Re-thinking all-cause COVID-19 hospitalizations as a surrogate measure for severe illness in observational surveillance studies
J. Daniel Kelly, Samuel Leonard, W. John Boscardin, Katherine J. Hoggatt, Emily N. Lum, Charles C. Austin, Amy L. Byers, Phyllis C. Tien, Dawn M. Bravata, Salomeh Keyhani

TL;DR
This study suggests that using all-cause hospitalizations for severe COVID-19 may be misleading and recommends focusing on hospitalizations directly caused by the virus.
Contribution
The study introduces a method to distinguish between hospitalizations directly caused by SARS-CoV-2 and those coinciding with infection.
Findings
75.3% of all-cause hospitalizations were due to direct SARS-CoV-2 effects.
Unvaccinated individuals had the highest rate of direct SARS-CoV-2 hospitalizations.
Non-COVID-19 hospitalizations increased in the later period (15–30 days) after infection.
Abstract
All-cause COVID-19 hospitalization ≤ 30 days of infection is a common outcome for severe illness in observational/surveillance studies. Milder COVID-19 disease and COVID-19-specific measurements calls for an evaluation of this endpoint. This was a descriptive, retrospective cohort study of adults ≥ 18 who were established in primary care at Veteran Health Administration (VHA) facilities. The outcome was hospitalization within 30 days of a laboratory-confirmed, symptomatic SARS-CoV-2 infection. Between December 15, 2021 and May 1, 2022, a simple random sample of all VA facilities, excluding Puerto Rico or Philippines, was drawn to identify these hospitalized cases and determine whether hospitalization was due to COVID-19-specific causes. A chart review was conducted to record the inpatient clinical team’s diagnosis and whether the inpatient team classified the diagnosis as COVID-19…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
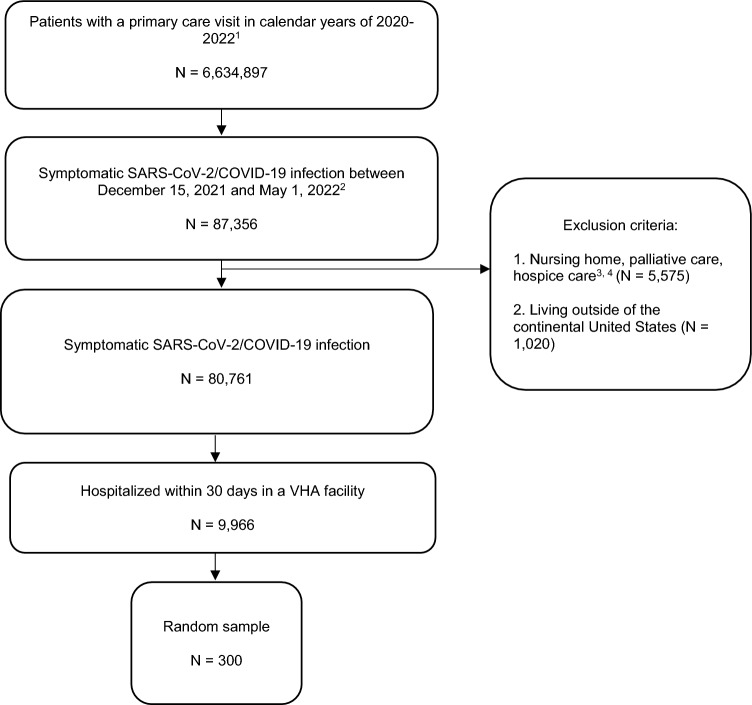 Figure 1
Figure 1- —Veterans Health Administration Clinical Sciences Research and Development
- —http://dx.doi.org/10.13039/100007217Health Services Research and Development
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 epidemiological studies · SARS-CoV-2 and COVID-19 Research · COVID-19 and healthcare impacts
Introduction
Observational, surveillance studies rely on readily available data from electronic health records, insurance databases, or other sources to assess the effectiveness of COVID-19 vaccines or therapeutics through a target trial emulation approach^1–5^. This approach uses all-cause hospitalization after symptomatic COVID-19 as a proxy for COVID-19-related hospitalization with the intent to measure severe illness. In contrast, clinical trials of COVID-19 vaccines and therapeutics have the intensive resources to directly measure COVID-19-related hospitalization^6–8^. The U.S. Veterans Health Administration (VHA) has access to detailed, patient-level data so that chart reviews can be conducted, offering the ability to evaluate all-cause COVID-19 hospitalization for mismeasurement biases.
