Transdermal bisoprolol for prevention of postoperative atrial fibrillation: A systematic review and meta‐analysis
Andrew G. Kim, Sandeep Banga, Qi Xuan Ang, Lalitsiri Atti, Harith Ghnaima, Saif AlAttal, Preeti Banga, Matthew D. Wilcox

TL;DR
A review finds that transdermal bisoprolol is effective in reducing postoperative atrial fibrillation, possibly better than the oral version.
Contribution
First systematic review and meta-analysis on transdermal bisoprolol for postoperative atrial fibrillation prevention.
Findings
Transdermal bisoprolol reduced postoperative atrial fibrillation risk by 57% compared to control groups.
The analysis included three studies with 551 patients, showing no heterogeneity among results.
The findings suggest transdermal bisoprolol may be more effective than oral formulations.
Abstract
The transdermal patch of bisoprolol available in Japan has been reported to demonstrate superior efficacy in preventing postoperative atrial fibrillation, possibly surpassing its oral counterpart. However, there has been no systematic review and meta‐analysis assessing the efficacy of transdermal bisoprolol. A comprehensive systematic literature search was conducted on PubMed, Embase, and Cochrane to identify all relevant studies assessing the efficacy of transdermal bisoprolol in preventing postoperative atrial fibrillation. The search covered studies from inception up to December 4, 2023. For data analysis, Review Manager (RevMan) 5.4 software was employed, using a random‐effects model to calculate risk ratios (RR) and 95% confidence intervals (CI). Three studies, comprising a total of 551 patients (transdermal bisoprolol 228 and control 323), were included. There was a decreased…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
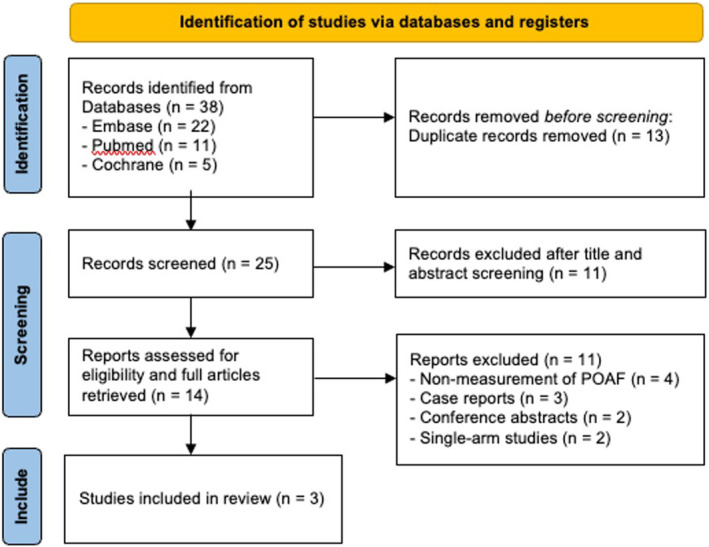 FIGURE 1
FIGURE 1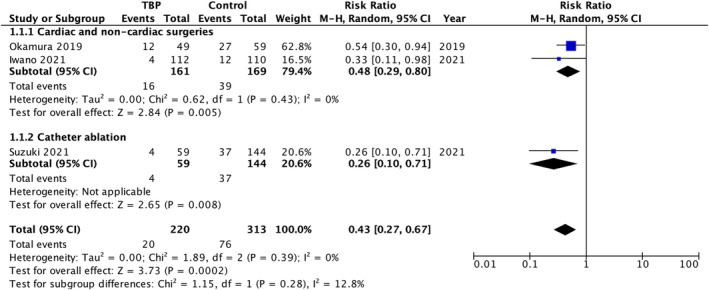 FIGURE 2
FIGURE 2| Author | Okamura et al. (2019) | Iwano et al. (2021) | Suzuki et al. (2021) |
|---|---|---|---|
| Country | Tokyo, Japan | Okayama, Japan | Akashi, Japan |
| Study design | Single‐center retrospective study | Multicenter randomized controlled study | Single‐center retrospective study |
| Study period | April 2016 to February 2018 | November 2014 to February 2019 | January 2018 to June 2019 |
| Sample size, N | Total 108; TBP 49 and control (OBF) 59 |
Total 240; TBP 120 and control 120 at randomization (intention‐to‐treat analysis) Total 222; TBP 112 and control 110 | Total 203; TBP 59 and control 144 |
| Population | Patients who underwent cardiac and/or thoracic aortic surgery | Patients aged ≥60 years, with hypertension and a Revised Cardiac Risk Index (RCRI) score ≥2, scheduled for noncardiac surgery, and not receiving beta‐blockers. Patients with chronic AF were excluded. | Patients with paroxysmal atrial fibrillation who underwent their first ablation and had a left ventricular ejection fraction of ≥35% |
| Intervention | TBP 4 mg (equivalent to OBF 2.5 mg) or lower daily from POD 1 | TBP 4 mg daily or lower from 7 days before surgery until POD 7 | TBP 4 mg or dose adjusted |
| Comparison | No TBP; OBF 2.5 mg or lower daily from POD 1 | No TBP; no beta‐blockade was given to the comparison group | No TBP; oral antiarrhythmics were substituted, including OBF (32.6%), carvedilol (15.3%), atenolol (1.4%), verapamil (1.4%), bepridil (2.8%), flecainide (11.1%), and amiodarone (0.7%) |
| Outcome | Postoperative AF | Postoperative AF | Postprocedural early recurrences of AF or AT |
