Autoimmune Hemolytic Anemia Associated with Mature Ovarian Cystic Teratoma Containing Monoclonal Immunoglobulin G: A Case Report and Review of Literature
Yuma Nato, Keiki Nagaharu, Keika Itoh, Naoki Shinke, Keiko Maeyama, Akihiko Sawaki, Hiroyuki Miyashita

TL;DR
A rare case of autoimmune hemolytic anemia linked to an ovarian tumor was successfully treated, suggesting a possible connection between the tumor and antibody production.
Contribution
This case report provides evidence of monoclonal IgG-κ in a mature cystic teratoma potentially causing secondary AIHA.
Findings
A 22-year-old woman with an ovarian tumor showed signs of autoimmune hemolytic anemia.
Tumor contents contained monoclonal immunoglobulin G-κ, suggesting intratumoral antibody production.
Prednisolone treatment improved the patient's anemia.
Abstract
Autoimmune hemolytic anemia (AIHA) associated with solid tumors such as mature cystic teratomas is rare and poorly understood. Here, we report a successfully treated case of secondary AIHA in a mature cystic teratoma containing antibodies against red blood cells. Case description. A 22-year-old woman was referred to our hospital with progressive anemia. Laboratory findings revealed hemolysis with a positive direct and indirect antiglobulin test. Imaging studies identified a left ovarian mass, suspected to be a mature cystic teratoma, which was later confirmed by histopathology after laparoscopic oophorocystectomy. The patient was treated with prednisolone, resulting in improved anemia. To examine the relationship between the tumor and AIHA, an indirect antiglobulin test was performed on the tumor contents. Stronger aggregations were observed at any concentration diluted by 10 times from…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
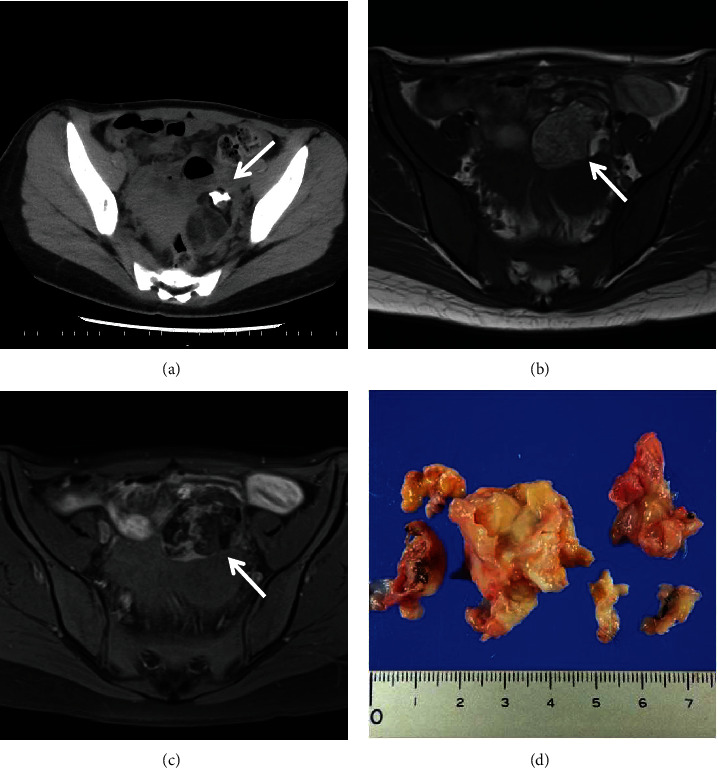 Figure 1
Figure 1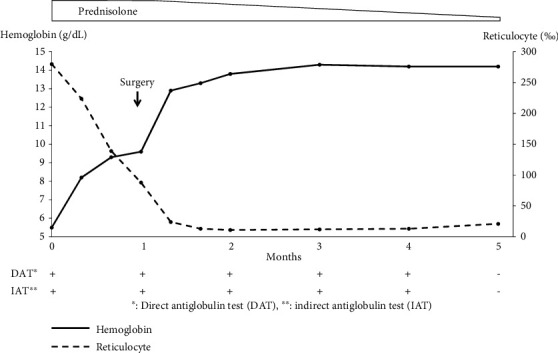 Figure 2
Figure 2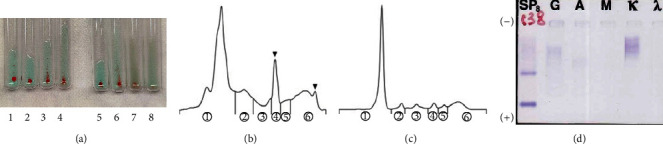 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBlood groups and transfusion · Erythrocyte Function and Pathophysiology · Renal Diseases and Glomerulopathies
1. Introduction
Autoimmune hemolytic anemia (AIHA) is a condition in which the immune system produces antibodies that attack red blood cells, leading to their destruction and a reduced lifespan. AIHA stands out as one of the leading types of acquired hemolytic diseases with an incidence of approximately 1.8 per 100,000 person-years [1], and those are further subdivided into primary and secondary AIHA. Secondary AIHA frequently occurs in association with hematological cancers in 50% of cases, infections in about 33%, and collagen vascular diseases in around 17% [2]. Rare instances have also identified solid cancers, such as mature cystic teratomas, as potential triggers of secondary AIHA. Studies have indicated that secondary AIHA, when linked to mature cystic teratomas, does not typically respond well to treatments like steroids or splenectomy. However, tumor removal often leads to AIHA resolution [2]. The exact pathogenic mechanisms by which tumors induce AIHA as part of a paraneoplastic syndrome remain elusive [3]. This case report discusses the effective treatment of AIHA in a patient with a mature cystic teratoma through prednisolone administration after a laparoscopic oophorocystectomy.