In an era of vaccines, increasing natural immunity, and viral evolution, it is important to re-evaluate all-cause COVID-19 hospitalization as a useful surrogate outcome in observational studies because COVID-19 disease has been associated with less severe illness and complications, including pneumonia, acute myocardial infarction, and ischemic stroke after infection^9^. Without the late occurrence of cytokine storms, progression to severe illness typically occurs over a shorter period, suggesting that measurement of all-cause COVID-19 hospitalization over a 30-day period may be more likely to detect hospitalizations unrelated than related to COVID-19. At the same time, COVID-19 remains a relatively common occurrence^10^ and infected, symptomatic individuals can be hospitalized for many reasons that may be unrelated to COVID-19 disease (incidental SARS-CoV-2 infections)^10^.
During a period with a predominance of Omicron SARS-CoV-2 variants, this study drew a random sample of all-cause COVID-19 hospitalizations among a national cohort of U.S. Veterans. Reasons for hospitalization documented by the inpatient care team in medical charts were abstracted and used to determine whether the hospitalization was due to a COVID-19-specific cause.
Methods
Ethics statement
The institutional review board of the University of California, San Francisco, approved this study and waived requirement for patient consent, due to the retrospective nature of the study. All methods were performed in accordance with the relevant guidelines and regulations. We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.
Study design, data sources, and participants
We conducted a retrospective cohort study using chart review to describe the proportion of all-cause hospitalizations due to COVID-19-specific or non-COVID-19-specific causes among hospitalized patients with laboratory-confirmed, symptomatic SARS-CoV-2 infection. The cohort included adults aged 18 or older who were established at the U.S. VHA facilities. Exclusion criteria included (1) use of nursing home or hospice care services within the 2 years prior to a COVID-19 diagnosis, and (2) hospitalization in Puerto Rico or the Philippines. We used VA Corporate Data Warehouse (CDW)^11^ and COVID-19 shared data resource^12^ to construct the cohort and identify patients who had laboratory-confirmed, symptomatic SARS-CoV-2 infection and were hospitalized within 30 days of infection. COVID-19 shared data resource was established to document symptomatic infections and hospitalizations occurring outside of VA facilities and integrate these data back into the VA health records. A random sample of hospitalizations was drawn for chart review between December 15, 2021 and May 1, 2022. Thirty percent of these charts were reviewed in duplicate.
Measurements
When reviewing charts, study staff recorded the inpatient clinical team’s diagnosis and whether the inpatient team classified the diagnosis as COVID-19 related or not. Diagnoses related to COVID-19 were defined as COVID-19-specific (direct manifestations of SARS-CoV-2 infection), and those unrelated to COVID-19 were defined as non-COVID-19-specific causes (incidental SARS-CoV-2 infection).
Any hospitalization with unclear labeling and/or disagreement amongst the chart abstractors about the diagnosis being related to COVID-19 was flagged for review by three clinicians (JDK, SK, DMB) and consensus was reached via discussion. An example of unclear labeling in a person with symptomatic SARS-CoV-2 infection was pneumonia, either due to bacterial and viral pathogen, so unless these were witnessed aspiration events, the pneumonia was classified as COVID-19-related since bacterial and viral infections were radiologically indistinguishable. The study team did not overrule any diagnoses or etiological statements made by the clinical team.
Covariates used to describe the cohort were extracted from the VA Corporate Data Warehouse. Those with high-risk comorbid and immunocompromising conditions were classified using U.S. Centers for Disease Prevention and Control definitions^10,13^.
Statistical analysis
The cumulative incidence of all-cause hospitalization was described in the overall cohort and sub-groups stratified by vaccination status (unvaccinated [no vaccine dose], vaccinated but not boosted [received primary series], boosted [received all recommended doses]) and time since infection (0–15 days, 16–30 days). In the random sample, reasons for hospitalization as determined by the abstraction team’s chart review were categorized as COVID-19-specific causes, and non-COVID-19-specific causes. Descriptive statistics with Chi-squared tests were used to compare the proportion of all-cause and cause-specific hospitalizations among those related and not related to COVID-19, stratified by vaccination status and by time since COVID-19 infection. A 2-tailed p < 0.05 was considered significant. Analyses were conducted in R version 1.2.5019.
