Radiation Oncologists’ Perspectives on Oligometastatic Prostate Cancer: A Survey from Korean Oligometastasis Working Group
Gyu Sang Yoo, Sunmin Park, Chai Hong Rim, Won Kyung Cho, Ah Ram Chang, Young Seok Kim, Yong Chan Ahn, Eui Kyu Chie

TL;DR
This study surveyed Korean radiation oncologists on their perspectives regarding oligometastatic prostate cancer and found strong agreement on using definitive radiation therapy for all metastatic lesions.
Contribution
The study provides insights into the consensus and variability in treatment approaches for oligometastatic prostate cancer among radiation oncologists in Korea.
Findings
Near perfect agreement was reached on applying definitive radiation therapy for all metastatic lesions in oligometastatic prostate cancer.
Stereotactic body radiation therapy is preferred for metastasis-directed RT by clinicians with higher clinical volume.
Agreement on optimal dose-fractionation for metastasis-directed RT has not yet been achieved.
Abstract
Background: Interest in the oligometastatic prostate cancer (OMPC) is increasing, and various clinical studies have reported the benefits of metastasis-directed radiation therapy (MDRT) in OMPC. However, the recognition regarding the adopted definitions, methodologies of assessment, and therapeutic approaches is diverse among radiation oncologists. This study aims to evaluate the level of agreement for issues in OMPC among radiation oncologists. Methods: We generated 15 key questions (KQs) for OMPC relevant to definition, diagnosis, local therapies, and endpoints. Additionally, three clinical scenarios representing synchronous metastatic prostate cancer (mPC) (case 1), metachronous mPC with visceral metastasis (case 2), and metachronous mPC with castration-resistance and history of polymetastasis (case 3) were developed. The 15 KQs were adapted according to each scenario and transformed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
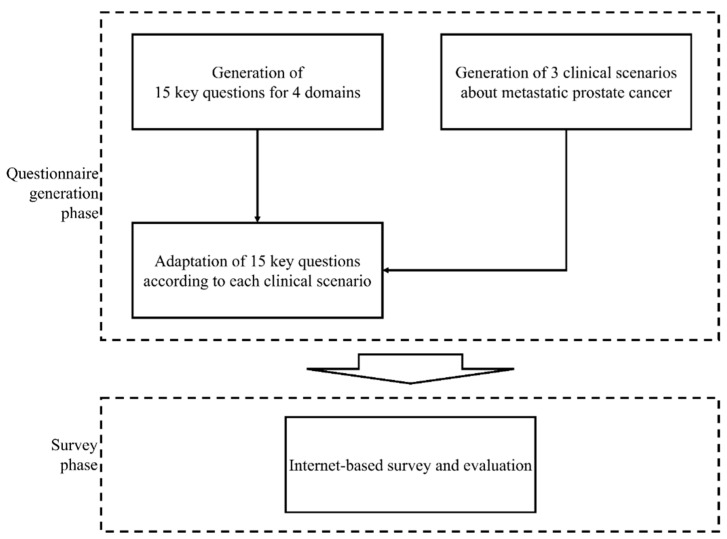 Figure 1
Figure 1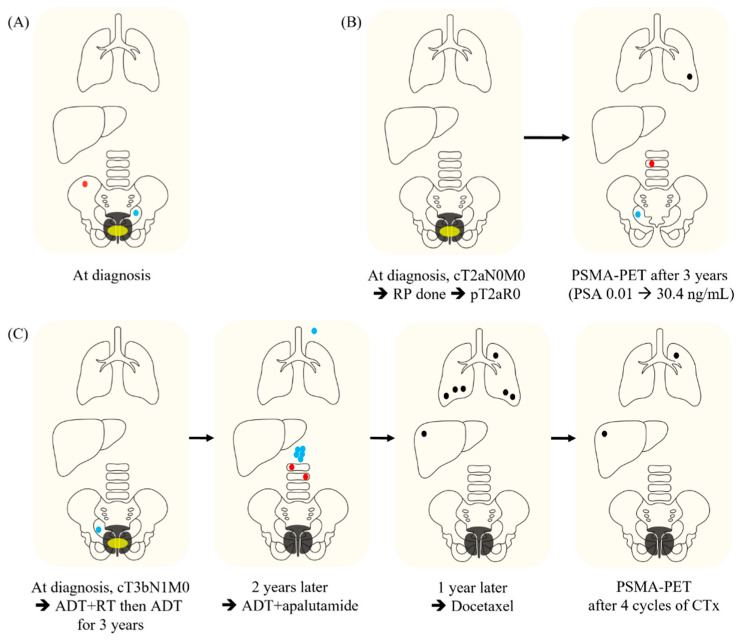 Figure 2
Figure 2- —Soonchunhyang University Research Fund
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsProstate Cancer Treatment and Research · Advanced Radiotherapy Techniques · Prostate Cancer Diagnosis and Treatment
1. Introduction
Oligometastatic disease (OMD) is a disease state in which a limited number of metastatic lesions exist while the disseminated metastatic growth is not fully developed [1]. This concept implies the possibility of the curation of OMD by applying ablative metastasis-directed local therapies (MDLTs). Since suggesting this concept, a number of studies have reported the benefit of MDLTs in improving oncological outcomes [2]. However, there is no consistency in the views of OMD among studies, including the definition and strategies for diagnosis, local treatment, and surveillance. To establish the consensus, the European Society for Radiotherapy and Oncology (ESTRO) conducted a survey study and reached a consensus on the definition of OMD [3]. However, this consensus does not consider primary tumor-specific aspects.