2. Case Presentation
A 22-year-old nulliparous woman was referred to our hospital due to anemia persisting for two weeks. Laboratory tests on admission revealed a hemoglobin level of 5.5 g/dL, a circulating reticulocyte count of 280‰, a lactate dehydrogenase level of 500 IU/L (reference range, 124–224 IU/L), and an indirect bilirubin level of 1.9 mg/dL (reference range, 0.1–0.8 mg/dL). Haptoglobin was undetectable, while both direct antiglobulin test (DAT) and indirect antiglobulin test (IAT), also known as direct and indirect Coombs tests, were positive, and antinuclear antibody test was negative. Anti-e antibodies were detected upon examination of irregular antibodies. Computed tomography showed a left ovarian tumor (6 cm in diameter) without lymphadenopathy or obvious hepatosplenomegaly (Figure 1(a)). Magnetic resonance imaging revealed a suspected mature cystic teratoma (Figures 1(b) and 1(c)). In the peripheral blood sample, α-fetoprotein was 6 ng/mL, squamous cell carcinoma antigen was 0.5 ng/mL, carbohydrate antigen 125 was 19 U/mL, and human epididymis protein 4 was 63 pico-mol/L, respectively. These tumor markers were not elevated.
The patient was diagnosed with AIHA and administered prednisolone orally at a dose of 55 mg/day, which improved their anemia. One month after initiating prednisolone therapy, laparoscopic oophorocystectomy was performed. Macroscopic examination of the tumor revealed the presence of fluid, cartilage, skin, and skin appendages. The tumor was pathologically diagnosed as a mature cystic teratoma (Figure 1(d)), and microscopic examination did not reveal any cells indicative of hematological malignancies within the tumor. The patient's anemia was normalized postoperatively without the need for blood transfusion. Four months after surgery, both the DAT and IAT results were negative (Figure 2).
We hypothesized that antibodies would be present in the fluid layer and, therefore, examined it. Additional studies were performed to clarify the relationship between tumors and AIHA.
2.1. Study Samples
After obtaining informed consent, laparoscopic oophorocystectomy was performed, and the mature cystic teratoma was resected. During the surgery, intratumor contents were extracted under sterile conditions. The tumor liquid contents were then centrifuged at 3000 g for 5 min at room temperature twice to remove impurities. The sample supernatant was used for further analysis.
2.2. IAT of the Mature Cystic Teratoma Contents
To perform the IAT on the tumor contents, the serous contents of mature cystic teratoma and the patient's serum were diluted with normal saline as 1 : 10, 1 : 100, 1 : 1000, and 1 : 10000. Ten percent of group O RBCs were incubated with the tumor fluid or patient's serum at 37.0°C for 30 minutes. After incubation, the treated RBCs were washed three times with normal saline. The IAT was performed using a polyclonal anti-immunoglobulin G (IgG) antibody, and any irregular antibodies were examined using a Data-Cyte Plus kit (Grifols, Barcelona, Spain).
2.3. Results
The IAT performed on the contents of the mature cystic teratoma showed agglutination at all tested dilutions of the tumor extract (ranging from 1 : 10 to 1 : 10,000), a reaction more pronounced than that observed with the patient's own serum (as depicted in Figure 3(a)). When screening for irregular antibodies within the tumor, there was no reactivity to anti-e antibodies.
