Heart rate variability biofeedback to reduce anxiety in autism spectrum disorder – a mini review
Helen L. Coulter, Mark P. Donnelly, Anita Yakkundi, Helen McAneney, Owen G. Barr, W. George Kernohan

TL;DR
This review examines how heart rate variability biofeedback can help reduce anxiety in people with autism spectrum disorder.
Contribution
The paper provides a mini review of heart rate variability biofeedback's effectiveness for anxiety in autism, highlighting gaps and future research directions.
Findings
Heart rate variability biofeedback shows positive short-term effects on anxiety in autism.
Long-term follow-up and accurate assessment methods are needed for reliable outcomes.
Future studies should consider device types, training settings, and additional measures like cortisol.
Abstract
There is a reported high prevalence of anxiety in people with autism spectrum disorder. This mini review appraises existing research investigating heart rate variability biofeedback to help manage symptoms of anxiety in people with autism spectrum disorder. A thorough search of electronic databases was conducted to find relevant literature. Consultation with experts and a librarian helped develop search terms following the PICO framework. Five databases were searched, and screening was undertaken using Covidence software, with the process outlined in a PRISMA flowchart. The latest review showed positive short-term effects but there is a need for long-term follow-up. Future investigations should consider device type, training settings, and control interventions. Accurate heart rate variability assessment independent of biofeedback devices is crucial. Additional measures like cortisol…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
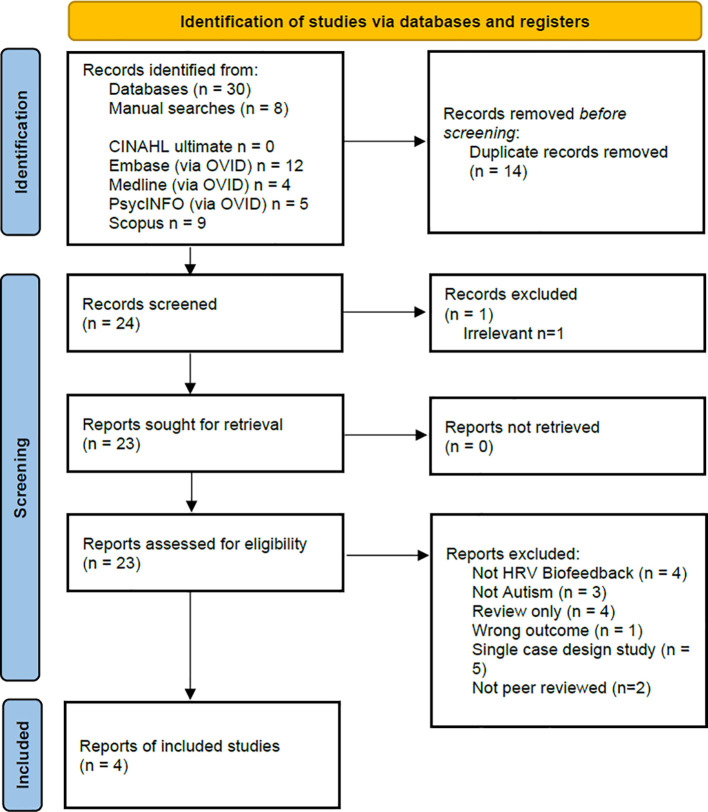 Figure 1
Figure 1| Population | Intervention | Comparator | Outcome |
|---|---|---|---|
| Autism* Asperger* | Biofeedback | – | Heart rate variability |
|
| Papers included in review (author & year) | |||
|---|---|---|---|---|
| ( | ( | ( | ( | |
| Country | USA | USA | UK | Belgium |
|
| ||||
| Population | ASD & non-ASD | Clinical diagnosis of ASD | Clinical diagnosis of ASD + previous attendance in health services for anxiety | Clinical diagnosis of ASD |
| Age range | Young adults - range not specified | 9–18 years | 13–22 years | 13–18 years |
| Sample size (ASD) | n=10 | n=15 | n=20 | n=44 (Supervised HRVB 24; Sham control 20) |
| Demographics | Gender | Age, gender, IQ | Age, gender, sleep, medication | Formal diagnosis of ASD (excluded people with intellectual disabilities), gender, age |
|
| ||||
| Design | 2 group design | 2 group design investigating two types of biofeedback intervention | 2 group design investigating adoption & usability in home setting | A single-blind, randomized sham-controlled pilot trial with between subject design was used. Trial of HRVB vs Sham control over five-week period (T1), followed a second five-week study (T2) of randomized home-non supervised vs non-treatment group. |
| Recruitment | Autism advisor | Autism group, school, online | Therapists, flyers at clinics | Autism centre, autism research group, special education schools, clinical practices, advocacy organisations |
| Random allocation | No | Yes | Yes | Yes |
| Concealment | No | No | No | Yes |
| Measures | ||||