Prostate cancer (PC) is the second most common cancer and the fifth leading cause of cancer-related deaths among men worldwide [4]. Among men diagnosed with PC, approximately 20% have metastatic disease [5]. Interest in oligometastatic PC (OMPC) is increasing, and various clinical studies have reported the benefits of MDLT in OMPC. However, adopted definitions, methodologies of assessment, and therapeutic approaches vary among studies. Therefore, standardization of these issues according to the specific characteristics of OMPC is necessary for future investigation and clinical practice. For this requirement, a Korean Oligometastsais Working Group (K-OWG), affiliated with the Korean Cancer Association, was organized by radiation oncologists in the Republic of Korea to investigate and standardize various issues for OMPC. Herein, we raised OMPC-specific clinical issues that require consensus and performed a survey study to evaluate the level of agreement.
2. Materials and Methods
We raised five issues with OMPC including definition, diagnosis, radiation therapy (RT), and endpoint, and generated 15 relevant key questions (KQs) (Table 1). Additionally, three clinical scenarios regarding metastatic PC (mPC) were made for the survey. Case 1 is an mPC case with single pelvic lymph node (LN) and single right posterior iliac bone metastasis which were detected at the time of diagnosis for primary disease (synchronous mPC). Case 2 is an mPC case with a single lumbar spine, single pelvic LN, and single pulmonary metastasis at 3 years after radical prostatectomy for localized PC (de novo metachronous mPC). And Case 3 is a metastatic castration-resistant PC (CRPC) case with two lesions (pulmonary and hepatic metastases) showing induced oligoprogression according to the disease classification by ESTRO following definitive RT to the whole pelvis and androgen deprivation therapy (ADT) for localized high-risk PC and subsequent conversion to polymetastatic CRPC with six or more metastatic lesions [6]. The 15 KQs were adapted in the context of each clinical scenario and transformed into 23 multiple-choice questions with 6–9 per scenario. A questionnaire regarding the demographics of respondents was also developed with eight questions. The flow of the survey design is illustrated in Figure 1. Details of the scenarios are shown in Figure 2.
An anonymous survey was conducted using an online platform provided by SurveyMonkey^®^ (Palo Alto, CA, USA) in August 2022. The case scenarios and corresponding questionnaires were distributed to 80 certified radiation oncologists in the Republic of Korea who are members of the Genitourinary Division of the Korean Society of Radiation Oncology. The levels of agreement were defined as follows: answer options with 0.0–29.9%, 30–49.9%, 50–69.9%, 70–79.9%, 80–89.9%, and ≥90% agreements were considered as no, minimal, weak, moderate, strong, and near perfect agreement, respectively. Response rates were compared according to the average monthly numbers of new and OMD patients per year treated by responders using Fisher’s exact test.
3. Results
Of the 80 candidates, 45 (56.3%) voluntarily participated in the survey. Table 1 summarizes the demographic characteristics of responders. The results of the survey are shown in Supplementary Tables S1–S3. The characteristics of the cases and rates of response to the KQs according to the cases are presented in Table 1.
3.1. Definitions
There was a near perfect agreement in the response that the case was included in OMPC (93.0%) only for Case 1. All the responders who disagreed that Case 3 was included in the OMPC category replied that the previous history of polymetastatic disease could be the reason for excluding Case 3 in the OMPC category while only 28.6% selected CRPC status as the reason.
