Successful closure of large mucosal defect with novel anchor-pronged clip after gastric endoscopic submucosal dissection
Kenichiro Okimoto, Tomoaki Matsumura, Keisuke Matsusaka, Yuki Ohta, Takashi Taida, Jun Kato, Naoya Kato

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Fig. 1
Fig. 1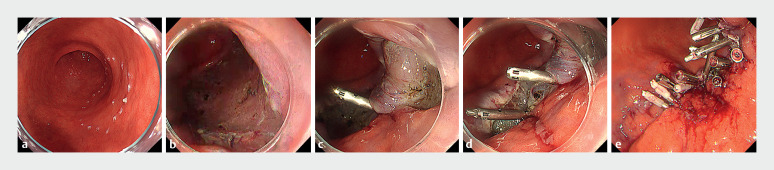 Fig. 2
Fig. 2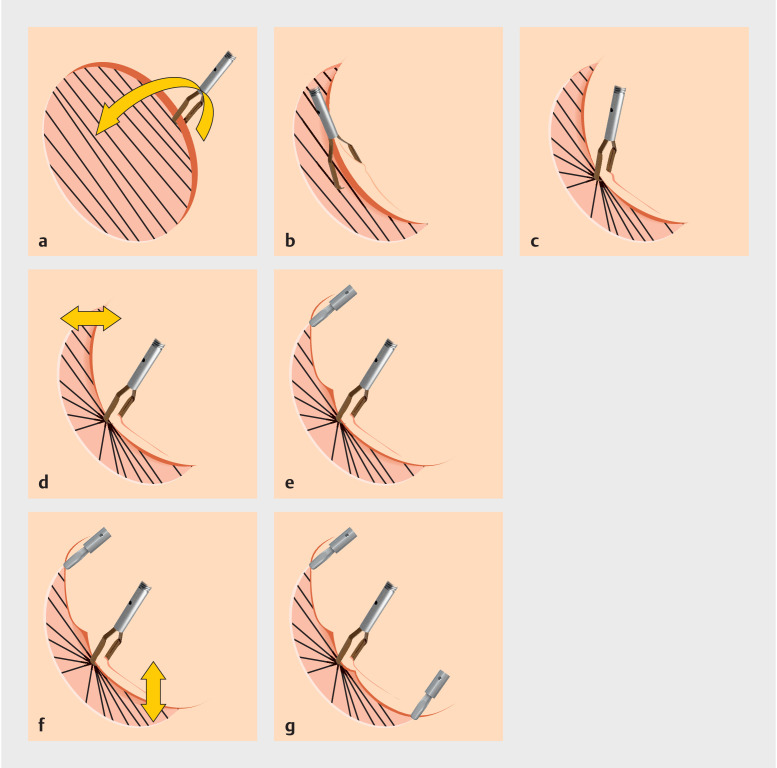 Fig. 3
Fig. 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Esophageal and GI Pathology · Metastasis and carcinoma case studies
Delayed bleeding after gastric endoscopic submucosal dissection (ESD) is a major complication 1 that sometimes leads to shock, and mucosal defect closure to prevent delayed bleeding was reported 2 . However, the thickness of the gastric mucosa and proper muscle layer makes suturing difficult 3 . A recent study reported the closure of an intermediate-size mucosal defect post-gastric ESD with a novel anchor-pronged clip (MANTIS Clip; Boston Scientific, Marlborough, Massachusetts, USA) ( Fig. 1 ) 4 . Here, we present the successful closure of large mucosal defect with a MANTIS Clip after gastric ESD ( Video 1 ).
Novel anchor-pronged clip. The clip is re-openable and rotational.
Successful closure of large mucosal defect after gastric endoscopic submucosal dissection.Video 1
The case involved a woman in her 90s on continued low-dose aspirin therapy. A 40-mm lesion was identified on the posterior wall of the lower body in the stomach ( Fig. 2 a ). ESD was performed for en bloc resection, resulting in a mucosal defect approximately 60 mm in size ( Fig. 2 b ). The pathological finding was intramucosal carcinoma with a negative horizontal and vertical margin. The defect was closed using a similar approach as a mucosa-submucosa closure after colorectal ESD 5 . First, one side of the mucosa was grasped with the MANTIS Clip. The clip was then moved to the opposite muscle layer, opened once, and after sufficient air aspiration, the clip was used to grasp the muscle layer ( Fig. 2 c, d ; Fig. 3 a, c ). After sufficient shrinkage of the mucosal defect, complete closure without obvious dead space was achieved by adding mucosa-mucosa and mucosa-muscle closure with normal clips (16-mm Sure Clip; Micro-Tech Co., Ltd, Nanjing, China) or EZ Clip (Olympus Medical Systems, Tokyo, Japan) ( Fig. 2 e ; Fig. 3 d–g ). In total, three MANTIS Clips, six Sure Clips, and four EZ Clips were applied. The closure time was 14 minutes. The patient was discharged according to schedule without experiencing delayed bleeding.
Closure of a large mucosal defect after gastric endoscopic submucosal dissection (ESD). a The lesion was diagnosed endoscopically as a 40-mm diameter IIc. Markings were placed around it. b The mucosal defect after ESD. The diameter was estimated to be around 60 mm. c The mucosal defect was shrunk with a MANTIS Clip (mucosa-muscle closure was performed). d The mucosal defect was further shrunk using the same method. e Complete closure was achieved by adding mucosa-mucosa and mucosa-muscle closure with normal clips.
Closing method schema. The black diagonal lines represent the course of muscle fibers. a–c When the mucosal defect is large after ESD, grasp one side of the mucosa with a MANTIS Clip. Then move the clip to the opposite muscle layer, open the clip once, and after sufficient air aspiration, grasp the muscle layer. d, e When the mucosal defect is small, mucosa-mucosa closure after sufficient air aspiration is performed with a normal clip. f, g When the mucosal defect is intermediate in size, mucosa-muscle closure after sufficient air aspiration is performed with a normal clip.
The novel anchor-pronged clip was thought to be useful in closing even large mucosal defects after gastric ESD.
Endoscopy_UCTN_Code_TTT_1AO_2AO
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hatta W Tsuji Y Yoshio T Prediction model of bleeding after endoscopic submucosal dissection for early gastric cancer: BEST-J score Gut 20217047648410.1136/gutjnl-2019-31992632499390 PMC 7873424 · doi ↗ · pubmed ↗
- 2Maekawa S Nomura R Murase T Complete closure of artificial gastric ulcer after endoscopic submucosal dissection by combined use of a single over-the-scope clip and through-the-scope clips (with videos)Surg Endosc 20152950050425052125 10.1007/s 00464-014-3725-1PMC 4293458 · doi ↗ · pubmed ↗
- 3Choi KD Jung HY Lee GH Application of metal hemoclips for closure of endoscopic mucosal resection-induced ulcers of the stomach to prevent delayed bleeding Surg Endosc 2008221882188610.1007/s 00464-008-9743-018270775 · doi ↗ · pubmed ↗
- 4Inada T Sumida Y Homma H Novel clip method for endoscopic submucosal dissection defect closure reducing submucosal dead space in antithrombotic gastric patients Endoscopy 202456 E 45E 4610.1055/a-2223-447538232769 PMC 10794086 · doi ↗ · pubmed ↗
- 5Nishizawa T Banno S Kinoshita S Feasibility of endoscopic mucosa-submucosa clip closure method (with video)Endosc Int Open 20186 E 1070 E 107430105296 10.1055/a-0630-0566 PMC 6086683 · doi ↗ · pubmed ↗