| Parent/carer questionnaire | No | Spence Anxiety Scale; Emotion | Social Communication Questionnaire (ASD rating) | Parents completed: Social responsiveness scale; Repetitive Behaviour Scale – Revised; Strengths and Difficulties Questionnaire |
| Participant questionnaire | No | No | Beck Anxiety & Beck Depression inventory/ | Adolescents self-report tools: Strengths and Difficulties Questionnaire; Perceived Stress Scale; Depression, Anxiety and Stress scale – 21; Visual Analogue Scale for sensory hypersensitivity; Visual Analogue Scale for perceived stress |
| Physiological testing | No | QEEG/Respiration/ECG | ECG (Actiwave Cardio) | Three lead ECG/Breathing frequency (using an elastic band with stretch sensitive sensors)/Salivary Cortisol |
| Adoption | Attrition rates calculated | Amount of home practice | Amount of home practice | Compliance rates for supervised HRVB and sham training (T0, T1) and home-based HRVB (T1 and T2) |
| Usability | No | No | System Usability Scale | |
| Equipment | emWave desktop (HeartMath) | BioGraph Infiniti software 6.0 | StressEraser/Inner Balance | NeXus- 10 MKII and BioTrace+ software |
|
| ||||
| Non-ASD students | HRVB + Mu Rhythm Synchrony neurofeedback combined | Delayed intervention | Sham HRVB control | |
|
| ||||
| Analysis type | Exploratory data analysis | Statistical analysis | Pre-post analysis of mean differences in reported anxiety and depression. | Statistical analysis, including mixed effect analysis. Analysis of mean differences across HRVB and Sham groups |
| Findings | ASD participants showed an increase in mean HRV scores compared to students without autism in the second five weeks of the study. | HRVB group - Increased emotion regulation and social behaviour. | Reduction in Anxiety post intervention | Supervised HRVB resulted in a late increase in cardiac vagal modulation in adolescents with autism. |
|
| ||||
| Initial training | Initial training x 4 sessions | Initial training 2 x30 min | Phase 1: 30 min training and supervised practice session in clinic one day a week, and parallel 20min/day home session for 5 weeks. Phase 2: non-supervised 20 min home practice for 5 weeks | |
|
| ||||
| Institute Higher Education | Clinic intervention + home practice | Home intervention + practice | Clinic intervention + home practice | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHeart Rate Variability and Autonomic Control · EEG and Brain-Computer Interfaces · Attention Deficit Hyperactivity Disorder
Introduction
Heart rate variability (HRV) is a term used to describe the natural variability in heart rhythm which reflects the activity of both the sympathetic and parasympathetic actions of the autonomic nervous system (1). HRV is a complex variable which constantly changes according to the individual’s responses to their environment, and which also declines with age (2, 3). A detailed review of HRV metrics has been produced (4) and normative values have been reported (5, 6). A number of theoretical models have been proposed describing the links between HRV and health, mediated via connections between the heart and the brain (7–9). HRV is now frequently used as a physiological marker and is considered a sensitive indicator of the stress response (10) and an index of an individual’s ability to self-regulate behaviour (11).
