Ureteral stent encrustation in an HIV patient treated with disposable flexible ureteroscope: a case report
Lin Xiong, Nga-nuen Loo, Zhen-Quen Lu, Xiang Xu, Genggeng Wei

TL;DR
An HIV patient with a kidney stone and ureteral stent encrustation was successfully treated using a disposable flexible ureteroscope.
Contribution
Demonstrates the effectiveness of disposable flexible ureteroscopes in treating HIV patients with ureteral stent encrustation.
Findings
Ureterolithotripsy with a disposable flexible ureteroscope was performed successfully.
The patient's postoperative recovery was favorable.
The procedure is effective for HIV patients with ureteral stent encrustation.
Abstract
Human immunodeficiency virus prevalence was increasing worldwide. Medication-associated urinary calculi are very commonly caused by medications used to treat HIV-positive patients. We present a case of an HIV-positive 39-year-old male with ureteral stent encrustation and kidney stone. Ureterolithotripsy using a disposable flexible ureteroscope is performed. The postoperative evolution was favorable. The disposable flexible ureteroscope is effective in the treatment of HIV combined with ureteral stent encrustation.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
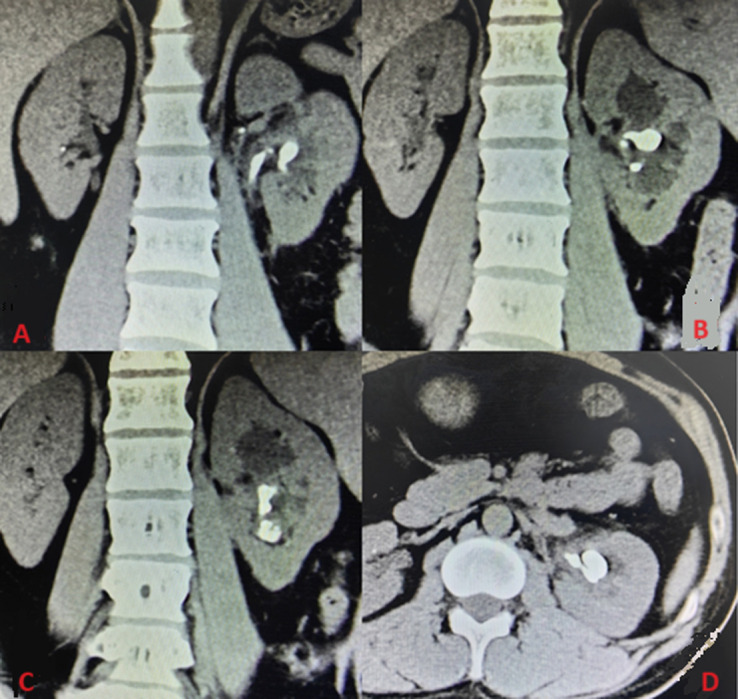 Figure 1
Figure 1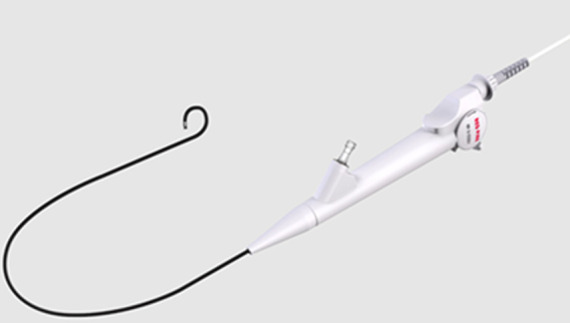 Figure 2
Figure 2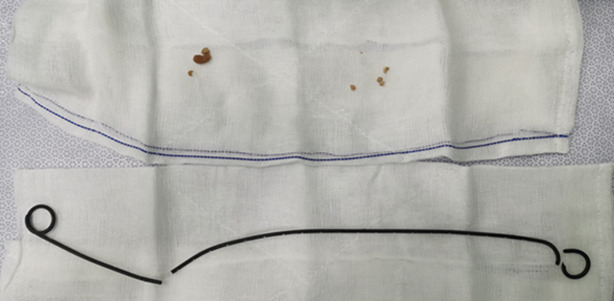 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsKidney Stones and Urolithiasis Treatments · Dialysis and Renal Disease Management · Renal and Vascular Pathologies
Introduction
The global prevalence of human immunodeficiency virus (HIV) was increasing worldwide. Urolithiasis is a common urological disease and the procedure of ureteral stent implantation is often performed after its management. The number of HIV-positive patients with calcified ureteral stents is increasing every year. When ureteral stents are indwelling for an extended length of time, some of them become calcified, causing issues such as extraction difficulties [1]. We report a case of urethral stent encrustation combined with a kidney stone in an HIV patient.
