The Usefulness of Intravascular Ultrasound and Optical Coherence Tomography in Patients Treated with Rotational Atherectomy: An Analysis Based on a Large National Registry
Wojciech Siłka, Michał Kuzemczak, Krzysztof Piotr Malinowski, Łukasz Kołtowski, Kinga Glądys, Mariola Kłak, Ewa Kowacka, Damian Grzegorek, Piotr Waciński, Michał Chyrchel, Miłosz Dziarmaga, Sylwia Iwańczyk, Miłosz Jaguszewski, Wojciech Wańha, Wojciech Wojakowski

TL;DR
Using imaging tools like IVUS or OCT during heart procedures with rotational atherectomy improves success rates in achieving proper blood flow.
Contribution
This study demonstrates that IVUS and OCT use during rotational atherectomy PCIs significantly increases the odds of successful revascularization.
Findings
RA-PCIs guided by IVUS or OCT achieved postprocedural TIMI 3 flow more frequently than angio-guided procedures.
IVUS and OCT use independently increased the odds of successful revascularization by 67% and 66%, respectively.
Abstract
Background: Intravascular ultrasound (IVUS) and optical coherence tomography (OCT) have been shown to improve the clinical outcomes of percutaneous coronary interventions (PCIs) in selected subsets of patients. Aim: The aim was to investigate whether the use of OCT or IVUS during a PCI with rotational atherectomy (RA-PCI) will increase the odds for successful revascularization, defined as thrombolysis in myocardial infarction (TIMI) 3 flow. Methods: Data were obtained from the national registry of PCIs (ORPKI) maintained by the Association of Cardiovascular Interventions (AISN) of the Polish Cardiac Society. The dataset includes PCIs spanning from January 2014 to December 2021. Results: A total of 6522 RA-PCIs were analyzed, out of which 708 (10.9%) were guided by IVUS and 86 (1.3%) by OCT. The postprocedural TIMI 3 flow was achieved significantly more often in RA-PCIs guided by…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
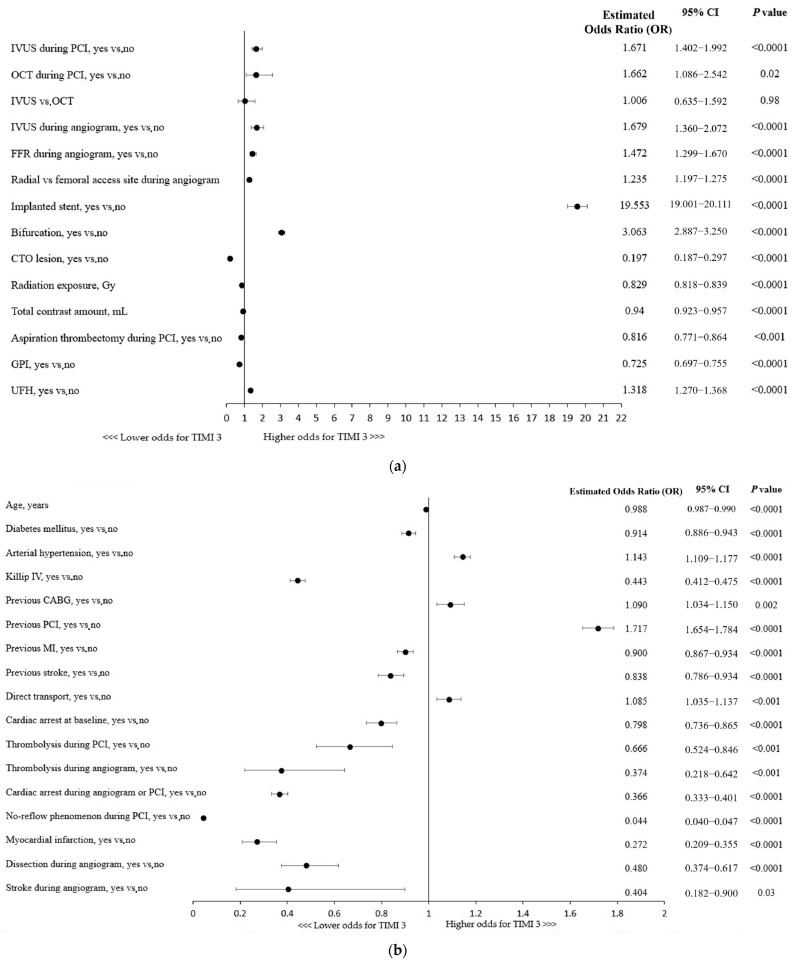 Figure 1
Figure 1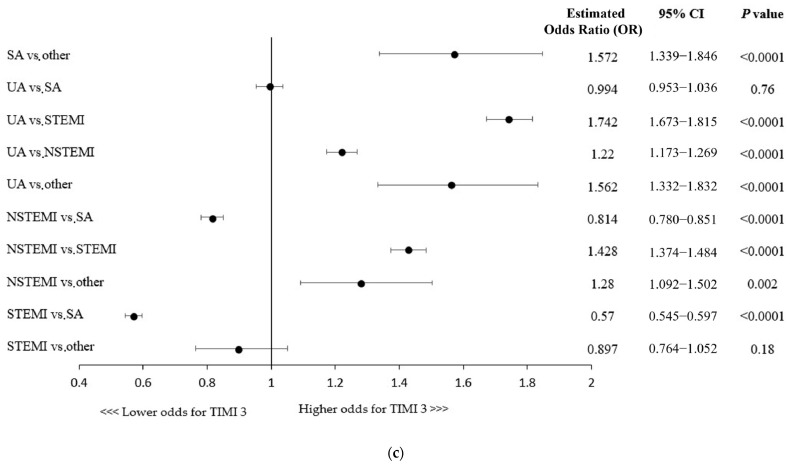 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoronary Interventions and Diagnostics · Cardiac Imaging and Diagnostics · Peripheral Artery Disease Management
1. Introduction