Biofeedback involves monitoring physiology by actively involving the user, enabling them to learn to change their unique physiological responses to improve health (12). Several systematic reviews have been conducted highlighting the potential of biofeedback as a cost-effective digital health intervention to help people manage anxiety (13, 14). A review of the types of biofeedback modalities and devices being trialled for stress management has been carried out by Yu et al. (15). HRV measurement has been used in conjunction with sensor technology to develop a form of biofeedback now referred to as heart rate variability biofeedback or HRVB (16). HRVB involves breathing training to develop a phenomenon called Respiratory Sinus Arrhythmia (RSA), where heart rate acceleration and deceleration synchronizes with respiration and typically occurs when breathing is slowed to a rate between 4.5–7 breaths per minute (17). A guide to the process of HRVB training to develop what has been termed ‘Resonance Frequency’ breathing has been outlined (18) and the possible mechanisms of effect underlying HRVB have been described (19, 20). Several meta-analytic reviews have now demonstrated efficacy for HRVB to reduce anxiety in a range of populations (14, 21).
People with autism spectrum disorder (ASD) frequently experience high levels of anxiety (22, 23) and reviews have indicated higher prevalence rates of anxiety in young people with ASD, in comparison with typically developing peers (24). A range of interventions have been employed to treat anxiety in people with ASD (25). Despite widespread use of medication, the evidence for its effectiveness is limited and side effects and adverse events can occur (26). There is evidence for effectiveness of interventions such as cognitive behavioural therapy adapted for people with ASD (27), however the availability of interventions for anxiety is limited by difficulties with adoption of interventions (28) and lack of support and training for those working with people with ASD (29).
As a non-invasive digital health solution, HRVB may represent a useful method of engaging people with ASD. HRVB removes the complex social and communication demands of traditional cognitive and behavioural therapies (30), bypasses the risks of medication and through often intuitive digital displays, leverages the characteristic visual strengths and interests of people with ASD. People with ASD do, however, present with a wide range of differences in physiological reactions compared to neurotypical peers (31–33) and further investigation into interventions to help improve autonomic system regulation may be particularly important.
This paper presents a review conducted to assess and summarise literature that currently exists on the use of HRVB in people with Autistic Spectrum Disorder (ASD).
Methodology
A comprehensive search of electronic databases followed by the screening of the articles was undertaken to identify relevant literature. In consultation with experts in the areas of ASD and HRV, and then further refinement with advice from a subject librarian, the search terms were developed and followed the PICO framework (Population, Intervention, Comparator and Outcome) (34). These search terms are listed in Table 1 and were combined using Boolean logic. Five databases, CINAHL ultimate, Embase (via OVID), Medline (via OVID), PsycINFO (via OVID) and Scopus were searched to capture relevant literature across the domains represented by these databases. An initial search was carried out on 19^th^ July 2017, with no date restrictions applied, and further updated with the final search performed on 16^th^ November 2023, in which relevant publications between 2017 and 2023 were then added to form the full list of included studies in this mini review. Inclusion and exclusion criteria applied during the screening process are also outlined in Table 1. That is, the inclusion of peer reviewed research articles, with no restriction on date published or language. Papers were excluded if not ASD/autism, not HRV/biofeedback, no English abstract, or if it was a review article or of a single case study design. Only peer reviewed articles were included in the review. Single case studies were also excluded as they were viewed to lack generalisability due to their focus on a singular instance, limiting the applicability and reliability of findings in broader contexts.
The screening process was facilitated using the software Covidence (35), which automatically removes duplicates. Articles were initially screened by title and abstract, carried out by HC & AY, followed by full text screening. A PRISMA flowchart provides an overview of this screening process (36).
Summary details of included articles were then extracted, including details of population, intervention, comparator, and outcome aspects, followed by an assessment of the study, using the CASP framework (37) as a guide, which was carried out in duplicate.
Results
An overview of the screening process is provided in the PRISMA flowchart (36) presented in Figure 1. In total 38 articles were returned, 30 from the searches of the five databases (CINAHL ultimate n = 0, Embase (via OVID) n = 12, Medline (via OVID) n = 4, PsycINFO (via OVID) n = 5, Scopus n = 9) and 8 additional articles from manual searches. After duplicates were removed, 24 articles were screened for inclusion with 20 articles excluded for the reasons as listed in Figure 1. Four remaining articles are included in this review (38–41).
PRISMA Flowchart (36) showing the overview of the identification of and screening of studies for inclusion in this review.
