Endoscopic treatment of a large Brunner’s gland hamartoma in the duodenum
Ha Eun Lee, Gwang Ha Kim, Kyungbin Kim

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
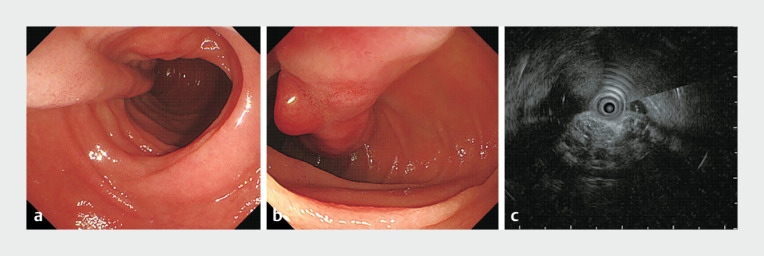 Fig. 1
Fig. 1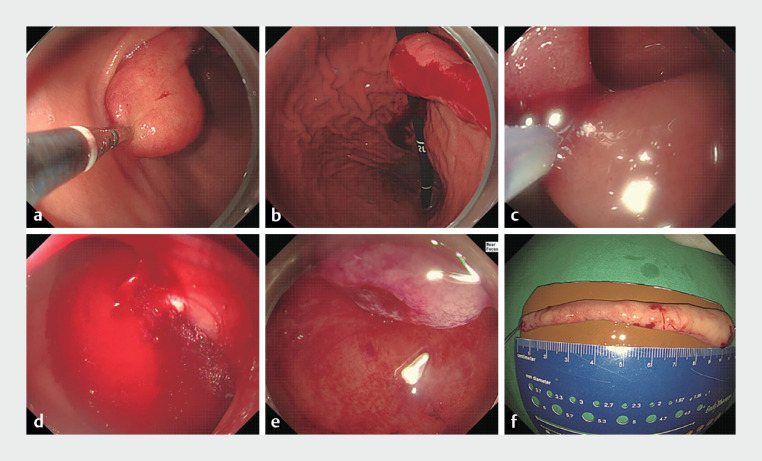 Fig. 2
Fig. 2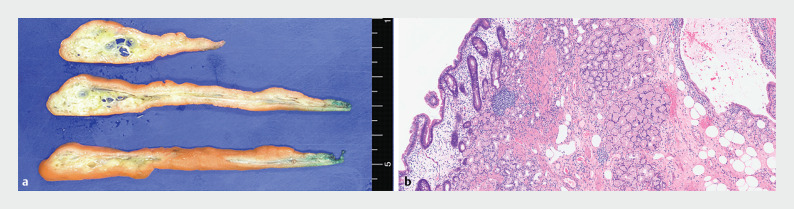 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal Tumor Research and Treatment · Gastrointestinal disorders and treatments · Sarcoma Diagnosis and Treatment
A 62-year-old woman visited our hospital for further evaluation of a large elongated polypoid mass in the duodenum, which was incidentally discovered during a health check-up endoscopy. The patient had a medical history of hypertension and hyperlipidemia. At endoscopy, a 10-cm subepithelial mass with a long stalk was observed in the second portion of the duodenum ( Fig. 1 a ); nodular mucosal changes were observed in the distal portion of the mass ( Fig. 1 b ). Endoscopic ultrasonography (EUS) revealed that the mass was a heterogeneously mixed echogenic lesion with cystic changes in the deep mucosal and submucosal layers Fig. 1 c ).
A duodenal subepithelial mass is seen on: a, b endoscopy; c endoscopic ultrasonography showing: a a 10-cm subepithelial mass with a long stalk in the second portion of the duodenum; b nodular mucosal changes in the distal portion of the mass; c a heterogeneously mixed echogenic mass with cystic changes in the deep mucosal and submucosal layers.
Endoscopic mucosal resection was planned to exclude the possibility of malignancy owing to the nodular mucosal changes on the surface of the mass and its large size ( Video 1 ). Because we were unable to place the snare at the base of the mass, it was first expelled from the duodenum into the stomach using mucosal forceps ( Fig. 2 a, b ). The snare was then placed at the base of the mass and the resection was performed ( Fig. 2 c ). Spurting bleeding occurred after the tumor resection ( Fig. 2 d ); however, hemostasis was successfully achieved by ligation using an O-ring ( Fig. 2 e ).
Endoscopic resection of a large Brunner’s gland hamartoma.Video 1
Endoscopic images of the resection of a duodenal subepithelial mass showing: a, b the mass being expelled from the duodenum to the stomach using mucosal forceps; c the snare being placed at the base of the mass, before resection is performed; d spurting bleeding after tumor resection; e successful hemostasis by ligation using an O-ring. f Photograph of the resected specimen, which was a 10.0 × 1.7-cm elongated subepithelial mass.
The resected specimen was a long polypoid subepithelial mass, measuring 10.0 × 1.7 cm ( Fig. 2 f ). Histopathologically, the mass comprised of proliferating adipose tissue and hyperplastic Brunner’s glands in the deep mucosa and submucosa, consistent with a Brunner’s gland hamartoma (BGH) ( Fig. 3 ). No dysplastic areas were observed in the resected tumor. The patient’s post-procedural course was uneventful and she was discharged on postoperative day 3.
Histopathologic findings showing: a on gross evaluation, a well-defined heterogeneous yellow-to-white solid mass with cystic changes mainly located in the deep mucosa and submucosa; b microscopically, proliferating adipose tissue and hyperplastic Brunner’s glands, consistent with a Brunner’s gland hamartoma (hematoxylin and eosin [H&E] stain, magnification × 100).
BGH is a benign proliferative disorder of the Brunner’s glands in the duodenum 1 . It is often discovered incidentally during endoscopy, with typical findings indicating mucosal protrusions or polyps 2 . The American Institute of Radiologic Pathology categorizes lesions <5 mm as “Brunner’s gland hyperplasia” and those >5 mm as “BGH” 3 . The exact pathogenesis of BGH remains unknown. Although it is commonly regarded as a benign duodenal condition, it can enlarge and cause gastrointestinal bleeding or obstruction. In addition, malignant transformation can occur, especially when there is a significant increase in size or the presence of a shallow central depression on its surface 3 . Treatment depends on the tumor size, symptoms, and the possibility of malignancy. Previously, surgical resection was the primary treatment modality. Given however that the BGH is located in the deep mucosa and submucosa, endoscopic resection can be successfully performed, as in the present case, even when it is large.
Endoscopy_UCTN_Code_CCL_1AB_2AC_3AB
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lee KJ Park B Kim HM Endoscopic ultrasonography findings for Brunner’s gland hamartoma in the duodenum Clin Endosc 20225530530910.5946/ce.2020.25933906330 PMC 8995996 · doi ↗ · pubmed ↗
- 2Choe Y Cho YK Kim GH Prevalence, natural progression, and clinical practices of upper gastrointestinal subepithelial lesions in Korea: a multicenter study Clin Endosc 20235674475310.5946/ce.2023.00537621066 PMC 10665619 · doi ↗ · pubmed ↗
- 3Patel ND Levy AD Mehrotra AK Brunner's gland hyperplasia and hamartoma: imaging features with clinicopathologic correlation AJR Am J Roentgenol 200618771572210.2214/AJR.05.056416928936 · doi ↗ · pubmed ↗