| Definition of outcome | New onset of postoperative AF lasting >30 seconds recorded using a telemetry system throughout hospitalization | Onset of AF that occurred within 30 days after surgery | Any episode of AF or AT lasting ≥30 seconds and occurring within 90 days of AF ablation |
| Methods of AF detection | Telemetry system throughout hospitalization with average postoperative 23 ± 14 days | ECG monitoring for several days after surgery. After the ECG monitoring was discontinued, arrhythmia was detected on the basis of the patient's symptoms and vital signs | ECG monitor, 12‐lead ECG, Holter ECG, or CIED |
| Adjusted confounders |
– Age ( – Preoperative medication: ACEI ( – Type of surgery: isolated valve surgery ( |
Toda et al. (2020) (MAMACARI trial) – Age, gender, BMI, RCRI score, high‐risk procedure, history of IHD, history of heart failure, history of cerebrovascular disease, renal failure, preoperative insulin use, ASA class 2, ASA class 3, hypertension, DM, dyslipidemia, smoker, paroxysmal AF, PAD, obstructive lung disease, and asthma – Previous treatment: PCI, CABG, and pacemaker – Systolic blood pressure, diastolic blood pressure, pulse rate, LVDF, LA diameter, E/e’, and eGFR – Medication: CCB, ACEI, ARB, diuretics, antiplatelet therapy, oral anticoagulants, and statin – Vital capacity, FEV1 – Surgical specialty: general, thoracic, vascular, neurosurgery, orthopedic, otolaryngology, urology, and others – Anesthesia: inhalation anesthesia and duration of surgery |
– Age ( – Medications on discharge: verapamil ( – Ablation procedure: CTI ablation ( |
| Covariates in model | Hypertension (TBP 76%, control 56%, |
– Medications on discharge: beta‐blocker (TBP 100%, control 49.3%, – Ablation procedure: cryoballoon (TBP 50.8%, control 66%, |
| Okamura et al. (2019) | Iwano et al. (2021), | Suzuki et al. (2021) | ||||
|---|---|---|---|---|---|---|
| TBP ( | Control ( | TBP ( | Control ( | TBP ( | Control ( | |
| Age (years) | 69.2 ± 14.5 | 68.4 ± 14.0 | 76 (67–85) | 76 (66–86) | 66.9 ± 12.7 | 66.7 ± 10.0 |
| Male gender | 25 (51%) | 25 (42%) | 92 (77%) | 92 (77%) | 38 (64.4%) | 108 (75%) |
| BMI (kg/m2) | 22.3 ± 3.7 | 23.2 ± 4.7 | 22.8 (20.6–24.7) | 22.8 (21.2–25.3) | 23.5 ± 3.6 | 23.9 ± 3.6 |
| Hypertension | 37 (76%) | 33 (56%) | 120 (100%) | 120 (100%) | 30 (50.8%) | 71 (49.3%) |
| DM | 4 (8%) | 10 (17%) | 53 (44%) | 62 (52%) | 9 (15.3%) | 22 (15.3%) |
| Heart failure | 17 (35%) | 23 (39%) | 34 (28%) | 29 (24%) | 2 (3.4%) | 4 (2.8%) |
| Dyslipidemia | 9 (18%) | 13 (22%) | 62 (52%) | 62 (52%) | 20 (33.9%) | 35 (24.3%) |
| IHD | 9 (18%) | 10 (17%) | 73 (61%) | 65 (54%) | 6 (10.2%) | 8 (5.6%) |
| Stroke | 6 (12%) | 5 (8%) | 37 (31%) | 36 (30%) | 4 (6.8%) | 9 (6.3%) |
| LVEF (%) | 61.4 ± 12.3 | 62.0 ± 13.9 | 66 (61–69) | 66 (62–69) | 66.0 ± 6.5 | 65.9 ± 6.9 |
| LA diameter (mm) | 37 ± 9 | 40 ± 7 | 37 (34–40) | 36 (32–40) | 36.4 ± 4.6 | 35.6 ± 5.3 |
| BNP (pg/mL) | 330 ± 607 | 282 ± 491 | – | – | 99.2 ± 19.7 | 64.9 ± 8.1 |
| Beta‐blocker | 13 (27%) | 9 (15%) | 0 (0%) | 0 (0%) | 59 (100%) | 71 (49.3%) |
| ACEI or ARB | 18 (36%) | 26 (45%) | 71 (67%) | 82 (68%) | 20 (33.9%) | 48 (33.3%) |
| CCB | 21 (43%) | 24 (41%) | 71 (59%) | 70 (58%) | – | – |
| Statin | 10 (20%) | 17 (29%) | 44 (37%) | 49 (41%) | 21 (35.6%) | 31 (21.5%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtrial Fibrillation Management and Outcomes · Cardiovascular Syncope and Autonomic Disorders · Cardiac pacing and defibrillation studies
INTRODUCTION
1