Table 2 summarises the extracted data and critical assessment of the four included articles. Two of the four articles are published within the last two years (40, 41), with two studies conducted in the USA (38, 39), one in the UK (40) and one in Belgium (41). The design of the interventions in these studies varies but all comprise exploratory or pilot studies, with appropriately small sample sizes. Across the papers, there is variation in the measures used and demographics reported.
Discussion
Based on a review of existing literature on the use of HRVB in people with ASD, several themes emerge regarding current studies and several recommendations are made for the development of future research in this area.
Analysis of the studies reviewed here highlight wide variations in study design and the methodologies employed, which have employed different devices, training protocols and diverse outcome measurements. The current studies all provide important information on specific areas of focus and are typical of early-stage research under development however the heterogeneity of design makes direct comparisons difficult. This problem has been highlighted in several biofeedback reviews (15, 42) and there is a clear need for larger randomised control studies particularly with this new population. The most recent study reviewed in this paper, Thoen et al. (41), did employ this type of design and showed some positive effects for HRVB but also highlighted the need for more follow up to assess the longer-term effects of HRVB for ASD populations.
The type of biofeedback device used, and the type and location of training employed may also be important to consider in future investigations. Two studies reviewed here employed more real-world training in either school or home environments (38, 40) and did not adopt protocols using multi sensor devices in a clinical environment. Whilst this type of study remains problematic in terms of standardising environment conditions the need for follow up testing of devices in real world situations with clinical populations has been emphasized (43).
Resonance frequency breathing rates within individuals may not remain stable over time (44, 45) and assessing any HRVB intervention in conjunction with repeated HRV measures and age-related HRV norms is vital. The type of control intervention used may also be important. As noted by Goodman et al. (39), it is possible that simply teaching diaphragmatic breathing alone may be enough to create changes in symptoms such as anxiety. This type of slow breathing intervention has been shown to have positive effects (46, 47) and may be useful as an active control intervention in future studies to assess its effects on HRV in people with ASD.
A further issue highlighted by this review is the need to accurately assess and record HRV independently from biofeedback devices. We argue that studies should include measures of HRV measured via 12-lead ECG which are independent from the biofeedback device itself. Heart rate variability is now a commonly collected data variable which can be measured via apps on iPhones and activity trackers. However, this belies the complexity underlying the multiple influences which contribute to HRV on a moment-to-moment basis (3). The increasing number of studies now assessing HRV and the variability of data collection, analysis, and reporting, highlight the need to adhere to standardize data collection according to agreed guidelines (48). Separate independent measurement of HRV pre and post intervention is needed to elucidate whether HRVB practice does change HRV responses.
The importance of using additional measures of participants reactions is recommended to help elucidate the links between biofeedback and anxiety in ASD. The use of physiological assessments such as cortisol assessment (41) and the use of tests of EEG functioning (39) represent valuable methods of gathering vital information on physiological and neurological reactions.
The involvement of both users and carers in providing direct reports on symptoms and perceived stress in this population is also seen as a vital area which is needed. The use of participant reports on levels of stress and sources of stress (40, 41) and usability reports on device function highlight how user input can help to develop future work and highlight risks and benefits of an intervention.
Assessing the longer-term effectiveness of any intervention is important, and the use of remote monitoring to assess home practice and stress levels will be important in future work to assess adoption and usage of any intervention in this area. In addition, capturing and recording data from the biofeedback devices or from home practice reports as used by Goodman et al. (39) may help assess whether there is a dose response relationship for this type of intervention.
Several key issues are apparent regarding the specific vulnerabilities of people with ASD. Foremost in this area is the need for larger studies to establish normative values for HRV in people with ASD under a range of conditions. Several previous studies assessing the physiological responses of people with ASD have indicated that this population may have different responses to stress compared to neurotypical peers (33) and increased levels of anxiety and depression (23, 24). Assessment of autonomic nervous system functioning, and physical and mental health conditions is particularly important for people with ASD considering the increased level of these co-morbidities in this population (49–51).