Results
Among 6,634,897 patients receiving care at VHA facilities, 80,761 had laboratory-confirmed, symptomatic SARS-CoV-2 infection (121.7 events per 10,000 persons; 95% CI: 120.9, 122.6). Among these infected patients, there were 9966 (12.3%) all-cause hospitalizations (95% CI: 12.1%, 12.5%). A simple random sample of this hospitalized population was used to select 300 patients who were representative of the national cohort (Fig. 1). Among these 300 hospitalized patients, 196 (65.3%) were aged 65 or older and 17 (5.7%) were female; 198 (66.0%) had high-risk comorbid conditions and 67 (22.3%) had an immunocompromising condition. See Table 1 for additional characteristics.Figure 1. Cohort selection in U.S. cohort of patients receiving care at Veterans Health Administration (VHA) facilities during a period of Omicron variant predominance and were hospitalized within 30 days of a symptomatic SARS-CoV-2 infection.Table 1. Characteristics of overall hospitalized cohort (N = 300).Overall cohort, N = 300Male283 (94.3)Female17 (5.7)Age, 18–4431 (10.3)Age, 45–6473 (24.3)Age, 65–74109 (36.3)Age, 75–8460 (20.0)Age, 85 or older27 (9.0)American Indian or Alaska Native3 (1.0)Asian2 (0.7)Black or African American74 (24.7)White202 (67.3)Native Hawaiian or other Pacific Islander2 (0.7)More than one race2 (0.7)Unknown15 (5.0)Hispanic or Latino ethnicity (regardless of race)20 (6.7)Married131 (43.7)Urban220 (73.3)Rural64 (21.3)Highly rural7 (2.3)Unknown9 (3.0)Prior history of COVID-198 (2.7)Hypertension213 (71.0)CHF56 (18.7)IHD78 (26.0)Diabetes115 (38.3)Stroke TIA18 (6.0)COPD Bronchiectasis63 (21.0)Cirrhosis10 (3.3)Dementia27 (9.0)Dialysis12 (4.0)Cancer-solid organ20 (6.7)Cancer-lymphoma leukemia11 (3.7)Cancer-other6 (2.0)Current smoker71 (23.7)Alcohol use disorder45 (15.0)Substance use disorder40 (13.3)Housing problems34 (11.3)BMI, < 18.53 (1.0)BMI, 18.5–24.952 (17.3)BMI, 25–29.996 (32.0)BMI, > = 30111 (37.0)Unknown BMI38 (12.7)No Chronic kidney disease204 (68.0)Chronic kidney disease76 (25.3)Severe chronic kidney disease20 (6.7)VA district, Continental49 (16.3)VA district, Midwest51 (17.0)VA district, North Atlantic69 (23.0)VA district, Pacific63 (21.0)VA district, Southeast68 (22.7)Hospitalization 0–15 days post infection280 (93.3)Unvaccinated127 (42.3)Vaccinated-not boosted99 (33.0)Boosted69 (23.0)Vaccinated Status unclear5 (1.7)Age > = 65 and no high-risk conditions21 (7.0)High-risk co-morbid conditions (not immunocompromised),198 (66.0)Immunocompromised67 (22.3)
Among all-cause hospitalizations, 226/300 (75.3%) were determined to be COVID-19-specific. The most common causes of the 226 COVID-19-specific hospitalizations were as follows: COVID-19 pneumonia, 147 (65.0%); cardiovascular events (e.g., myocarditis, new onset atrial fibrillation), 23 (10.2%); weakness/falls, 12 (5.3%); COPD/asthma exacerbation, 8 (3.5%); neurocognitive disorders (e.g., encephalopathy), 8 (3.5%); and gastrointestinal (GI) illness (e.g., diarrhea), 10 (4.0%). The remaining hospitalizations (74/300, 24.7%) were non-COVID-19-specific. The most common causes of the 74 non-COVID-19-specific hospitalizations were as follows: GI illness (e.g., recurrent GI bleeding, abdominal pain from constipation), 17 (23.0%); mental illness or substance abuse (e.g., alcohol withdrawal), 16 (21.6%); non-COVID infectious disease (e.g., urinary tract