In contemporary clinical practice, the procedural success rate of percutaneous coronary interventions (PCIs) exceeds 95% [1]. However, the overall short- and long-term clinical outcomes depend on multiple factors, including but not limited to the patient’s condition at baseline, medical history, and operator experience [2,3,4,5]. Furthermore, dynamic advances in interventional technologies along with older and more comorbid patients translate into more complex and challenging cases to deal with in a cath lab, which were previously not eligible for PCI and were usually referred for coronary artery bypass graft surgery [6,7,8].
In order to achieve a sufficient lumen gain translating into short- and long-term postprocedural coronary patency, proper lesion preparation as well as optimal stent positioning and sizing play a crucial role. Therefore, intravascular imaging modalities, namely intravascular ultrasound (IVUS) and optical coherent tomography (OCT), have been introduced into the clinical arena. Importantly, despite clear benefits of intravascular imaging, particularly in more complex lesions, the use of the above-mentioned techniques varies, but it is still insufficient in Europe and North America [9]. According to the reported data from the National Inpatient Sample, intravascular imaging is used in less than 10% of all PCI procedures performed in the United States [10]. European data vary from country to country. Despite a significant increase in the use of these techniques, the British data indicate that intravascular imaging is used in 18% of cases, while in Poland in 2021, it was only 4.42% [11,12]. The rate of OCT use rarely exceeds 1 percent in all-comers patients [10,13].
The usefulness of IVUS and OCT among patients undergoing PCI of calcified coronary lesions has been demonstrated in several studies [14,15,16,17]. RA is an effective technique for calcified plaques, facilitating stent delivery and implantation. While IVUS- and OCT-guided PCIs have been demonstrated to yield improved clinical outcomes in complex lesions compared to angiography-guided procedures, the association between the use of IVUS/OCT in RAs and angiographic success (defined as postprocedural TIMI 3 flow) in real-world patients has not been extensively elucidated. Importantly, some available data indicate that intravascular imaging findings may predict coronary flow disturbances following RA [18]. Therefore, in the present study, we aimed to evaluate whether the use of intravascular imaging modalities is independently associated with the angiographic success rate of PCI with concomitant RA.