In addition, the use of the ‘stress test’ paradigm may not be appropriate or indeed ethical to use for people with ASD. One feasibility study reviewed here noted that the level of ASD symptoms was correlated with increased heart rate during a stress test and noted several previously undetected mental health and cardiac health difficulties in participants during assessments (40). Recent systematic reviews have highlighted links between heart disease and ASD (52, 53) and the implications of these issues should be considered in future studies. Further work in this area should consider not employing a stress test paradigm for people with ASD and instead should consider longer term HRV recording (54) or repeated daily recordings under rest conditions and follow standardised recording and assessment guidelines (48). In addition, recording severity of symptoms in individuals with a diagnosis of ASD, as well as levels of mental and physical health symptoms pre and post intervention are important to provide more accurate information on the links between ASD and HRV.
Conclusion
ASD is now a common condition (55) with significant economic health care costs (56, 57). Providing interventions for symptoms that affect the day to day lives of people with ASD such as anxiety have been emphasized as a vital area for research (58, 59). Despite concerns regarding overuse, there has also been a recognition of the potential for digital technology to manage the growing levels of mental health in the general population to help reduce the increasing burden of mental illness (60, 61). HRVB has been found to be an important adjunct to existing interventions for neurotypical populations with mental health conditions (62, 63) and people with ASD should not be excluded from any future research developments in this area (64, 65).
We argue that there exists evidence from recent studies to suggest the potential for this intervention to help people with ASD manage anxiety. Future studies should aim to address some of the issues outlined in this review to determine both the type and level of intervention appropriate in this vulnerable population and to further assess the mechanism of effect of HRVB.
Author contributions
HC: Writing – original draft, Writing – review & editing. MD: Writing – original draft, Writing – review & editing. AY: Writing – original draft, Writing – review & editing. HM: Writing – review & editing. OB: Writing – review & editing. WK: Writing – original draft, Writing – review & editing.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability. Standards of measurement, physiological interpretation, and clinical use. Eur Heart J. (1996) 17:354–81. doi: 10.1093/oxfordjournals.eurheartj.a 014868 8737210 · doi ↗ · pubmed ↗
- 2Shaffer F Mc Craty R Zerr CL. A healthy heart is not a metronome: an integrative review of the heart's anatomy and heart rate variability. Front Psychol. (2014) 5:1040. doi: 10.3389/fpsyg.2014.01040 25324790 PMC 4179748 · doi ↗ · pubmed ↗
- 3Lombardi F Huikuri H Schmidt G Malik M. e-Rhythm Study Group of European Heart Rhythm Association. Short-term heart rate variability: Easy to measure, difficult to interpret. Heart Rhythm. (2018) 15:1559–60. doi: 10.1016/j.hrthm.2018.05.023 29803853 · doi ↗ · pubmed ↗
- 4Shaffer F Ginsberg JP. An overview of heart rate variability metrics and norms. Front Public Health. (2017) 5:258. doi: 10.3389/fpubh.2017.00258 29034226 PMC 5624990 · doi ↗ · pubmed ↗
- 5Nunan D Sandercock GR Brodie DA. A quantitative systematic review of normal values for short-term heart rate variability in healthy adults. Pacing Clin electrophysiology: PACE. (2010) 33:1407–17. doi: 10.1111/pace.2010.33.issue-11 20663071 · doi ↗ · pubmed ↗
- 6Dantas EM Kemp AH Andreão R Vda Silva VJD Brunoni AR Hoshi RA. Reference values for short-term resting-state heart rate variability in healthy adults: Results from the Brazilian Longitudinal Study of Adult Health-ELSA-Brasil study. Psychophysiology. (2018) 55:e 13052. doi: 10.1111/psyp.13052 29292837 · doi ↗ · pubmed ↗
- 7Porges SW. The polyvagal theory: phylogenetic substrates of a social nervous system. Int J Psychophysiol. (2001) 42:123–46. doi: 10.1016/s 0167-8760(01)00162-3 11587772 · doi ↗ · pubmed ↗
- 8Thayer JF Lane RD. A model of neurovisceral integration in emotion regulation and dysregulation. J Affect Disord. (2000) 61:201–16. doi: 10.1016/s 0165-0327(00)00338-4 11163422 · doi ↗ · pubmed ↗