infection), 15 (20.3%); cardiovascular events (e.g., hypertensive emergency off blood pressure medications), 6 (8.1%); and pain syndrome, 6 (8.1%). See Table 2 for other diagnoses classified as COVID-specific or non-COVID-19-specific hospitalizations. See Supplement for descriptions of these diagnoses during the hospitalization and whether the case was classified as COVID-19-specific or non-COVID-19-specific. Table 2. Classification of all-cause hospitalizations as COVID-19-specific hospitalizations (N = 247) or non-COVID-19-specific hospitalizations (N = 73).TotalBy vaccination statusBy time elapsed between breakthrough infection and admissionBoostedVaccinated, not boostedNot vaccinatedStatus unclearp-value for COVID-specific versus non-specificHospitalized 0–15 daysHospitalized 16–30 daysp*-value for COVID-specific versus non-specificOverall3006999127528020COVID-19-specific hospitalizations All226 (75.3)41 (59.4)73 (73.7)108 (85.0)4 (80.0) < 0.001217 (77.5)9 (45)0.003 COVID-19 pneumonia147 (65.0)26 (63.4)40 (54.8)79 (73.1)2 (50.0)145 (66.8)2 (22.2) Cardiovascular events23 (10.2)3 (7.3)10 (13.7)9 (8.3)1 (25.0)22 (10.1)1 (11.1) Weakness/falls12 (5.3)2 (4.9)6 (8.2)3 (2.8)1 (25.0)11 (5.1)1 (11.1) COPD/asthma exacerbation8 (3.5)4 (9.8)0 (0.0)4 (3.7)0 (0.0)7 (3.2)1 (11.1) Neurocognitive disorders8 (3.5)1 (2.4)4 (5.5)3 (2.8)0 (0.0)7 (3.2)1 (11.1) Gastrointestinal illness8 (3.5)0 (0.0)4 (5.5)4 (3.7)0 (0.0)7 (3.2)1 (11.1) Other6 (2.7)2 (4.9)4 (5.5)0 (0.0)0 (0.0)6 (2.8)0 (0.0) Thromboembolic events4 (1.8)1 (2.4)2 (2.7)1 (0.9)0 (0.0)4 (1.8)0 (0.0) Isolation/observation for COVID 194 (1.8)1 (2.4)0 (0.0)3 (2.8)0 (0.0)4 (1.8)0 (0.0) Kidney disease3 (1.3)1 (2.4)1 (1.4)1 (0.9)0 (0.0)2 (0.9)1 (11.1) Non-COVID infectious disease3 (1.3)0 (0.0)2 (2.7)1 (0.9)0 (0.0)2 (0.9)1 (11.1)Non-COVID-19-specific hospitalizations All74 (24.7)28 (40.6)26 (26.3)19 (15.0)1 (20.0)63 (22.5)11 (55.0) GI illness17 (23.0)9 (32.1)5 (19.2)3 (15.8)0 (0.0)13 (20.6)4 (36.4) Mental illness or substance abuse16 (21.6)3 (10.7)6 (23.1)7 (36.8)0 (0.0)13 (20.6)3 (27.3) Non-COVID infectious disease15 (20.3)8 (28.6)4 (15.4)2 (10.5)1 (100.0)14 (22.2)1 (9.1) Cardiovascular events6 (8.1)2 (7.1)2 (7.7)2 (10.5)0 (0.0)6 (9.5)0 (0.0) Pain syndrome6 (8.1)2 (7.1)2 (7.7)2 (10.5)0 (0.0)6 (9.5)0 (0.0) Genitourinary illness5 (6.8)2 (7.1)1 (3.8)2 (10.5)0 (0.0)4 (6.3)1 (9.1) Other4 (5.4)1 (3.6)2 (7.7)1 (5.3)0 (0.0)4 (6.3)0 (0.0) Neurocognitive disorders2 (2.7)0 (0.0)2 (7.7)0 (0.0)0 (0.0)2 (3.2)0 (0.0) Oncology2 (2.7)1 (3.6)1 (3.8)0 (0.0)0 (0.0)1 (1.6)1 (9.1) Kidney disease1 (1.4)0 (0.0)1 (3.8)0 (0.0)0 (0.0)0 (0.0)1 (9.1)*More details of these diagnoses are described in the Supplement.
The proportion of COVID-19-specific hospitalizations among all-cause hospitalizations varied by vaccination status. The highest proportion of COVID-19-specific hospitalizations occurred among the unvaccinated group (108/127, 85.0%), followed by the vaccinated but not boosted group (73/99, 73.7%) and boosted group (41/69, 59.4%) (p < 0.001). Stratified by time since infection (0–15 days, 15–30 days), the majority of all-cause hospitalizations (280, 93.3%) occurred within the first 15 days of infection. The proportion of non-COVID-19-specific hospitalizations was higher in the later period (15–30 days: 11/20, 55.0%) than the early period (0–15 days: 63/280, 22.5%) (p = 0.003) (Table 2).
