. (A) LAD angiography. (B) LCx angiography. (C) RCA angiography.
Aortic pressure and left ventricular end-diastolic pressure (LVEDP) curves. Aortic pressure (A) and left ventricular end-diastolic pressure (B) curves with iVAC 2L. Aortic pressure (C) and left ventricular end-diastolic pressure (D) curves after the device retrieval.
Pre-discharge TTE displayed an overall good bioprosthetic valve performance, with aortic mean gradient of 14 mmHg, no paravalvular leak, and 35% EF.
Patient experienced a fast recovery after the procedure. The LVEF improved to 35%, the aortic valve area was 1.7 cm2, and the patient was discharged on Day 2 after the procedure.
Discussion
Multiple percutaneous LVADs with variable profile and mode of operations are available.^1^ Patients undergoing complex PCI may be at risk for haemodynamic compromise but,^2^ current evidence does not support the routine utilization of LVAD devices to mitigate cardiovascular events during complex PCI. Clinical judgement is advised on a case-by-case basis (class IIb, level of evidence B).^2^
In our case, the patient was deemed at high surgical risk and also at risk for haemodynamic compromise during PCI because of the decompensated severe AS in combination with low LVEF and multi-vessel complex coronary disease that may require advanced lesion preparation techniques. We opted for a percutaneous approach with TAVI and PCI under LVAD support with the iVAC 2L (PulseCath BV, Amsterdam, The Netherlands), a percutaneous 17 Fr bi-directional flow catheter that generates up to 2.0 L/min of pulsatile support on top of the existing cardiac output.^4^ This catheter is inserted through the common femoral artery and advanced retrogradely across the aortic valve into the LV. The LVAD distal tip should be positioned midway within the left ventricular cavity and the two-way valve containing outlet in the ascending aorta.^5^ After introduction, the catheter is connected to an extracorporeal membrane pump, which is driven by an intra-aortic balloon pump console. Using electrocardiographic triggering, blood is aspirated from the LV through the inlet tip during systole and ejected via the two-way valve into the ascending aorta during diastole.^5^ The resulting pulsatile support generates additional output with systolic unloading of the LV and diastolic counterpulsation.^4,5^ The pivotal valve function at the outflow port is synchronized with aortic valve closure and should not interfere with the aortic valve functioning.^4,5^
Unexpectedly, after TAVI and the introduction of the iVAC2L, the patient experienced immediate respiratory discomfort. After completion of the multi-vessel PCI, the LVEDP remained elevated despite LVAD support. Upon LVAD removal, LVEDP promptly decreased. Our primary hypothesis for this occurrence was the eccentric position of the LVAD across the aortic valve, potentially leading to partial immobilization or restricted mobility of one or more aortic leaflets, resulting in inadequate leaflet coaptation and severe valvular aortic regurgitation. In order to prevent this complication, physicians should be mindful of LVAD malpositioning across the aortic valve and have a low threshold for echocardiography in the context of unexplained haemodynamic compromise under mechanical circulatory support.
Conclusion(s)
Left ventricular assist device can potentially cause malcoaptation of TAVI leaflets, leading to acute aortic regurgitation (AR) due to partial immobilization or restricted mobility of one or more aortic leaflets. This inadequate leaflet coaptation can result in severe valvular AR. Thus, it is essential to ensure precise device placement and promptly detect any aortic leaflet malcoaptation to prevent this rare occurrence.
Supplementary Material
ytae291_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Salter BS , Gross CR, Weiner MM, Dukkipati SR, Serrao GW, Moss N, et al Temporary mechanical circulatory support devices: practical considerations for all stakeholders. Nat Rev Cardiol 2023;20:263–277.36357709 10.1038/s 41569-022-00796-5PMC 9649020 · doi ↗ · pubmed ↗
- 2Lawton JS , Tamis-Holland JE, Bangalore S, Bates ER, Beckie TM, Bischoff JM, et al 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice Guidelines. J Am Coll Cardiol 2022;79:e 21–e 129.34895950 10.1016/j.jacc.2021.09.006 · doi ↗ · pubmed ↗
- 3Nederlandse Vereniging voor Thoraxchirurgie en Nederlandse Vereniging voor Cardiologie. Indicatie richtlijn TAVI. 2020.
- 4Van Mieghem NM , Daemen J, Lenzen MJ, Zandstra R, Malkin O, van Geuns RJ. The Pulse Cath i VAC 2L left ventricular assist device: conversion to a percutaneous transfemoral approach. Euro Intervention 2015;11:835–839.26603991 10.4244/EIJV 11I 7A 168 · doi ↗ · pubmed ↗
- 5den Uil CA , Daemen J, Lenzen MJ, Maugenest A-M, Joziasse L, van Geuns R-JM, et al Pulsatile i VAC 2L circulatory support in high-risk percutaneous coronary intervention. Euro Intervention 2017;12:1689–1696.28216471 10.4244/EIJ-D-16-00371 · doi ↗ · pubmed ↗