Mutational profile of primary clear cell renal cell carcinoma predicts recurrence and potential candidacy for adjuvant immune checkpoint inhibition
Panagiotis J. Vlachostergios, Maria Papathanassiou, Maria Anagnostou, Eleni Thodou, Ioannis Tamposis, Lampros Mitrakas, Ioannis Zachos, Maria Ioannou, George K. Koukoulis, Maria Samara, Vassilios Tzortzis, Athanasia Pavlopoulou, Panagiotis J. Vlachostergios

TL;DR
This study shows that specific genetic mutations in kidney cancer can predict cancer recurrence and guide treatment with immune checkpoint inhibitors.
Contribution
The study identifies non-VHL mutations as prognostic markers for recurrence and potential response to adjuvant immunotherapy in clear cell renal cell carcinoma.
Findings
Non-VHL mutations in ccRCC tumors are associated with larger tumor size and higher stage.
Patients with non-VHL mutations had a higher risk of recurrence compared to those with VHL-only or no mutations.
Non-VHL mutations in TCGA ccRCC patients correlated with significantly shorter disease-free survival.
Abstract
Background: The risk of recurrence after nephrectomy for primary clear cell renal cell carcinoma (ccRCC) is estimated in daily practice solely based on clinical criteria. The aim of this study was to assess the prognostic relevance of common somatic mutations with respect to tumor aggressiveness and outcomes of ccRCC patients after definitive treatment. Methods: Primary tumors from 37 patients with ccRCC who underwent radical nephrectomy were analyzed for presence of somatic mutations using a 15-gene targeted next-generation sequencing (NGS) panel. Associations to histopathologic characteristics and outcomes were investigated in the study cohort (n=37) and validated in The Cancer Genome Atlas (TCGA) ccRCC cohort (n=451). Results: VHL was the most frequently mutated gene (51%), followed by PBRM1 (27%), BAP1 (13%), SETD2 (13%), KDM5C (5%), ATM (5%), MTOR (5%), and PTEN (3%). One-third…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
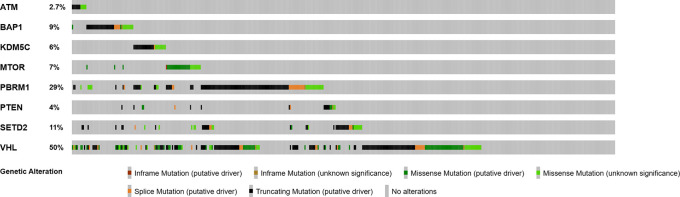 Figure 1
Figure 1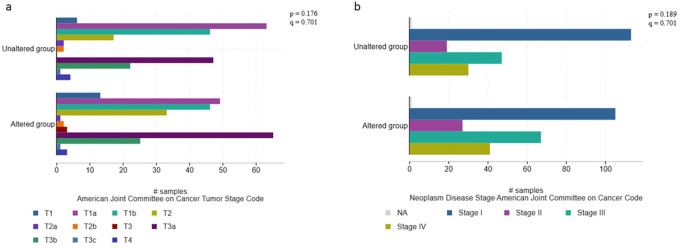 Figure 2
Figure 2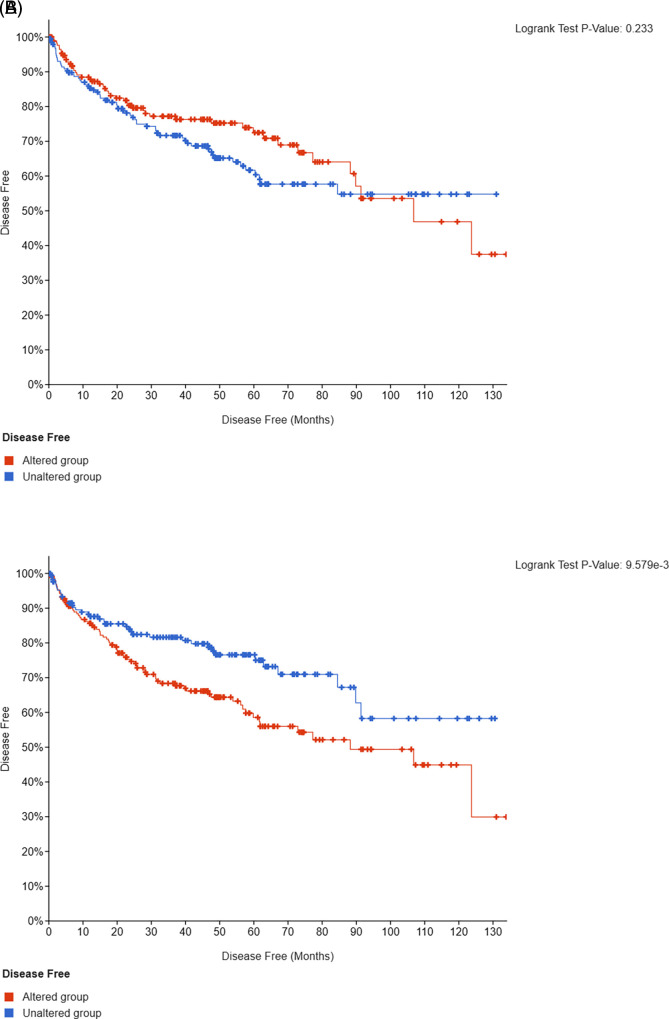 Figure 3
Figure 3| Characteristic | Number (%) |
|---|---|
| Age | |
| median (range) | 63 (42-87) |
| Sex | |
| males | 28 (75) |
| Tumor diameter (cm) | |
| median (range) | 5.6 (1.6 – 15) |
| Pathological T stage | |
| T1 | 21 (57) |
| T2 | 6 (16) |
| T3 | 10 (27) |
| ISUP grade | |
| 2 | 13 (35) |
| 3 | 15 (41) |
| 4 | 8 (24) |
| Vascular invasion | 5 (14) |
| Necrosis | 13 (35) |
| Sarcomatoid differentiation | 0 |
| AJCC TNM stage | |
| I | 21 (57) |
| II | 6 (16) |
| III | 10 (27) |
| Gene | Frequency, n (%) |
|---|---|
|
| 19 (51) |
|
| 10 (27) |
|
| 5 (13) |
|
| 5 (13) |
|
| 2 (5) |
|
| 2 (5) |
|
| 2 (5) |
|
| 1 (3) |
| Variable | Mutated genes | P value | |
|---|---|---|---|
| None or
| Non-
| ||
