RADIOGRAPHIC EVALUATION OF CONSERVATIVE TREATMENT OF DISTAL RADIUS FRACTURES
Brenno Lopes Cangussu, Henrique Cruz Baldanza, Ricardo Leão Carmo, Daniel Magalhães Nobre, Alexandre Ramos Estanislau, Tomás Santos Vasconcelos Barros

TL;DR
This study examines how radiographic parameters of wrist fractures change over time in patients receiving non-surgical treatment.
Contribution
The study provides insights into the stability of radiographic parameters in conservatively treated distal radius fractures.
Findings
Volar tilt improved after treatment and remained stable until the final visit.
Radial inclination and height initially improved but regressed by the final evaluation.
Stable fractures showed favorable outcomes with conservative therapy.
Abstract
This article aims to evaluate the evolution of radio-graphic parameters (radial tilt, volar tilt, and radial height) of distal radius fractures in patients indicated for conservative treatment at three different times: date of diagnosis, first outpatient visit within 2 weeks after closed reduction, and last outpatient visit. We included 84 patients seen at the emergency department of Hospital Municipal Odilon Behrens, with a diagnosis of distal radius fracture and an indication for conservative treatment. We considered only those patients who had serial radiographs taken at least three different times (n=69) in this analysis. There was an improvement in radiographic parameters of volar tilt after closed reduction and immobilization, which was maintained until the last outpatient visit. Radial inclination and radial height showed increased values from the first to the second…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
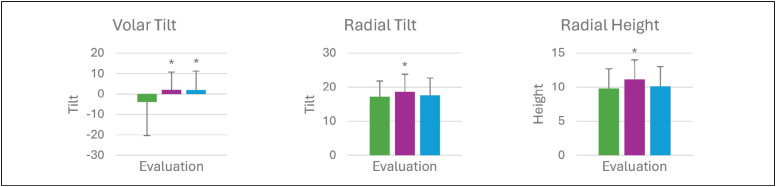 Figure 1
Figure 1| Universal Classification (COONEY) |
| I. Extra-articular without deviation |
| II. Extra-articular with deviation |
| A. Stable reducible |
| B. Unstable reducible |
| C. Irreducible |
| III. Intra-articular without deviation |
| IV. Intra-articular with deviation |
| A. Stable reducible |
| B. Unstable reducible |
| C. Irreducible |
| D. Complex |
| I. fractures produced by angulation of the distal metaphysis of the radius, in which a cortical suffers a degree of comminution, as seen in Colles' and Smith's fractures; |
| II. fractures produced by shear mechanism, such as Barton's fractures and those of the radial styloid apophysis; |
| III. compression of the articular surface with impaction of the subchondral bone and the epiphysis. Current terms used for this fracture are complex articular fracture or radial pilon fracture; |
| IV. avulsion mechanism, includes radial and ulnar styloid fractures associated with carpal displacement; |
| V. fractures produced by high-energy trauma, translated by the combination of the four previous mechanisms, that means, angulation, shear, compression, and avulsion. |
| AO classification - distal radius - 2R3 |
| Extra articular - 2R3A |
| Radial styloid avulsion - 2R3A1 |
| Single line - 2R3A2 |
| Wedge or multifragment 2R3A3 |
| Partial articular - 2R3B |
| Sagittal 2R3B1 |
| (Barton) dorsal rim 2R3B2 |
| (Reverse Barton) volar rim2R3B3 |
| Complete articular 2R3C |
| Simple articular and metaphysis - 2R3C1 |
| Multifragmentary Metaphyseal - 2R3C2 |
| Multifragmentary articular, simple or multifragmentary metaphyseal - 2R3C3 |
| Lafontaine Criteria |
| Dorsal deviation > 20°, dorsal comminution, radial shortening > 9 mm, radiocarpal and distal radioulnar articular involvement, associated ulnar fractures, intra-articular fragment spacing > 2 mm, and age > 60 years. |
| Variable | 1º | 2ª | 3ª | F-value | p-value | n |
|---|---|---|---|---|---|---|
| Volar | -3,8 (16,6) | 2,1 (8,6) | 2,0 (9,2) | 10,92 | <0,001 | 0.05 (Small) |
| Radial | 17,2 (4,6) | 18,6 (5,2) | 17,6 (5,1) | 6,723 | <0,001 | 0.01 (Small) |
| Radio | 9,8 (2,9) | 11,1 (2,9) | 10,1 (2,9) | 11,45 | <0,001 | 0.03 (Small) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopedic Surgery and Rehabilitation · Elbow and Forearm Trauma Treatment · Bone fractures and treatments
INTRODUCTION
Defined as those that occur up to 3 cm from the radius carpal joint, fractures of the distal end of the radius account for 17% of all fractures seen in emergency rooms.^ 1 ^ Middle-aged women are the most affected, with a significant increase in incidence over the age of 50. ^ 2 ^
In order to define the best type treatment it is fundamental to initially classify them in relation to the parameters of instability, reducibility, the fracture mechanism and associated injuries, as well as the patient's age and comorbidities.^ 2 ^
Among the classifications most widely used today, we highlight three that have greater practical applicability because they provide contributions to the treatment and prognosis of fractures: the AO classification, the Universal classification described by Raylock in 1990, modified by Cooney in 1993, and the Fernandez classification, described in 1994 (Board 1, 2 and 3).