2. Methods
2.1. Materials and Study Design
The present study is a retrospective analysis of prospectively collected data obtained from the Polish National Registry of Percutaneous Coronary Interventions (ORPKI). The registry has already been described in previously published papers [19,20]. Data were collected from the registry for PCIs performed between January 2014 and December 2021. We extracted 6522 PCIs performed with concomitant rotational atherectomy. Out of them, 788 (12.08%) PCIs were guided by intravascular imaging, either IVUS (708, 89.8%) or OCT (86, 10.91%). The technical aspects of the procedure, such as the access site, catheter size, type of a coronary guidewire, intravascular imaging modality and burr diameter, were left at the operator’s discretion. Patients were referred for RA-PCI and intravascular imaging according to the current European Guidelines [21,22,23,24]. The protocol complied with the Declaration of Helsinki, and all the patients gave written informed consent prior the coronary procedure. Due to the retrospective nature and anonymization of the collected data, obtaining the consent of the Bioethics Committee was not required.
2.2. Statistical Analysis
Continuous variables are presented as means [standard deviation] and medians [first quartile; third quartile]. Normality was assessed via the Shapiro–Wilk test or Kolmogorov–Smirnov test with Lilliefors correction for variables with more than 2000 observations. The differences between the 2 groups were compared using the Student’s or Welch’s t-tests, depending on the equality of variance for normally distributed variables. In case of nonparametric data, the Mann–Whitney U test was introduced. Categorical variables were compared with Pearson’s chi-squared or Fisher’s exact test if 20% of the cells had an expected count of less than 5 (Monte Carlo simulation for Fisher’s test using tables of dimensions higher than 2 × 2). All demographic and clinical patients’ characteristics were adopted as potential factors associated with successful revascularization in univariable logistic regression models. Variables with a p-value < 0.2 were included in the final multivariable model constructed using minimization of the Akaike Information Criterion in order to find factors linked to the postprocedural TIMI 3 flow achievement. Statistical analysis was performed using R version 4.1.1 (R Foundation for Statistical Computing, Vienna, Austria, 2021) with the ‘rms’ package, version 6.2-0.
3. Results
A total of 6522 patients undergoing RA-PCI were analyzed in this study. Out of them, 788 (12.1%) underwent PCI with the guidance of intravascular imaging, either OCT (10.9%) or IVUS (89.8%). The postprocedural TIMI 3 flow was achieved significantly more often in RA-PCIs performed with intravascular imaging compared to angiography-guided procedures (98.7% vs. 96.6%, p < 0.0001).
3.1. General Characteristics at Baseline
The baseline characteristics are presented in Table 1 and Table 2. Patients who underwent RA-PCI guided by intravascular imaging modalities were younger (p = 0.03), less often males (p = 0.01), and less frequently suffered from diabetes mellitus (p = 0.005). However, arterial hypertension was significantly more prevalent among patients undergoing OCT compared to those who underwent RA-PCI without OCT (p = 0.001). Patients who were treated through RA-PCI with the guidance of intravascular imaging presented with acute coronary syndromes more often, including unstable angina, STEMI, or NSTEMI. Both comparison groups were similar according to the Killip classification at presentation.
3.2. Vascular Access, Coronary Angiography, and Procedural Indices
The femoral approach was significantly more common in patients undergoing IVUS- or OCT-guided procedures, whereas radial access was more frequently used for RA-PCIs without intravascular guidance (p = 0.01, Table 3). With regard to vascular access, no difference was found between groups in the analysis restricted to OCT-guided procedures. Isolated LMCA disease and MVD were found more frequently in patients undergoing imaging-guided RA-PCIs, whereas SVD was more prevalent in angiography-guided procedures. Furthermore, bivalirudin was more often used during PCIs guided using OCT or IVUS (Table 3), whereas P2Y_12_ inhibitors were used more frequently during PCI performed without IVUS, i.e., either with OCT or without any intravascular imaging guidance (Table 3).