| Pathological T stage | 0.02 | ||
| T1/T2 | 17 (89) | 8 (44) | |
| T3 | 2 (11) | 10 (56) | |
| AJCC TNM stage | 0.02 | ||
| I/II | 17 (89) | 8 (44) | |
| III | 2 (11) | 10 (56) | |
| ISUP grade | 0.93 | ||
| 2/3 | 15 (79) | 14 (78) | |
| 4 | 4 (21) | 4 (22) | |
| Necrosis | 0.64 | ||
| no | 13 (68) | 11 (61) | |
| yes | 6 (32) | 7 (39) | |
| Vascular invasion | 0.58 | ||
| no | 17 (89) | 15 (83) | |
| yes | 2 (11) | 3 (17) | |
| Outcome | Mutated genes | P value | |
|---|---|---|---|
| None or
| Non-
| ||
| Recurrence | 0.06 | ||
| no | 19 (100) | 15 (83) | |
| yes | 0 (0) | 3 (17) | |
- —European Union and Greek national funds, Operational Program Competitiveness, Entrepreneurship and Innovation, under RESEARCH—CREATE—INNOVATE
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRenal cell carcinoma treatment · Renal and related cancers · Cancer Genomics and Diagnostics
Introduction
Renal cell carcinoma (RCC) is a heterogenous group of kidney cancers originating from the nephron. ^ 1 ^ Renal cell carcinoma ranks among the ten most frequently diagnosed malignancies worldwide, with an estimated 400.000 new diagnoses and more than 170.000 deaths annually. ^ 2 ^ ^,^ ^ 3 ^ Clear cell RCC (ccRCC) is the most common RCC subtype, accounting for about 70-75% of cases and has a distinct molecular profile. ^ 1 ^ ^,^ ^ 4 ^
Localized ccRCC is treated with surgical resection, either partial or radical nephrectomy. Nevertheless, one-third of these patients experience recurrence. ^ 5 ^ So far, ccRCC recurrence, disease progression and mortality are being predicted using clinicopathological criteria. ^ 6 ^ While various recurrence models have been proposed, they only marginally outperformed standard staging. ^ 7 ^ Further, they demonstrate statistically significant variability in their predictive ability over time, rendering implementation into clinical practice and clinical trial design challenging. ^ 7 ^
Immune checkpoint inhibition with the use of pembrolizumab, a monoclonal antibody against programmed death-1 (PD-1), is approved as adjuvant therapy for patients with resected ccRCC who have a high risk of recurrence. ^ 8 ^ This was based on results of a phase III randomized double-blind study comparing pembrolizumab with placebo, which demonstrated a significant improvement in disease-free survival (DFS). ^ 9 ^ Patient selection criteria for a high risk of recurrence included tumor stage II with nuclear grade 4 or sarcomatoid differentiation, tumor stage III or higher, regional lymph-node metastasis, or stage M1 without evidence of disease after combined nephrectomy and metastasectomy either concurrently or within a year from primary tumor resection. ^ 9 ^
What currently remains an unmet need is the ability to predict which patients with ccRCC will relapse using a single or composite molecular biomarker that would be more directly related with tumor biology.