3.2. Diagnosis
For Case 1, only 60.5% agreed with the request of PSMA-PET to confirm the OMPC status. For Case 2, only 30.2% replied that the steep elevation of the prostate-specific antigen (PSA) could be the reason for excluding the case in the OMPC category.
3.3. Treatment
In Case 1, 93.0% of the responders replied that local treatment for primary PC was required and all chose definitive RT as the modality for primary PC. In Case 1, 97.7% of responders agreed with the application of MDLT, and all chose metastasis-directed RT (MDRT) for all metastatic lesions as MDLT while there was no moderate or higher level of agreement regarding the questions in Cases 2 and 3. To determine whether systemic therapy was required even if local control was achieved after MDRT, 79.1% and 87.2% responded that systemic therapy was required for Cases 1 and 3, respectively. No moderate or higher level of agreement has been reached regarding the dose-fractionation regimens for MDRT. However, there were significant differences in the response rates according to the clinical volume of new patients or OM patients treated by responders. For Case 2, the palliative RT dose to bone metastasis was chosen by responders with an average number of new patients per month < 30, significantly more than others (37.5% vs. 5.3%, p = 0.026; Supplementary Table S2). On the other hand, stereotactic body RT (SBRT) for lung metastasis was significantly preferred in responders with a clinical volume of the average numbers of OMD per year ≥ 10 (81.0% vs. 45.5%, p = 0.027; Supplementary Table S2). For Case 3, metastasis-directed SBRT was also significantly preferred in responders with a clinical volume of the average numbers of OMD per year ≥ 10 than others (80.0% vs. 42.1%, p = 0.022; Supplementary Table S3).
3.4. Endpoint
For the question about the parameter representing the failure of MDRT, responses in radiology and PSA level were chosen at 76.7% and 86.1%, respectively, for Case 1 while the rates of agreements were 81.4% and 72.1%, respectively, for Case 2 (Table 1). The rate of response that PSMA-PET needs to be applied to evaluate the complete remission after MDRT was 61.5% for Case 3.
4. Discussion
4.1. Definitions
In our study, only Case 1 was recognized as OMPC with a near perfect agreement. The definitions adopted by previous studies are heterogeneous in terms of number, location, and imaging modality for diagnosing OMPC. To provide a consensus, the ESTRO Guidelines Committee proposed consensus recommendations [7]. In the recommendation, 80% of the experts agreed to recommend MDRT for a maximum of five lesions [7]. In addition, 88% agreement was achieved in treating OMPC patients with LN, bone, and visceral metastasis. MDRT was not contraindicated by panelists; however, it was limited to selected cases based on clinical judgment [7].
While the majority of previous studies targeted hormone-sensitive mPC [8], oligometastatic CRPC has been investigated in only a limited number of studies [9,10]. The ESTRO recommendation also dealt with oligoprogressive CRPC without visceral metastasis [7]. In the Dutch multidisciplinary consensus meeting, 90% of the participants disagreed with the statement that OMPC following failure to ADT should preferably be treated by radical MDLT [11]. However, in our study, only 28.6% agreed that CRPC status was the reason for excluding Case 3 from the OMPC category. Therefore, this issue remains unclear. Rather than CRPC, a history of polymetastasis was recognized as the most important reason for excluding Case 3 from the OMPC category in our study. ESTRO and EORTC have suggested the concept of induced OMD with which patients have a history of polymetastasis before the diagnosis of OMD [6]. While previous studies have reported de novo OMD most frequently, induced OMD has rarely been reported [12]. The literature has not reported on induced OMPC, which might be a reason for the low awareness. Further studies are required to validate the concept of induced OMD in mPC.
4.2. Diagnosis
For the diagnosis of OMPC, the high performance of PSMA-PET has been proven in detecting metastasis of both hormone-sensitive PC and CRPC [13,14]. Based on this result, a consensus on the requirement of PSMA-PET for the confirmation of OMPC has been reached in previous studies [7,11]. However, in our study, there was no moderate or higher level of agreement regarding the requirement of PSMA-PET for Case 1 in which only conventional imaging was performed. Despite the excellent performance of PSMA-PET, its use was limited in the Republic of Korea because of limitations in government insurance coverage and this may impact the results of this study. However, the coverage was recently extended to include PSMA-PET, and the requirement for PSMA-PET is expected to increase in the Republic of Korea [15]. Therefore, re-evaluation of the consensus regarding PSMA-PET is necessary for the future.
