Striving for Improved Prognostication in Adults With Repaired Aortic Coarctation: Utility of the H2FPEF Score
Matthias Greutmann

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1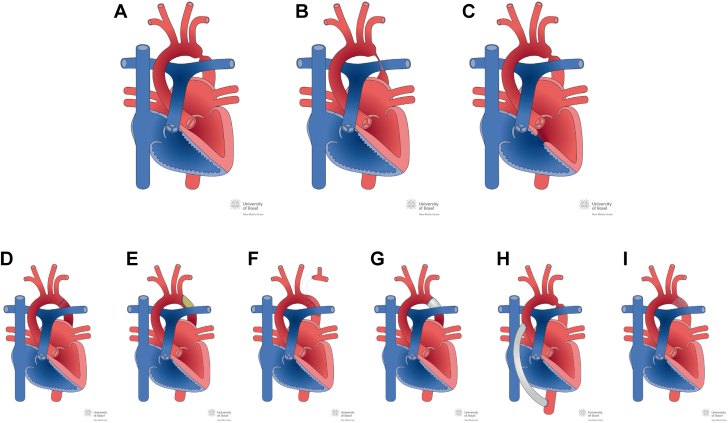 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Heart Disease Studies · Cardiac Valve Diseases and Treatments · Cardiac Structural Anomalies and Repair
Adults with repaired aortic coarctation
Aortic coarctation is a common congenital heart defect, accounting for about 10% of patients followed up at specialized centers.1 While aortic coarctation, on first glance, may appear to be a “simple” lesion, outcome studies have shown that it bears a substantially increased mortality risk, with heart failure being the predominant cause of attrition in affected young and middle-aged adults, accounting for 31% of deaths in one study.2
Aortic coarctation encompasses a spectrum of anatomical variants with a variety of associated lesions, most commonly bicuspid aortic valves, present in about two-thirds of all patients (Figures 1A to 1C). Furthermore, numerous surgical and interventional repair techniques have evolved over previous decades. These are tailored to the patient’s individual defect anatomy but also to evolving knowledge about long-term complications and progress in medical technology (Figures 1D to 1I). All these different repair techniques harbor the potential for long-term complications, generic to the defect or being specific to the type of individual repair technique. Thus, for affected patients, regular follow-up at specialized centers is mandatory.Figure 1Anatomic Variants of Aortic Coarctation and Different Repair ProceduresIllustration taken from http://www.chd-diagrams.com. (A to C) Variants of aortic coarctation and associated lesions: (A) focal type of aortic coarctation with concomitant bicuspid aortic valve; (B) aortic coarctation, tubular type; (C) aortic coarctation associated with muscular septal defects. (D-I) Types of repair operation: (D) repair by resection and end-to-end anastomosis; (E) repair by patch aortoplasty; (F) repair by subclavian flap aortoplasty; (G) repair by interposition graft; (H) repair by extra-anatomic ascendens-descendens graft; (I) repair by endovascular stent placement.
Heart failure in adult congenital heart disease: a major challenge ahead of us
Heart failure is the leading cause of death among adult survivors with congenital heart defects.2 With the evolution of novel adult patient cohorts, its overall prevalence and clinical importance will likely increase over upcoming decades.3 While the cohort of adults with end-stage heart failure is expected to increase substantially in the near future, only a minority of these patients will have access to timely heart transplantation.4 Identifying patients at risk, in order to optimize their therapy, with the aim of delaying the need for heart transplantation is therefore of paramount importance.
While there is no doubt that risk-stratification has to occur on a lesion-specific basis, even within a single disease entity, such as aortic coarctation, the spectrum of underlying anatomical variants and various types of repair techniques hamper the generalizability of risk scores based on these variables. More generic risk scores, such as the H_2_FPEF score, take into account demographic and hemodynamic characteristics and may overcome some of the variabilities among individual patients.
In their study in this issue of JACC: Advances, Egbe et al5 impressively confirms the high risk of serious cardiovascular complications among adults with repaired aortic coarctation. Within their cohort, over a median follow-up of 8 years, cardiovascular complications occurred in 14% of all patients, with heart failure being the predominant clinical problem occurring in 9% of the entire study cohort. They also found that a higher H_2_FPEF score was independently associated with an increased risk of cardiovascular events, particularly in patients with isolated aortic coarctation. Furthermore, in patients with follow-up of more than 5 years, the authors were able to demonstrate that an increase in the H_2_FPEF score during follow-up was independently associated with an increased risk of cardiovascular events. As expected, the H_2_FPEF score correlated with N-terminal pro-B-type natriuretic peptide levels (available in about 40% of patients) but interestingly not with left ventricular ejection fraction, nor with systolic pressure gradients across the coarctation site or with arm-leg pressure gradients.
Outlook and future needs
Retrospective single-center studies are important in the field of adult congenital heart disease. Such studies allow the analysis of data with high granularity from single institutions with standardized follow-up protocols. However, such retrospective studies typically can generate hypotheses only, as results are subject to numerous biases by nature of data and analysis. Thus, it is important that hypotheses generated by retrospective studies be validated in prospective studies or registries, ideally in a multicenter setting.
There is no doubt that the validity of the H_2_FPEF score merits further assessments in such a prospective study. This will allow to identify whether the H_2_FPEF score and its changes over time will really prove to be an independent predictor of outcomes, independent, for example, from N-terminal pro-B-type natriuretic peptide levels that may be easier to obtain. Furthermore, longitudinal studies may allow to assess whether interventions such as aggressive treatment of systemic arterial hypertension or interventional treatment of residual coarctation may have an impact on H_2_FPEF scores and cardiovascular complications.
Funding support and author disclosures
The author has reported that he has no relationships relevant to the contents of this article to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tobler D.Schwerzmann M.Bouchardy J.Swiss Adult Congenital H Eart disease Registry (SACHER)—rationale, design and first results Swiss Med Wkly 1472017 w 1451910.4414/smw.2017.1451929120021 · doi ↗ · pubmed ↗
- 2Diller G.P.Kempny A.Alonso-Gonzalez R.Survival prospects and circumstances of death in contemporary adult congenital heart disease patients under follow-up at a large tertiary centre Circulation 1322015211821252636935310.1161/CIRCULATIONAHA.115.017202 · doi ↗ · pubmed ↗
- 3Greutmann M.Tobler D.Changing epidemiology and mortality in adult congenital heart disease: looking into the future Future Cardiol 820121711772241397710.2217/fca.12.6 · doi ↗ · pubmed ↗
- 4Crossland D.S.Jansen K.Parry G.Outcome following heart transplant assessment in adults with congenital heart disease Heart 1052019174117473127814210.1136/heartjnl-2019-314711 PMC 6855839 · doi ↗ · pubmed ↗
- 5Egbe A.C.Miranda W.R.Reddy Y.N.V.Prognostic value of the H 2FPEF score in adults with repaired coarctation of aorta JACC Adv 152022100130