In this ongoing prospective study, we examined the mutational profile of patients with non-metastatic ccRCC who underwent nephrectomy, followed by observation or adjuvant immunotherapy with pembrolizumab depending on established clinical and histopathological criteria. We studied associations of mutated genes with high-risk features and assessed the prognostic relevance of somatic mutations with regard to DFS after nephrectomy with or without adjuvant immunotherapy.
Methods
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board and Ethics Committee of Faculty of Medicine, University of Thessaly (3214/29.07.2016) on 29 July 2016.
Study design
This was a prospective single-center cohort study of patients with a diagnosis of ccRCC who underwent radical nephrectomy followed by observation or adjuvant immune checkpoint inhibition with pembrolizumab at the University Hospital of Larissa between December 2020 and February 2023. Eligible subjects included patients of ≥18 years of age, with histologically confirmed non-metastatic ccRCC, without prior systemic therapy for RCC. Patients were eligible if they had an intermediate-to-high or high risk of recurrence based on histopathological features including pT2 with grade 4 or sarcomatoid differentiation, pT3 or pT4 with any grade, or any pT and grade with presence of positive lymph nodes (N+). Subjects unable to provide consent, those with low risk of recurrence or subjects receiving steroids at a daily dose above 10mg of prednisone for an active autoimmune or other condition were excluded from the study. The primary endpoint of the study was the percentage of patients without disease recurrence.
Data collection
Fresh frozen tissue samples were acquired from patients. Tumor tissue was acquired after surgical resection, cut in 5 mg cubes and stored in stabilization solution (RNA later, Thermo Fisher Scientific) at -80 ^o^C freezer, after written informed consent was obtained. DNA extraction and quantification was performed from 5 mg of fresh-frozen tissue. Library preparation was conducted with the use of DNA AmpliSeq for Ion Torrent, with an input of 40 ng DNA per sample. Sample libraries were quantified with the use of Qubit (Thermo-Fisher Scientific) and real-time polymerase chain reaction (PCR), then sequenced on Ion Torrent S5 sequencer, using the Oncomine Kidney panel (Thermo-Fisher Scientific). Library amplification was conducted using the Library PLUS for Ion Torrent kit (Thermo Fisher). Library amplification included enzyme activation at 99 ^o^C for 2 minutes, 16 cycles of denaturation at 99 ^o^C for 15 seconds and annealing and extension steps at 60 ^o^C for 4 minutes and a final hold step at 10 ^o^C. The commercially available Oncomine ^TM^ Kidney Panel (Thermo Fisher Scientific) provided the primer pairs used for library preparation. qPCR was conducted using the Ion Universal Library Quantitation Kit (Thermo Fisher Scientific). qPCR steps include an initial step of incubation at 50 ^o^C for 2 minutes, a polymerase activation step at 95 ^o^C for 2 minutes, 40 cycles of 95 ^o^C for 15 seconds and 60 ^o^C for 1 minute and a final hold step at 10 ^o^C. ^ 10 ^
Clinicopathological characteristics recorded for the analysis included patient age, sex, ISUP grade, tumor diameter, T-stage, presence of vascular invasion, presence of sarcomatoid differentiation, presence of necrosis, AJCC stage, and emergence of recurrent disease during follow up. Nephrectomy surgical specimens were reviewed by two independent pathologists from our institution.