Board 1: Universal Classification (COONEY).
Board 2: Fernandez Classification.
Board 3: AO Classification – Distal Radius Fractures.
In a conservative approach, closed reduction of the fracture is performed when necessary and cast immobilization for approximately six weeks. The objective of this intervention is the anatomical restructuring and return of its functionality as close as possible to the physiological one.^ 3 ^
This study, carried out at Hospital Municipal Odilon Behrens - Belo Horizonte - MG, was performed through periodic patient follow-up at the orthopedics/hand surgery outpatient clinic. Radiographic parameters in distal radius fractures were evaluated.
MATERIALS AND METHODS
The study included 84 patients who sought emergency care at the Odilon Behrens Municipal Hospital and whose diagnosis was distal radius fracture. After diagnosis and conservative treatment of the fractures, the patients were followed up as outpatients, performing radiographic control.
Cooney's Universal Classification (Board 1) was used to evaluate the fractures and plan inclusion or exclusion of patients in the study, by means of radiographic criteria.
For analysis in our study, only patients who had undergone out-patient follow-up in our service, with radiographic control in at least three distinct times (n=69), such as: day of diagnosis and immobilization, first outpatient visit (two weeks) and last visit.
There were excluded patients who had deviated and irreducible extra-articular (Cooney IIC), deviated and irreducible articular (Cooney IVC), complex fractures (Cooney IVD), and fractures with more than two criteria of instabilities defined by Lafontaine (Board 4). There were excluded patients who did not have adequate follow-up, did not have radiographic control or did not attend return visits. Two patients who were referred to surgery after two weeks of immobilization due to fracture deviation, were excluded from the study. These two were previously classified as Cooney IVB (intra-articular with deviation and unstable reducible).
Board 4: Lafontaine Criteria.
We take into account three radiographic parameters: radial tilt/ulnar tilt of the radius, volar tilt, and radial height.
All patients in the study were made aware of the risks and benefits of participating in the research through the Free and Informed Consent Form (TCLE), having signed this document.
The present study was approved by the ethics and research committee through the brasil platform under number 5.113.627.
RESULTS
Out of the total 84 patients initially selected in the study, 55 (65%) participants required closed reduction in the emergency room.
Most patients (n=68; 81%) used axillopalmar cast, 10 patients (12%) used antebrachiopalmar cast, 2 patients (2%) used long splint and 2 patients (2%) used short splint immobilization. Out of the total 69 patients included in the study 54 were women (78%), 47 patients were aged 50 years or older (68.11%).
The patients had UNIVERSAL classification information at the date of diagnosis (pre-reduction). Out of this total, 14.2% were classified as Cooney I; 19% Cooney IIA, 8.3% Cooney IIB, 10.7% Cooney III, 4.7% Cooney IVA, 8.3% Cooney IVB.
It was observed a significant increase in volar tilt values during the evaluations, after closed reduction, immobilization, and a new radiography in a return visit (-3.8°, 2.0°) P<0.001. (Table 1) The radial tilt and radial height showed increased values from the first to the second radiographic evaluation. Both values had regression when comparing the second to the third (last) evaluation (17.2° / 18.6° / 17.6°) P<0.001, (9.8 mm/ 11.1 mm/ 10.1 mm) P<0.001. (Figure 1) Data presented on average (standard deviation). * statistically significant difference compared to the first evaluation in the One-Way ANOVA test (p<0.05).
Changes shown by each variable in the three evaluation moments.
DISCUSSION
Wrist fractures involving the distal radius are frequent injuries in emergency care, affecting mostly middle-aged women. With n=54 (78%), they were also predominant in our study.^ 4 ^
With this research it was possible to observe through radiographic criteria, the evolution of the non-surgical treatment of distal radius fractures, using the criteria cited previously.