Postoperative atrial fibrillation (POAF) is observed in 5%–60% of postsurgical patients, with a higher incidence following cardiac and valve surgeries.1 Although many cases spontaneously convert to normal sinus rhythm,2 POAF is linked to adverse outcomes, such as stroke and death.3
Beta‐blockers have been employed to prevent POAF in both cardiac4 and noncardiac surgeries.5 Bisoprolol, a selective beta‐1 receptor blocker without intrinsic sympathomimetic activity, not only controls heart rate but also exhibits antiarrhythmic effects in atrial fibrillation, potentially through the suppression of sympathetic activity.6 Recent advances in electrophysiology, such as cardioneuroablation, underscore the role of steady autonomic nervous system regulation in suppressing atrial fibrillation.7 In light of these findings, hypothesizing that maintaining a more stable serum beta‐blocker concentration would offer superior POAF prevention seems plausible.
Transdermal bisoprolol patch (TBP) (Bisono^®^ Tape; Toa Eiyo, Tokyo, Japan) offers advantages over oral bisoprolol fumarate (OBF) by ensuring a steady serum concentration. This could be beneficial in POAF prevention, considering that minimizing autonomic variability through autonomic denervation reduces atrial fibrillation recurrences.7 Hypothetically, TBP may outperform OBF in preventing POAF by potentially minimizing autonomic variability by maintaining steadier serum concentrations. Indeed, Okamura et al. (2019)8 demonstrated the superiority of the transdermal formula over the oral formula in preventing POAF. In this context, we conducted a comprehensive literature review on the efficacy of TBP.
METHODS
2
Search strategy
2.1
An extensive search of the literature was conducted using the databases PubMed, Embase, and Cochrane, gathering all studies available from their start dates up to December 4, 2023. The search terms used included “bisoprolol,” “transdermal,” and “atrial fibrillation,” in various word forms, applied across all texts.
Study selection
2.2
Two reviewers (AGK and SB) independently conducted a thorough evaluation of the study articles. We included all studies that evaluated the efficacy of TBP in preventing POAF with a comparison group. Case reports or abstracts with insufficient data were excluded, along with single‐arm studies that only evaluated the efficacy of TBP. Five studies8, 9, 10, 11, 12 from Japan evaluating the effect of TBP in POAF were retrieved. Three studies8, 9, 10 were included in the review. Two studies11, 12 only included patients who received TBP, thereby being removed from the comparative analysis. The meta‐analysis was performed following the Preferred Reporting Items for Systematic Reviews and Meta‐Analysis (PRISMA) guidelines (Figure 1).
Preferred reporting items for systematic reviews and meta‐analysis (PRISMA) flowchart.
Statistical analysis
2.3
The pooled analysis was conducted using Review Manager (RevMan) 5.4 software, applying a random‐effects model for the calculation of risk ratios (RRs) and 95% confidence intervals (CIs). Statistical significance was determined by an overall p‐value below .05. The I ^2^ test was used to evaluate heterogeneity.
RESULTS
3
Study characteristics
3.1
The analysis comprised one multicenter randomized controlled study9 and two single‐center retrospective studies,8, 10 with a total of 551 patients—228 in the TBP arm and 323 in the control arm. Heterogeneity existed among the three studies in terms of the type of surgery, control group, and outcome measures. Detailed characteristics of the included studies and patients are listed in Tables 1, 2.