Bifurcation PCI was more common in intravascular imaging-guided procedures compared to angiography-guided PCIs (p < 0.001, Table 4). Patients treated with an intravascular imaging-guided RA-PCI had a lower rate of TIMI 0/1 prior to the procedure (14.3% vs. 19.6%, p < 0.001) as compared to subjects undergoing RA-PCIs without intravascular imaging guidance. Contrast dye volumes and radiation exposure were higher in IVUS- or ICT-guided procedures (Table 4).
3.3. Periprocedural Complications
There were no significant differences between the study groups for periprocedural complications rates including death, myocardial infarction, no-flow/no-reflow/slow-flow phenomena, access site bleeding, cardiac arrest, allergic reactions, and coronary artery perforation (Table 5).
3.4. Predictors of a Technical Success
The use of any of the intravascular imaging modalities, IVUS (OR, 1.67; 95% CI: 1.40–1.99; p < 0.0001) or OCT (OR, 1.66; 95% CI: 1.09–2.54; p = 0.02), for the guidance of RA-PCI was independently associated with the technical success of the procedure, defined as TIMI 3 flow following the PCI (Figure 1a). No significant superiority of one technique over the other was found in a multivariable analysis. Importantly, the use of adjunctive IVUS during coronary angiography increased the chances of a successful RA-PCI by nearly 68% (Figure 1a). Considering other procedural indices, the radial access site, stent implantation, and fractional flow reserve (FFR) assessment during the angiogram were shown to be associated with technical success. Given the coronary lesion characteristics, bifurcation PCI was linked to higher odds for successful revascularization, whereas CTO (chronic total occlusion) lesions were found to be associated with a lower chance of achieving postprocedural TIMI 3 flow (Figure 1a). Furthermore, aspiration thrombectomy performed during the procedure as well as a higher usage of contrast dye and greater radiation exposure were associated with reduced odds for technical success (Figure 1a).
A more advanced age and the majority of concomitant comorbidities were associated with lower odds for postprocedural TIMI flow 3, except for hypertension being linked with 14% higher chances of successful revascularization (Figure 1b). Killip class IV (cardiogenic shock) or cardiac arrest at baseline were shown to be associated with decreased odds of postprocedural TIMI 3 flow, while direct transport, indicating the poor condition of a patient, was linked to higher odds of technical success (Figure 1b). Importantly, as shown in Figure 1c, the clinical presentation of coronary artery disease in patients undergoing RA-PCI had influence on the technical success rate (e.g., lower odds of achieving successful revascularization in NSTEMI/STEMI vs. SA patients).
Furthermore, all the periprocedural complications (MI, cardiac arrest, no-reflow phenomenon, coronary dissection, and stroke) and thrombolysis use were associated with lower chances of postprocedural TIMI 3 flow (Figure 1b).
4. Discussion
The present study supports the utilization of intravascular imaging to guide PCIs performed with concomitant rotational atherectomy. The notion is supported by the fact that postprocedural TIMI 3 flow was significantly more prevalent in IVUS- or OCT-guided RA-PCIs compared to angiography-guided procedures. Importantly, both the imaging modalities were independently associated with successful revascularization. Additionally, multivariable analysis revealed that among other factors linked to postprocedural TIMI 3 flow were younger age, bifurcation lesion, and prior revascularization attempts, whereas a worse clinical condition at baseline (Killip IV, presentation of acute coronary syndromes), greater procedural complexity (CTO lesion, more contrast and radiation used during PCI), and the incidence of periprocedural complications were associated with lower odds of the successful procedure.