Patient and observation
Patient information: we present a case of a 39-year-old male patient, HIV-positive, non-smoker, and non-alcoholic.
Clinical findings: the patient is asymptomatic. He had no pain, no fever, no nausea, and no vomiting. He had neither a renal infection nor blood in the urine. The patient´s renal function is not affected. During physical examination, the patient only showed costovertebral angle tenderness. The rest of the examination findings are unremarkable.
Timeline of the current episode: in 2020, the patient was diagnosed with HIV-positive and started treatment for HIV. In March 2021, the left laparoscopic ureterolithotomy and urethral stenting were performed. In October 2021, there was a follow-up after surgery. Urological computed tomography (CT) was performed. Phase one of left transurethral lithotripsy and urethral stent replacement were performed. In November 2021, phase two of left transurethral lithotripsy and urethral stent replacement were performed. Renal stone analysis was performed. In December 2021, the urological CT was performed and the urethral stent was removed.
Diagnostic assessment: the patient´s CT+T lymphocyte count was ≥ 200 cells/μl and the HIV load is > 500. Urological computed tomography was performed. It showed that there is a retained ureteral stent calcification and a left kidney stone. The size of the calcification on the left ureteral stent is 16 mmx11 mm, with a CT maximum value of 1485 and a mean value of 1155 (Figure 1).
computed tomography showing ureteral stent encrustation and kidney stones; A,B) ureteral stent and ureteral stent encrustation; C) kidney stones located in the renal pelvis and subrenal calyx; D) kidney stones of CT cross-sectional imaging
Diagnosis: a diagnosis of ureteral stent encrustation and kidney stone was made.
Therapeutic interventions: after thorough examinations, the patient underwent transurethral left ureteral flexible lithotripsy and left ureteral stent replacement. Intraoperatively, there was no obvious calcification in the bladder segment and the ureteral segment of the ureteral stent. These segments of the ureteral stent were cut with a holmium laser with the power set to 1.2j/5hz and then removed in sections. Then, the ureteral access sheath was inserted and adjusted to slightly below the pelvic. Redpine disposable flexible ureteroscope (Figure 2) was then positioned. the remaining ureteral stent was found to have obvious calcification. The stones were fragmented with the holmium laser power was set to 0.6j/50hz. The remaining ureteral stents were removed using a lithotripsy extraction basket (Figure 3). Due to the significant stone load, a second operation was performed. The surgery was carried out one month later with transurethral left ureteral flexible lithotripsy and replacement of the left ureteral stent. This operation also utilizes the red pine disposable flexible ureteroscope. During this operation, the residual kidney stones were fragmented and the residual stones bigger than 2 mm were removed using a lithotripsy extraction basket. The stones from both surgeries were analyzed as a mixture of calcium oxalate dihydrate and calcium hydrogen phosphate dihydrate. A 5F polaris ultra ureteral stent was placed after both procedures.
disposable red pine flexible ureteroscope; the single-used flexible urethroscope used during the surgery
the segment of the ureteral stent obtained after the surgery; it is broken into three parts
Follow-up and outcome of interventions: a urological CT was performed and suggested no residue stone. The urethral stent was then removed.
Patient perspective: “I was quite worried that my HIV status would contaminate the tools and harm other patients or medical personnel. However, I was rather relieved to learn that they would be utilizing urethroscopes that could only be used once.”
Informed consent: the patient gave a written informed consent.
Discussion
Ureteral stents are generally routinely used in urology, whether for flexible ureteroscopic lithotripsy, percutaneous nephrolithotripsy, or laparoscopic ureterotomy for stone extraction. In clinical practice, calcification is typical following protracted stent installation. Various variables, such as stent material and bacterial colonization, can influence stent calcification, but the most significant risk factor is the period of ureteral stent retention. Kawahara [2] in their study, reported stent encrustation rates of 26.8% at less than 6 weeks, 56.9% at 6 to 12 weeks, between 6 to 12 weeks, and 75.9% at more than 12 weeks of indwelling time. In our case, the patient had a ureteral stent indwelling for more than 6 months and showed calcification on the pelvic segment of the ureteral stent. There are several different clinical criteria for grading ureteral stent calcification. According to the FECal classification [3], our case belongs to grade 3. According to the KUB criteria [4], our case has a K score of 4, U score of 1, and a B score of 1, with a total of 6. According to Singh I classification [5], our case is classified as mild encrusted. Our case was categorized as mild encrusted based on all three classification criteria. Cicione A [6] and other researchers recommended the KUB criteria as a better predictor of the requirement for numerous procedures.