Cardiac and noncardiac surgeries
3.1.1
Okamura et al. (2019)8 conducted a single‐center retrospective study in Tokyo, Japan, from April 2016 to February 2018, involving 108 participants undergoing cardiac/thoracic aortic surgery. The study compared TBP 4 mg or lower from POD 1 to discharge to no TBP (OBF 2.5 mg or lower), with 49 participants in the TBP arm and 59 in the control (OBF) arm. The outcome measured was the new onset of AF (>30s).
Iwano et al. (2021),9 a subanalysis of the MAMACARI trial with baseline characteristics stated in Toda et al. (2020),13 is a multicenter randomized controlled study conducted in Okayama, Japan, from November 2014 to February 2019. It included 240 participants aged ≥60 with hypertension and a revised cardiac risk index score ≥2 scheduled for noncardiac surgery. Patients receiving beta‐blockers and patients with chronic AF were excluded. The study compared TBP 4 mg or lower from 7 days pre‐surgery to POD 7 to no TBP, with 120 participants in each arm. The measured outcome was AF onset within 30 days postsurgery.
Catheter ablation
3.1.2
Suzuki et al. (2021)10 is a single‐center retrospective study in Akashi, Japan, from January 2018 to June 2019, involving 203 participants with paroxysmal AF undergoing their first ablation, with LVEF ≥35%. The study compared TBP 4 mg or dose adjusted to no TBP immediately after AF ablation for 3 months, with 59 participants in the TBP arm and 144 in the control arm. The control arm could have received either OBF or other antiarrhythmics instead of TBP, including OBF (32.6%), carvedilol (15.3%), atenolol (1.4%), verapamil (1.4%), bepridil (2.8%), flecainide (11.1%), and amiodarone (0.7%). The measured outcome was early recurrences of atrial arrhythmias within 90 days post‐AF ablation (blanking period).
Outcomes
3.2
Cardiac and noncardiac surgeries
3.2.1
The combined analysis by Okamura et al. (2019),8 which evaluated postoperative patients who underwent cardiac or thoracic aortic surgery, and Iwano et al. (2021),9 which assessed those undergoing noncardiac surgeries, showed a decreased risk of POAF in the TBP group; risk ratio 0.48, 95% CI 0.29–0.80, p = .005, I ^2^ = 0%.
Catheter ablation
3.2.2
Suzuki et al. (2021),10 which evaluated patients who underwent catheter‐guided AF ablation procedures, revealed a decreased risk of atrial arrhythmias in the TBP group; risk ratio 0.26, 95% CI 0.10–0.71, p = .008.
Overall
3.2.3
The pooled analysis of both subgroups revealed a decreased risk of either postoperative atrial fibrillation or atrial tachyarrhythmias in patients treated with transdermal bisoprolol, risk ratio 0.43, 95% CI 0.27–0.67, p = .0002, I ^2^ = 0%. Despite heterogeneity of the three studies in terms of type of surgery/procedure and comparison group, statistical heterogeneity of the outcome between the TBP arm and the control arms was 0%. In the test for subgroup differences between cardiac and noncardiac surgeries versus catheter ablation, the heterogeneity (I ^2^) was 12.8%, indicating low variability among the subgroups. Each study yielded statistically and clinically significant results, as illustrated in Figure 2.
Forest plot of outcomes. CI, confidence interval; M‐H, Mantel‐Haenszel; TBP, transdermal bisoprolol patch.
DISCUSSION
4
Postoperative atrial fibrillation (POAF) poses a clinical challenge, affecting a notable percentage of postsurgical patients, especially after cardiac and valve surgeries.1 While many cases spontaneously revert to normal sinus rhythm, the association between POAF and adverse outcomes, including stroke and death, underscores the need for effective prevention strategies.2, 3
Bisoprolol, a beta‐1 receptor blocker without intrinsic sympathomimetic activity, is commonly used for ventricular rate control in atrial fibrillation. It also demonstrates an antiarrhythmic effect, likely achieved by suppressing sympathetic activity, particularly in maintaining sinus rhythm for patients with a history of atrial fibrillation mediated by sympathetic tone.6
Evidence suggests that minimizing autonomic variability through vagal and sympathetic denervation is associated with a reduction in atrial fibrillation recurrences.7 This insight guides our exploration of the potential benefits of maintaining a more stable blood bisoprolol concentration through transdermal administration. Our study supports the advantages of transdermal bisoprolol patch (TBP) in preventing POAF.
Study limitations
4.1
Our study's interpretability is hindered by the variability in surgical procedures, control groups, and outcome measures across the included studies. This variability affects the consistency of the findings and their applicability to different surgical contexts.