Intravascular imaging modalities permit preprocedural lesion assessment, including an estimation of the true vessel size, based on which an optimal stent length and diameter can be chosen. With regard to RA-PCIs, this also allows for the selection of an optimal burr-to-artery ratio for appropriate calcified plaque modification without escalating the risk of periprocedural complications such as coronary artery dissection and perforation [25,26]. This might be particularly important not only for calcified de novo lesions, but also for RA-PCIs performed in stented segments [27]. The postprocedural assessment improves stent expansion and apposition as well as the detection of procedure-related complications. Although the utility of intravascular imaging depends on patients’ cohort characterization, the improvements of long-term clinical outcomes are generally well supported, particularly in severely calcified and complex lesions [14,16,28,29,30]. However, some studies encompassing both an all-comers cohort of patients and specific populations did not find significant improvements in the long-term endpoints (including MACE, target vessel revascularization, and definite stent thrombosis) following the introduction of intravascular imaging [31,32]. This is most likely driven by the lower complexity of PCIs (e.g., less severe calcifications), which reduces the potential benefits of intravascular imaging modalities. Since heavily calcified lesions are associated with stent underexpansion and the risk of in-stent restenosis, treatment of these particular lesions with the IVUS or OCT guidance yields most clinical benefits [33,34]. The armamentarium of calcium-modifying techniques is constantly expanding, and one can assume that the role of intravascular imaging modalities to guide these procedures will continue to increase in significance [35,36,37].
In the present analysis, the use of IVUS or OCT to guide RA-PCIs increased the odds for the postprocedural TIMI 3 flow by 67% and 66%, respectively. The technical success of the procedure defined as the achievement of TIMI 3 flow is a primary objective of all PCIs and has been shown to be an important predictor of improved clinical outcomes, including lower rates of in-hospital and long-term complications [38]. No difference between IVUS and OCT was found with regard to the achievement of successful revascularization. On the contrary, most of the published data comparing the efficacy of IVUS and OCT in the treatment of heavily calcified coronary arteries have shown the superiority of OCT over IVUS in terms of the periprocedural outcomes [16,17,38]. Kobayashi et al. reported greater stent expansion in OCT-guided RA-PCIs as compared to IVUS-guided RA-PCIs, concluding that RA with the guidance of OCT may be ideal for treating calcified coronary lesions [17]. Greater stent expansion following PCI guided with OCT was reported by other authors as well [16,39]. This is presumably driven by the higher resolution and more precise calcium visualization provided by OCT, as it detects calcium as signal-poor areas with well-delineated sharp borders [40]. On the contrary, IVUS does not permit the exact measurement of the calcium thickness given the fact that ultrasound signals are reflected by the calcium surface [41]. Therefore, OCT-guided RA-PCI enables more efficient calcium fracturing and facilitates optimal stent expansion. However, the immediate procedural success remains comparable, and the findings regarding long-term outcomes (the incidence of target lesion failure (TLR) and major adverse cardiovascular events (MACE)) remain inconsistent [16,17]. Therefore, the potential superiority of OCT in the treatment of severely calcified lesions warrants further studies.
Other findings of the present analysis are in line with the heretofore published data. In general, a younger age, prior revascularization attempts, and FFR are factors linked with better clinical outcomes, whereas a higher lesion complexity, worse patient clinical status at baseline, and procedural complications may have a detrimental influence on PCI outcomes [2,5,42,43].
5. Limitations
The present study has several limitations that need to be acknowledged when interpreting its results. First, this is a retrospective analysis with inherent limitations in the study design. It lacks randomization; therefore, one cannot exclude the influence of patient selection biases and unmeasured confounding factors on the final results. Second, the choice of intravascular imaging device was left entirely at the discretion of an operator, which could have also imposed a selection bias. Third, the number of patients undergoing OCT-guided RA-PCI was relatively small, which could have impacted the significance of the results. Fourth, due to the registry-based population cohort, certain data concerning RA-PCI were not available, including further follow-ups encompassing long-term outcomes of the RA-PCIs. Fifth, the data entered by operators were not double-checked for potential discrepancies with medical documentation. Lastly, in such a heterogenous population of patients (stable angina, unstable angina, NSTEMI, and STEMI), TIMI 3 flow might not be an equally adequate indicator of a successful procedure across the entire spectrum of patients, e.g., STEMI patients may have a large residual thrombus burden even following thrombectomy, which is a source of distal micro-embolization affecting postprocedural TIMI flow and long-term prognosis [44]. This is not observed in stable patients undergoing uncomplicated PCIs. The last issue is that the life span of the registry appears so long that technical changes could have modified the prevalence of using imaging modalities and even the clinical results.