A publicly available database, cBioportal for Cancer Genomics (accessed on 24 May 2023), was used to query DNA sequencing data for mutations in a prospective multicenter cohort from The Cancer Genome Atlas (TCGA) including 451 patients with ccRCC (accessed on 24 May 2023).
Data analysis
The following genes were analyzed for presence of somatic mutations: ATM, BAP1, KDM5C, MET, MTOR, NF2, PBRM1, PIK3CA, PTEN, SETD2, SMARCB1, TP53, TSC1, TSC2, and VHL. Variant calling was performed using the Ion Reporter Software (Thermo-Fisher Scientific). The Pearson’s Chi squared test was used to determine whether there was a statistically significant difference in clinicopathological characteristics and emergence of recurrence between subgroups of patients with distinct mutational profiles (unmutated or VHL-only mutated versus other gene mutations). Time-to-event outcomes (DFS) were estimated using the Kaplan-Meier method. Multiple hypothesis test correction was applied using the Benjamini–Hochberg method. All tests were two-sided, and p and q values ≤0.05 were considered statistically significant. The IBM SPSS v.22 software was used for the analysis.
Results
Mutations in non-
VHL genes are associated with more aggressive disease
We first assessed the frequency of mutations in primary ccRCC tumors. In the discovery cohort (n=37), patients’ clinical and histopathological characteristics are described in Table 1. VHL was the most frequently mutated gene (n=19; 51%), followed by PBRM1 (n=10; 27%), BAP1 (n=5; 13%), SETD2 (n=5; 13%), KDM5C (n=2, 5%), ATM (n=2, 5%), MTOR (n=2, 5%), and PTEN (n=1, 3%) ( Table 2). Variant types per gene are listed in the data file. ^ 23 ^ 11 patients (30%) did not have any somatic mutations within the 15-gene targeted panel.
Tumors harboring no mutations at all or only VHL mutations (n=19, 51%) were associated with smaller size (pT1-2 n=17, 89%) and earlier stage (I/II n=17; 89%), whereas presence of any other gene mutations in various combinations with or without VHL was enriched in larger (pT3, n=8; 44%; p=0.02) and more advanced tumors (III, n=8; 44%; p=0.02) ( Table 3). There was also a trend towards higher frequency of ISUP grade, vascular invasion, and necrosis in these tumors ( Table 3).
In the validation TCGA cohort (n=451), similar mutations frequencies were noted, including VHL in 50% of patients/samples, PBRRM1 in 29%, SETD2 in 11%, BAP1 in 9%, MTOR in 7%, KDM5C in 6%, PTEN in 4%, and ATM in 2.7%, respectively ( Figure 1). Larger and higher stage tumors, particularly T3a, T3b, and stage III tended to have a higher frequency of non-VHL mutations (p=0.282; q=0.437) ( Figure 2).
Frequency of mutated genes in primary ccRCC tumors (validation cohort, n=451).
Associations between histopathological characteristics and mutational profile (validation cohort, n=451).
Mutations in non-
VHL genes predict recurrence
No recurrences were noted in patients with unmutated tumors or VHL-only mutations whereas three patients (17%) with other somatic mutations relapsed (p=0.06) ( Table 4). Another three patients received and completed adjuvant PD-1 inhibition with pembrolizumab until present, none of whom recurred despite the presence of PBRM1 and SETD2 mutations in 2/3 and 1/3, respectively. Presence of somatic mutations in PBRM1, BAP1, SETD2, KDM5C, ATM, MTOR, or PTEN genes in 451 TCGA ccRCC patients was associated with a significantly shorter DFS compared to those with unaltered tumors (p<0.001; q=0.01) ( Figure 3).
Kaplan-Meier analysis of DFS in patients with unmutated or VHL-only versus non- VHL mutated tumors (validation cohort, n=451).
Discussion
This ongoing prospective study examined the mutational profile of patients with ccRCC on primary tumors after nephrectomy followed by observation or adjuvant immunotherapy with pembrolizumab and assessed for associations of mutated genes with high-risk features and DFS. In this preliminary analysis of the first 37 patients, non- VHL mutations, including mutations in PBRM1, SETD2, BAP1, KDM5C, MTOR, PTEN, or ATM genes in a targeted 15-gene NGS panel were significantly associated with more aggressive histopathological characteristics including larger size, and higher stage. Presence of mutations in any of those genes as opposed to completely unmutated or VHL-only mutated tumors was also associated with higher ISUP grade, necrosis, sarcomatoid differentiation, vascular invasion and predicted recurrence. In ccRCC tumors from TCGA, non- VHL mutations in the same genes were also associated with high-risk features and predicted a significantly shorter DFS compared to VHL-only mutations or complete absence thereof.