The study included both cardiac and noncardiac surgeries, as reported in studies by Okamura et al. (2019)8 and Iwano et al. (2021),9 as well as AF ablation procedures, according to Suzuki et al. (2021).10 This mix of different interventions may influence the generalizability of the results, despite the consistency observed.
Okamura et al. (2019)8 conducted a direct comparison between the TBP group and the OBF group. In contrast, Suzuki et al. (2021)10 compared the TBP group with a control group, which included a significant portion of patients receiving alternative oral antiarrhythmics. These included OBF (32.6%), carvedilol (15.3%), atenolol (1.4%), verapamil (1.4%), bepridil (2.8%), flecainide (11.1%), and amiodarone (0.7%).
Iwano et al. (2021),9 however, did not compare TBP with OBF but instead evaluated TBP against no beta‐blocker treatments. Despite these discrepancies, all included studies consistently demonstrated the efficacy of TBP in preventing POAF. Both Okamura et al. (2019)8 and Suzuki et al. (2021)10 suggested TBP's superiority over OBF in this context.
CONCLUSION
5
In conclusion, our study supports the potential of transdermal bisoprolol as a superior preventive measure against postoperative atrial fibrillation (POAF). The sustained suppression of sympathetic tone through the transdermal patch may introduce a clinically relevant avenue for exploration. Future randomized clinical trials may elucidate the nuanced efficacy of transdermal bisoprolol over oral bisoprolol in diverse surgical and procedural contexts.
CONFLICT OF INTEREST STATEMENT
The authors have no competing interests to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Danelich IM , Lose JM , Wright SS , Asirvatham SJ , Ballinger BA , Larson DW , et al. Practical management of postoperative atrial fibrillation after noncardiac surgery. J Am Coll Surg. 2014;219:831–841. 10.1016/j.jamcollsurg.2014.02.038 25127508 · doi ↗ · pubmed ↗
- 2Lee JK , Klein GJ , Krahn AD , Yee R , Zarnke K , Simpson C , et al. Rate‐control versus conversion strategy in postoperative atrial fibrillation: a prospective, randomized pilot study. Am Heart J. 2000;140:871–877. 10.1067/mhj.2000.111104 11099990 · doi ↗ · pubmed ↗
- 3Conen D , Alonso‐Coello P , Douketis J , Chan MTV , Kurz A , Sigamani A , et al. Risk of stroke and other adverse outcomes in patients with perioperative atrial fibrillation 1 year after non‐cardiac surgery. Eur Heart J. 2019;41:645–651. 10.1093/eurheartj/ehz 431 31237939 · doi ↗ · pubmed ↗
- 4Crystal E , Garfinkle MS , Connolly S , Ginger T , Sleik K , Yusuf S . Interventions for preventing post‐operative atrial fibrillation in patients undergoing heart surgery. Cochrane Database Syst Rev. 2004;8:CD 003611. 10.1002/14651858.CD 003611.pub 2 15495059 · doi ↗ · pubmed ↗
- 5Khanna AK , Naylor DF Jr , Naylor AJ , Mascha EJ , You J , Reville EM , et al. Early resumption of β blockers is associated with decreased atrial fibrillation after noncardiothoracic and nonvascular surgery. Anesthesiology. 2018;129:1101–1110. 10.1097/ALN.0000000000002457 30300157 · doi ↗ · pubmed ↗
- 6Ishiguro H , Ikeda T , Abe A , et al. Antiarrhythmic effect of bisoprolol, a highly Selective.BETA.1‐blocker, in patients with paroxysmal atrial fibrillation. Int Heart J. 2008;49:281–293. 10.1536/ihj.49.281 18612186 · doi ↗ · pubmed ↗
- 7Pachon‐M JC , Pachon‐M EI , Pachon CTC , Santillana‐P TG , Lobo TJ , Pachon‐M JC , et al. Long‐term evaluation of the vagal denervation by Cardioneuroablation using Holter and heart rate variability. Circ Arrhythm Electrophysiol. 2020;13:13. 10.1161/CIRCEP.120.008703 33198486 · doi ↗ · pubmed ↗
- 8Okamura H , Arakawa M , Miyagawa A , Adachi H . Incidence of postoperative atrial fibrillation in transdermal β‐blocker patch users is lower than that in oral β‐blocker users after cardiac and/or thoracic aortic surgery. Gen Thorac Cardiovasc Surg. 2019;67:1007–1013. 10.1007/s 11748-019-01131-5 31049816 · doi ↗ · pubmed ↗