6. Conclusions
In conclusion, the results of the present study indicate that intravascular imaging guidance (IVUS or OCT) during RA-PCIs is an independent predictor of a successful procedure (as defined by the achievement of postprocedural TIMI 3 flow); however, due to several limitations concerning the current analysis, the presented results should be considered as suggestive or supporting data. More studies are needed to evaluate the roles of intravascular imaging modalities in specific subsets of patients, including those treated with new emerging technologies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mukherjee D. Moliterno D.J. Effectiveness of PCI for non-acute coronary artery disease Lancet 200937387087210.1016/S 0140-6736(09)60522-519286067 · doi ↗ · pubmed ↗
- 2Brilakis E.S. Banerjee S. Karmpaliotis D. Lombardi W.L. Tsai T.T. Shunk K.A. Kennedy K.F. Spertus J.A. Holmes D.R. Grantham J.A. Procedural Outcomes of Chronic Total Occlusion Percutaneous Coronary Intervention: A Report from the NCDR (National Cardiovascular Data Registry)JACC Cardiovasc. Interv.2015824525310.1016/j.jcin.2014.08.01425700746 · doi ↗ · pubmed ↗
- 3Zein R. Seth M. Othman H. Rosman H.S. Lalonde T. Alaswad K. Menees D. Daher E. Mehta R.H. Gurm H.S. Association of Operator and Hospital Experience With Procedural Success Rates and Outcomes in Patients Undergoing Percutaneous Coronary Interventions for Chronic Total Occlusions: Insights From the Blue Cross Blue Shield of Michigan Cardiovascular Consortium Circ. Cardiovasc. Interv.202013 e 00886310.1161/CIRCINTERVENTIONS.119.00886332791954 · doi ↗ · pubmed ↗
- 4Hannan E.L. Wu C. Walford G. King S.B. Holmes D.R. Ambrose J.A. Sharma S. Katz S. Clark L.T. Jones R.H. Volume-Outcome Relationships for Percutaneous Coronary Interventions in the Stent Era Circulation 20051121171117910.1161/CIRCULATIONAHA.104.52845516103238 · doi ↗ · pubmed ↗
- 5Hannan E.L. Zhong Y. Jacobs A.K. Stamato N.J. Berger P.B. Walford G. Sharma S. Venditti F.J. King S.B. Patients With Chronic Total Occlusions Undergoing Percutaneous Coronary Interventions: Characteristics, Success, and Outcomes Circ. Cardiovasc. Interv.20169 e 00358610.1161/CIRCINTERVENTIONS.116.00358627162216 · doi ↗ · pubmed ↗
- 6Kirtane A.J. Doshi D. Leon M.B. Lasala J.M. Ohman E.M. O’Neill W.W. Shroff A. Cohen M.G. Palacios I.F. Beohar N. Treatment of Higher-Risk Patients With an Indication for Revascularization: Evolution Within the Field of Contemporary Percutaneous Coronary Intervention Circulation 201613442243110.1161/CIRCULATIONAHA.116.02206127482004 PMC 9117111 · doi ↗ · pubmed ↗
- 7Riley R.F. Henry T.D. Mahmud E. Kirtane A.J. Brilakis E.S. Goyal A. Grines C.L. Lombardi W.L. Maran A. Rab T. SCAI Position Statement on Optimal Percutaneous Coronary Interventional Therapy for Complex Coronary Artery Disease Catheter. Cardiovasc. Interv.20209634636210.1002/ccd.2899432406991 · doi ↗ · pubmed ↗
- 8Brinza C. Popa I.V. Basarab A. Crisan-Dabija R. Burlacu A. Procedural Success Prediction Scoring Systems Used in Percutaneous Coronary Interventions for Chronic Total Occlusions: A Systematic Evaluation Healthcare 20219103310.3390/healthcare 908103334442170 PMC 8393835 · doi ↗ · pubmed ↗