A tiered approach to surgery is advised because ureteral stent tube calcification typically requires severe treatments. An average of 3±1.08 operations per patient was reported by Thangavelu M et al. [7] for 13 cases. In our case, the first procedure was primarily to remove the calcification ureteral stent, and the second operation was to treat any remaining kidney stones.
There is no conventional therapy for ureteral stent calcification, which may generally be addressed by several combinations of surgical techniques, depending on the location of the calcification and the degree of calcification. Thangavelu M et al. [7] reported 13 management modalities for ureteral stent calcification: eight that involved bladder lithotripsy, ureteroscopy (URS), and retrograde intrarenal surgery (RIRS), two that involved URS and extracorporeal shock wave lithotripsy (ESWL), two that involved bladder stone, URS, RIRS, and ESWL. According to Torricelli FC's report [8], there was a considerably higher chance of bleeding in HIV patients who underwent percutaneous nephrolithotomy for upper urinary tract stones. This encompasses not just the patient's danger, but also the risk to the health care practitioner. Ureteroscopic flexible surgery minimizes the risk of occupational exposure to the surgeon by eliminating intraoperative injuries as there are no edges or sharp tools etc. In our case, we used the combination of URS and RIRS for the therapy of ureteral stent calcification, attaining clinical effectiveness based on effective risk reduction to the health care worker.
Transurethral flexible lithotripsy was previously performed using a conventional reusable flexible ureteroscope (ru-fURS). One in eight of the ru-fURS were discovered to be microbiologically contaminated, according to Legemate JD et al. [9]. The insufficient sterilization process of ru-fURS was documented by Ofstead CL et al. [10], who also discovered contamination in 100% of the sterilized ru-fURS, as well as microbial growth in 13% of them and hemoglobin in 63%. The ru-fURS had hemoglobin contamination levels above the threshold for a thoroughly cleaned gastrointestinal endoscopy. The use of a disposable flexible ureteroscope for ureterolithotripsy in HIV patients eliminates blood contact, one of the mechanisms by which HIV is spread, and also speeds up the sterilization procedure. This is also one of the key reasons why we use disposable ureteroscopes to treat such HIV diseases.
Conclusion
The disposable flexible ureteroscope is effective in the treatment of HIV-combined ureteral stent encrustation. Not only can it reduce the likelihood of HIV cross-contamination. When compared to ru-fURS, it may also be less cost-effective.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Agha RA Franchi T Sohrabi C Mathew G Kerwan A Thoma Aet al The SCARE 2020 Guideline: Updating Consensus Surgical C Ase R Eport (SCARE) Guidelines Int J Surg 2020 Dec 842262303318135810.1016/j.ijsu.2020.10.034 · doi ↗ · pubmed ↗
- 2Kawahara T Ito H Terao H Yoshida M Matsuzaki J Ureteral stent encrustation, incrustation, and coloring: morbidity related to indwelling times J Endourol 2012 Feb 262178822200791610.1089/end.2011.0385 · doi ↗ · pubmed ↗
- 3Acosta-Miranda AM Milner J Turk TM The FE Cal Double-J: a simplified approach in the management of encrusted and retained ureteral stents J Endourol 2009 Mar 233409151926547110.1089/end.2008.0214 · doi ↗ · pubmed ↗
- 4Arenas JL Shen JK Keheila M Abourbih SR Lee A Stokes P Ket al Kidney, ureter, and bladder (KUB): A novel grading system for encrusted ureteral stents Urology 2016 Nov 9751552742178010.1016/j.urology.2016.06.050 · doi ↗ · pubmed ↗
- 5Singh I Gupta NP Hemal AK Aron M Seth A Dogra PN Severely encrusted polyurethane ureteral stents: management and analysis of potential risk factors Urology 2001 Oct 584526311159753110.1016/s 0090-4295(01)01317-6 · doi ↗ · pubmed ↗
- 6Cicione A Stira J Tema G Franco A Ghezzo N Gravina Cet al Ureteral stent encrustation: evaluation of available scores as predictors of a complex surgery Minerva Urol Nephrol 2023 Jun 7533593653628639810.23736/S 2724-6051.22.04999-0 · doi ↗ · pubmed ↗
- 7Thangavelu M Abdallah MY Isola OJ Kotb A Management of encrusted ureteral stents: Two center experience Arch Ital Urol Androl 2022 Sep 269433053103616547510.4081/aiua.2022.3.305 · doi ↗ · pubmed ↗
- 8Torricelli FC Monga M Dall'Aqua V Marchini GS Vicentini FC Danilovic Aet al Percutaneous Nephrolithotomy in Immunocompromised Patients: Outcomes from a Matched Case-Control Study J Endourol 2016 Dec 3012132613312761511610.1089/end.2016.0496 · doi ↗ · pubmed ↗