There are no suggested criteria for the definition of OMPC, including the level or kinetics of the PSA [7]. In a Dutch multidisciplinary consensus meeting, more than 80% of panelists responded that PSA kinetics were not important for treatment decisions in synchronous OMPC, whereas more than 60% agreed that it was very important in metachronous OMPC [11]. In addition to PSA, several biomarkers including genetic markers, circulating tumor cells, and immunologic markers have been investigated showing impractical performance for predicting outcomes [16].
4.3. Treatment
In our study, near perfect agreements were achieved for the requirement of local treatment for primary tumors, MDRT for all metastatic lesions, and systemic treatment even if MDRT achieved local control of metastatic lesions in Case 1 which was the only one showing also near perfect agreement in the recognition as OMPC.
Based on previous trials demonstrating the benefits of RT for primary tumors, local RT for primary tumors for low-volume mPC is recommended in the guidelines [17,18]. The strong agreement on this issue for Case 1 may reflect the current recommendations. For metastatic lesions, protocols from relevant trials are commonly required to encompass whole lesions in the MDRT fields [19,20]. Our results showed a consistent agreement in Case 1. Despite no moderate or higher level of agreement that Cases 2 and 3 were included in the OMPC category, in the subgroups recognizing Cases 2 and 3 as OMPC, 86.7% and 94.4% agreed with the MDL(R)T for whole metastatic lesions, respectively. PSMA-PET can be utilized to select the RT target as emphasized in the ORIOLE trial [19].
Regarding MDRT for pelvic LN metastasis, whether to perform elective nodal RT (ENRT) or not also remains controversial [7]. In our study, the rate of agreement for ENRT for pelvic LN recurrence in Case 2 was only 23.3% (Supplementary Table S2). Previous studies have reported controversial results for the benefit of ENRT compared with local RT for pelvic LN recurrence from PC [21,22]. To address this issue, the PEACE V-STORM trial is ongoing [23]. In recommendations for RT in OMPC from an ESTRO consensus, ENRT with a boost on suspicious LNs was recommended as a preferred option but with only 60% agreement with divergent criteria for ENRT [7].
There was no moderate or higher level of agreement regarding radiation dose-fractionation schemes. In previous trials, the dose-fractionation scheme was heterogeneous among trials and anatomic sites [20]. In the ESTRO consensus recommendations, the preferred dose-fractionation regimens of SBRT for bone and LN were diverse; the results were 27–33 Gy in three fractions and 35–40 Gy in five fractions of which 30 Gy in three fractions and 35 Gy in five fractions were mostly preferred [7]. In our study, for responders with higher clinical volume for new patients or OMD patients, SBRT as MDRT was significantly favored. And RT with a palliative dose was significantly less preferred, implying that SBRT might be extended for OPMC as clinical experience is accumulated. Another controversial issue is the calculation of effective SBRT doses. Generally, SBRT with a biological effective dose (BED) of ≥100 Gy is recommended to improve local control [24]. To calculate BED, the radiation sensitivity of the primary tumor, which is reflected by α/β, should be considered [25,26]. PC has been recognized to have an α/β of 1.5–3.0 Gy, which is lower than that of other primary cancers, frequently with an α/β of 10 [27]. A previous study identified a BED greater than 100 Gy, calculated with an α/β ratio of 3 as a significant factor for local progression-free survival [26]. However, in the present study, an α/β ratio of 10 rather than 3 was preferred in the BED calculation to determine the SBRT dose for lung or liver metastasis. Similarly, a previous study argued that a higher α/β ratio should be used as the dose per fraction increases [28]. Therefore, this problem remains unsolved. Further studies are needed to determine the optimal dose of MDRT for OMPC.
4.4. Endpoint
In our study, moderate and strong agreements that the radiological response of the RT target could represent the outcome of MDRT were reached in Cases 1 and 2, respectively. For the PSA response, a strong agreement was achieved only in Case 1, and a moderate agreement was reached in Case 2. The emergence of new lesions was also considered as a parameter for the outcome of MDRT, with moderate agreement in cases 1 and 2. Because PSA is a specific marker for disease progression in PC, the response and kinetics of PSA after MDRT can be an important endpoint [7,29]. However, in the ESTRO consensus, the achievement of consensus failed regarding the definition of biochemical failure after MDRT for OMPC [7]. As the PSA can be a surrogate for disease progression even at the microscopic scale in PC, methodologies for the optimal use of the PSA after MDRT need to be established [11]. Our study showed only weak agreement regarding the use of PSMA-PET in evaluating an MDRT response. The role of PET in MDRT has been evaluated in PET-guided MDRT, particularly in the selection of target lesions [13,14,19]. However, for the evaluation of the RT response, the relevant role of PSMA-PET or choline-PET has been investigated in very few studies that showed a decrease in uptake values after RT [30]. This is also an important field of future research to build criteria for the treatment response evaluation of OMPC.