The tumor suppressor VHL is the most frequently mutated gene in ccRCC and is a major player in renal cell carcinogenesis. However, VHL mutations alone are insufficient to drive disease progression. ^ 11 ^ Mounting evidence has revealed an emerging role of other genes, heavily involved in chromatin rearrangement and epigenetic DNA modifications, including PBRM1, SETD2, BAP1, and KDM5C in ccRCC progression. ^ 12 ^ ^,^ ^ 13 ^ Inactivating mutations or/and low expression of these genes in primary renal tumors have been associated with poor outcomes. ^ 14 ^ ^–^ ^ 20 ^
Due to the retrospective nature of these studies and lack of reproducibility, particularly across immunohistochemical assessments ^ 21 ^ ^,^ ^ 22 ^ in an era when observation was the only available modality post-operatively even in high-risk patients, there has been a paucity of data to support testing of these genes as a molecular tool to assist in selection of patients who might benefit from adjuvant therapy.
Our ongoing prospective study addresses this gap by demonstrating that patients who had either no mutation or mutations in the most frequently altered gene, VHL, were more likely to have smaller tumors and experienced a more benign course without relapse, compared to those patients with tumors that harbored mutations in other genes, including PBRM1, BAP1, SETD2, KDM5C, ATM, MTOR, or PTEN. Thus, this study suggests that patients with mutations in these high-risk genes might be more suitable candidates and should be prioritized for post-operative immunotherapy.
Our study was limited by small size and relatively short follow-up of patients. Nevertheless, presence of an early “signal” of high-risk genes in this preliminary report will be further studied in additional patients being accrued as part of this ongoing prospective study.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Shuch B Amin A Armstrong AJ : Under-standing pathologic variants of renal cell carcinoma: distilling therapeutic opportunities from biologic complexity. Eur. Urol. 2015;67:85–97. 10.1016/j.eururo.2014.04.029 24857407 · doi ↗ · pubmed ↗
- 2Hsieh JJ Purdue MP Signoretti S : Renal cell carcinoma. Nat. Rev. Dis. Primers. 2017;3:17009. 10.1038/nrdp.2017.9 28276433 PMC 5936048 · doi ↗ · pubmed ↗
- 3Bray F Ferlay J Soerjomataram I : Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018;68:394–424. 10.3322/caac.21492 30207593 · doi ↗ · pubmed ↗
- 4Cancer Genome Atlas Research Network: Comprehensive molecular characterization of clear cell renal cell carcinoma. Nature. 2013;499:43–49. 10.1038/nature 12222 23792563 PMC 3771322 · doi ↗ · pubmed ↗
- 5Li Y Lih TM Dhanasekaran SM : Clinical Proteomic Tumor Analysis Consor-tium. Histopathologic and proteogenomic heterogeneity reveals features of clear cell renal cell carcinoma aggressiveness. Cancer Cell. 2023;41:139–163.e 17. 10.1016/j.ccell.2022.12.001 36563681 PMC 9839644 · doi ↗ · pubmed ↗
- 6Leibovich BC Blute ML Cheville JC : Prediction of progression after radical nephrectomy for patients with clear cell renal cell carcinoma: a stratification tool for prospective clinical trials. Cancer. 2003;97:1663–1671. 10.1002/cncr.11234 12655523 · doi ↗ · pubmed ↗
- 7Correa AF Jegede O Haas NB : Predicting Renal Cancer Recurrence: Defining Limitations of Existing Prognostic Models With Prospective Trial-Based Validation. J. Clin. Oncol. 2019;37:2062–2071. 10.1200/JCO.19.00107 31216227 PMC 7085167 · doi ↗ · pubmed ↗
- 8Cosso F Roviello G Nesi G : Adjuvant Therapy for Renal Cell Carcinoma: Hype or Hope? Int. J. Mol. Sci. 2023;24:4243. 10.3390/ijms 24044243 36835654 PMC 9959913 · doi ↗ · pubmed ↗