From the 3 different forms of immobilization (axillopalmar circular cast, antebrachiopalmar circular cast, and short plaster cast), no significant discrepancy was observed in the outcome (loss of measurements obtained in closed reduction at the first and third visits). However, although this was not a randomized study, it was observed a tendency of the use of short splint/plaster for reducible and stable fractures.^ 5-7 ^
In this study, there was an improvement trend in the radiographic parameters from the first to the second moment (after reduction), followed by a slight loss of the values obtained when analyzed at the third moment.
The measurements and angulations of the distal radius are predictors of success in choosing non-surgical treatment. They are: radial height, volar tilt, and radial slope. In a treatment that can vary from 4 to 8 weeks, these values of measurements and angulations classically are responsible for defining the continuation or discontinuation of the therapeutic method, resulting in maintenance of reduction or loss of fracture reduction.^ 8 ^
Radiographic parameters such as volar tilt and radial height correlate closely with clinical outcomes in conservative therapy, so they must be carefully evaluated at well-defined intervals.^ 9 ^
Most distal radius fractures can be treated with non-surgical therapies, even if it is only the first choice. If after a period of radiographic control it is possible to find other treatment options. The exception is for comminuted, intra-articular fractures, and those with significant deviation. For example, 2 patients who were excluded from the study due to a change in treatment: after a conservative approach, were referred to surgery for deviation of a fracture after two weeks of cast immobilization.^ 10 ^
A limiting factor in the study concerns the radiographic indicators, although commonly used, there is no consensus or well-established guidelines as to which descriptors should actually be used and how they should be performed to guide the course and choice for conservative therapy.^ 2 ^
It was possible to analyze the primary outcome: analysis of the radiographic parameters radial height, radial tilt and volar tilt, which have a strong relationship with the primary outcomes.
CONCLUSION
The good follow-up of the conservative treatment is closely linked to a good technique of closed reduction and immobilization with a correctly positioned external imobilization, either short/long or splint. Stable fractures by the Universal classification tend to evolve well with conservative therapy. A change of treatment to the surgical option was observed in two patients who initially had a classification (intra-articular BVI with deviation and unstable reducible).
Indicators such as volar tilt, radial tilt and radial height were the points of important radiographic analysis and divided into three moments, making it possible to infer the evolution of the non-surgical management and predict the clinical results of the conservative choice.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mallmin H Ljunghall S Incident of Colles, fracture in Uppsala A prospective study of a quarter-million population. Acta Orthop Scand 1992632213215159006110.3109/17453679209154826 · doi ↗ · pubmed ↗
- 2Jensen J Rasmussen BS Duus LA Torfing T Precht H Tromborg H Distal radius fractures and radiographic assessment: a systematic review of measurement accuracy Acta Radiol 20196011148214893084581510.1177/0284185119834687 · doi ↗ · pubmed ↗
- 3Barvelink B Reijman M Schep NWL Brown V Kraan GA Gosens T The CAST study protocol: a cluster randomized trial assessing the effect of circumferential casting versus plaster splinting on fracture redisplacement in reduced distal radius fractures in adults BMC Musculoskelet Disord 20212213703703387913110.1186/s 12891-021-04238-0PMC 8059188 · doi ↗ · pubmed ↗
- 4Handoll HH Madhok R Conservative interventions for treating distal radial fractures in adults Cochrane Database Syst Rev 20032 CD 000314 CD 0003141280439510.1002/14651858.CD 000314 · doi ↗ · pubmed ↗
- 5Jamnik AA Chacon J Xiao AX Wagner ER Gottschalk The Effect Immobilization Mechanisms Have on Radiographic Outcomes and Complication Rates in the Conservative Treatment of Distal Radius Fractures: A Systematic Review Hand (N Y)2022171 Suppl 118S 128S 3537359010.1177/15589447221081864 PMC 9793616 · doi ↗ · pubmed ↗
- 6Saka N Hoshika S Inoue M Watanabe J Banno M Below-or above-elbow immobilization in conservative treatment of distal radius fractures: a systematic review and meta-analysis Injury 20225322502583496162510.1016/j.injury.2021.12.021 · doi ↗ · pubmed ↗
- 7Okamura A de Moraes VY Neto JR Tamaoki MJ Faloppa F Belloti JC No benefit for elbow blocking on conservative treatment of distal radius fractures: A 6-month randomized controlled trial Plo S One 2021166 e 02526673411116010.1371/journal.pone.0252667 PMC 8191961 · doi ↗ · pubmed ↗
- 8Zenke Y Furukawa K Furukawa H Maekawa K Tajima T Yamanaka Y Radiographic measurements as a predictor of correction loss in conservative treatment of colles, fracture J UOEH 20194121391443129235710.7888/juoeh.41.139 · doi ↗ · pubmed ↗