4.5. Limitations
This study had several limitations. This study does not represent the opinions of multidisciplinary experts, but only those of radiation oncologists in the Republic of Korea. Because the opinion of radiation oncologists could be influenced in the context of multidisciplinary discussion according to the cases, the cautious interpretation of the results in this study is required. The number of respondents was small and, especially, the rate of response was only 56.3%. This might not be enough to generalize the opinions of the radiation oncologists in the Republic of Korea. There was a limitation in increasing the rates of response because the survey should be based on the voluntary participation of responders. As the questionnaires were bound in the example cases, the agreements can be inconsistent for other possible clinical scenarios. The subsequent studies with more sufficient respondents and sample cases would be necessary to represent the opinion of radiation oncologists in the Republic of Korea and the diverse clinical situation regarding OMPC.
5. Conclusions
For the case recognized as OMPC, near perfect agreements were reached for the application of local therapies for primary and whole metastatic lesions. However, systemic therapy was also agreed to be applied very strongly even if local control was achieved after MDRT. While moderate or higher levels of agreement regarding the optimal dose-fractionation scheme for MDRT were not achieved, SBRT was favored by clinicians with a higher clinical volume for new patients or OMD patients. Further clinical studies on topics with an unreached consensus are necessary.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hellman S. Weichselbaum R.R. Oligometastases J. Clin. Oncol.19951381010.1200/JCO.1995.13.1.87799047 · doi ↗ · pubmed ↗
- 2Rim C.H. Cho W.K. Lee J.H. Kim Y.S. Suh Y.G. Kim K.H. Chie E.K. Ahn Y.C. Oligometastasis Working Group K.C.A. Role of Local Treatment for Oligometastasis: A Comparability-Based Meta-Analysis Cancer Res. Treat.20225495396910.4143/crt.2022.32935989655 PMC 9582460 · doi ↗ · pubmed ↗
- 3Lievens Y. Guckenberger M. Gomez D. Hoyer M. Iyengar P. Kindts I. Mendez Romero A. Nevens D. Palma D. Park C. Defining oligometastatic disease from a radiation oncology perspective: An ESTRO-ASTRO consensus document Radiother. Oncol.202014815716610.1016/j.radonc.2020.04.00332388150 · doi ↗ · pubmed ↗
- 4Sung H. Ferlay J. Siegel R.L. Laversanne M. Soerjomataram I. Jemal A. Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries CA Cancer J. Clin.20217120924910.3322/caac.2166033538338 · doi ↗ · pubmed ↗
- 5Rao A. Vapiwala N. Schaeffer E.M. Ryan C.J. Oligometastatic Prostate Cancer: A Shrinking Subset or an Opportunity for Cure?Am. Soc. Clin. Oncol. Educ. Book 20193930932010.1200/EDBK_23904131099652 · doi ↗ · pubmed ↗
- 6Guckenberger M. Lievens Y. Bouma A.B. Collette L. Dekker A. de Souza N.M. Dingemans A.C. Fournier B. Hurkmans C. Lecouvet F.E. Characterisation and classification of oligometastatic disease: A European Society for Radiotherapy and Oncology and European Organisation for Research and Treatment of Cancer consensus recommendation Lancet Oncol.202021 e 18e 2810.1016/S 1470-2045(19)30718-131908301 · doi ↗ · pubmed ↗
- 7Zilli T. Achard V. Dal Pra A. Schmidt-Hegemann N. Jereczek-Fossa B.A. Lancia A. Ingrosso G. Alongi F. Aluwini S. Arcangeli S. Recommendations for radiation therapy in oligometastatic prostate cancer: An ESTRO-ACROP Delphi consensus Radiother. Oncol.202217619920710.1016/j.radonc.2022.10.00536228761 · doi ↗ · pubmed ↗
- 8Connor M.J. Smith A. Miah S. Shah T.T. Winkler M. Khoo V. Ahmed H.U. Targeting Oligometastasis with Stereotactic Ablative Radiation Therapy or Surgery in Metastatic Hormone-sensitive Prostate Cancer: A Systematic Review of Prospective Clinical Trials Eur. Urol. Oncol.2020358259310.1016/j.euo.2020.07.00432891600 · doi ↗ · pubmed ↗