Capillary electrophoresis was employed on both the tumor extract and the patient's serum collected before any treatment. The protein fraction of the tumor contents showed an increase in the β1-globulin fraction and a slight increase in the γ-globulin fraction (Figure 3(b)), which was not observed in the patient's serum harvested before treatment (Figure 3(c)). Furthermore, immunofixation electrophoresis of the tumor contents revealed monoclonal antibodies of IgG-κ type (Figure 3(d)).
3. Discussion
In this report, we described a case of secondary AIHA effectively managed in a patient with mature cystic teratomas.
Although there have been case reports of AIHA associated with mature cystic teratoma in recent years [4–6], the exact mechanism between mature cystic teratoma and AIHA remains elusive. However, several theories have been proposed regarding the etiology of secondary AIHA associated with mature cystic teratomas, including (1) immune responses against abnormal RBCs; (2) changes in RBC antigenicity caused by tumor-derived substances, like haptens; and (3) in situ antibody production within the tumor tissue, possibly by lymphoid cells [7].
Our literature review uncovered 12 previous cases of secondary AIHA linked to mature cystic teratomas where the IAT on intratumor contents (tumoral-IAT) was conducted (Table 1) [7–17]. Previous cases of secondary AIHA associated with mature cystic teratomas containing lymphocytes or plasma cells within the tumor cyst support the third theory [7, 11]. Besides, it was noted that patients with positive tumoral-IAT results demonstrated an 83% response to steroid treatment, which was notably higher than the 40% response rate in patients with negative tumoral-IAT. Also, the effectiveness of surgical removal of the tumor implies that the tumor tissue itself possesses the causative key for AIHA occurrence. Thus, in the case of positive tumoral-IAT, the pathophysiology of AIHA associated with mature cystic teratoma might be explained by in situ antibody production within the tumor tissue. There is a possibility that steroid therapy followed by tumor resection may be effective.
Furthermore, our case is notable due to the comparatively higher titer of tumoral-IAT than serum-IAT and the detection of monoclonal IgG within the tumor fluid. Although our examination did not reveal any hematological malignancies, the heightened agglutination in the tumoral-IAT and the presence of monoclonal IgG within the tumor strengthen the theory of intratumoral lymphocytes' role in anti-RBC antibody production. Further investigative work is needed to clarify the precise mechanisms at play in secondary AIHA.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hansen D. L. Möller S. Andersen K. Gaist D. Frederiksen H. Increasing incidence and prevalence of acquired hemolytic anemias in Denmark, 1980-2016 Clinical Epidemiology 20201249750810.2147/CLEP.S 25025032547241 PMC 7250289 · doi ↗ · pubmed ↗
- 2Hill Q. A. Stamps R. Massey E. Guidelines on the management of drug-induced immune and secondary autoimmune, haemolytic anaemia British Journal of Haematology 2017177220822010.1111/bjh.146542-s 2.0-8501717250228369704 · doi ↗ · pubmed ↗
- 3Kamesaki T. Autoimmune hemolytic anemia as a paraneoplastic syndrome associated with solid tumors Rinshō Ketsueki 201556777878410.11406/rinketsu.56.7782-s 2.0-8494613449726251140 · doi ↗ · pubmed ↗
- 4Felemban A. A. Rashidi Z. A. Almatrafi M. H. Alsahabi J. A. Autoimmune hemolytic anemia and ovarian dermoid cysts in pregnancy Saudi Medical Journal 201940439740010.15537/smj.2019.4.24l 0730957135 PMC 6506659 · doi ↗ · pubmed ↗
- 5Martellosio J. P. Landron C. Milin S. Traitement chirurgical d’une anémie hémolytique auto-immune La Revue de Médecine Interne 201839643543810.1016/j.revmed.2018.03.0182-s 2.0-8504510108729650300 · doi ↗ · pubmed ↗
- 6Nii M. Kondo E. Maki S. Safety and efficacy of laparoscopic oophorocystectomy for ovarian dermoid cyst associated with autoimmune hemolytic anemia Gynecology and Minimally Invasive Therapy 201871273010.4103/GMIT.GMIT_9_172-s 2.0-8506975835030254931 PMC 6135149 · doi ↗ · pubmed ↗
- 7De Bruyère M. Sokal G. Devoitille J. M. Fauchet-Dutrieux M. C. De Spa V. Autoimmune haemolytic anaemia and ovarian tumour British Journal of Haematology 1971201839410.1111/j.1365-2141.1971.tb 00789.x 2-s 2.0-00149718995540043 · doi ↗ · pubmed ↗
- 8Allibone E. C. Collins D. H. Symptomatic haemolytic anaemia associated with ovarian teratoma in child Journal of Clinical Pathology 19514441242010.1136/jcp.4.4.4122-s 2.0-000043191414897918 PMC 1023472 · doi ↗ · pubmed ↗