Discussion
In this cohort of patients hospitalized at VHA facilities 30 days after symptomatic SARS-CoV-2 infection, we evaluated the extent to which all-cause hospitalization within 30 days of symptomatic SARS-CoV-2 infection remains a useful outcome for severe COVID-19 illness in observational, surveillance studies. Consistent with the literature^14,15^, about one-quarter of all-cause hospitalizations were non-COVID-19-specific (incidental SARS-CoV-2 infection). A higher proportion of non-COVID-19-specific hospitalizations occurred among those who were boosted than unvaccinated and among those hospitalized 16–30 days instead of 0–15 days after infection. As the U.S. population has become highly immunized to COVID-19 either through vaccination or infection and as the clinical spectrum of illness has moderated^9^, continued use of all-cause hospitalization within 30 days of symptomatic SARS-CoV-2 infection as a study outcome should be approached with caution because of its trade-off between sensitivity and specificity.
Hospitalization within 15 days after symptomatic SARS-CoV-2 infection was a more specific measurement of COVID-19 hospitalization than within 30 days and may be less prone to measurement bias. Over time, the likelihood that SARS-CoV-2 infection results in a hospitalization due to COVID-19-specific causes decreases; thus we expect to observe more incidental SARS-CoV-2 infections during this later period (16–30 days). In addition, summary measures of COVID-19-specific hospitalization have yet to be validated. This study found hospitalization due to COVID-19 pneumonia accounted for most COVID-19-specific causes and can be identified with an ICD-10 code and chart review. To this end, most studies attempting to use a specific outcome have focused on the most common, cause-specific diagnoses such as pneumonia^10^, and to a lesser extent, arterial and venous thrombotic events^16^. A tradeoff of these more focused analyses has been the loss of sensitivity, which could slow down research on time-sensitive questions.
There are limitations of this study. First, we relied on the inpatient medical team’s assessment of the cause for hospitalization. In some cases, the team’s indicated diagnosis was clearly not related to COVID-19 (e.g., fracture, fall, pain, substance use) but in other cases distinguishing etiology of symptoms was more challenging (e.g., progression of kidney disease). Second, the study population was predominantly White men and included community-dwelling individuals living in the U.S. Third, it is likely that the proportion of all-cause hospitalization (12.3%) was an overestimate given the timeframe under investigation (large Omicron wave). Additional limitations of generalizability extend to Omicron variants beyond BA.1 and BA.2 and after receipt of the bivalent Omicron booster vaccine. Finally, during the observational study period, rapid antigen test became available, so the total number of cases was an underestimate.
Evidence from this study supports use of COVID-19-specific hospitalization in many scenarios instead of all-cause hospitalization in observational surveillance studies. Further, the earlier period (0–15 days) of the outcome was less susceptible to potential measurement bias in contrast to the later period (16–30 days). This report highlights the importance of re-evaluating clinical endpoints in an evolving landscape of viral variants and booster vaccine.
Supplementary Information
Supplementary Information.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dickerman BA Gerlovin H Madenci AL Kurgansky KE Ferolito BR Figueroa Muñiz MJ Comparative effectiveness of BNT 162b 2 and m RNA-1273 vaccines in U.S. Veterans N. Engl. J. Med.2022386210511510.1056/NEJ Moa 211546334942066 PMC 8693691 · doi ↗ · pubmed ↗
- 2Ioannou GN Locke ER Green PK Berry K Comparison of Moderna versus Pfizer-Bio N Tech COVID-19 vaccine outcomes: A target trial emulation study in the U.S. veterans affairs healthcare system E Clinical Medicine 20224510132610.1016/j.eclinm.2022.10132635261970 PMC 8896984 · doi ↗ · pubmed ↗
- 3Tenforde MW Self WH Adams K Gaglani M Ginde AA Mc Neal T Association between m RNA Vaccination and COVID-19 hospitalization and disease severity JAMA.2021326202043205410.1001/jama.2021.1949934734975 PMC 8569602 · doi ↗ · pubmed ↗
- 4Dagan N Barda N Kepten E Miron O Perchik S Katz MABNT 162b 2 m RNA Covid-19 vaccine in a nationwide mass vaccination setting N. Engl. J. Med.2021384141210.1056/NEJ Moa 210176533626250 PMC 7944975 · doi ↗ · pubmed ↗
- 5Kelly, J. D. et al. Comparative m RNA booster effectiveness against death or hospitalization with COVID-19 pneumonia across at-risk US Veteran populations. Nat. Commun.14(1), 2976. 10.1038/s 41467-023-38503-8 (2023).10.1038/s 41467-023-38503-8PMC 1020503237221198 · doi ↗ · pubmed ↗
- 6Hammond J Leister-Tebbe H Gardner A Abreu P Bao W Wisemandle W Oral Nirmatrelvir for high-risk, nonhospitalized adults with Covid-19N. Engl. J. Med.2022386151397140810.1056/NEJ Moa 211854235172054 PMC 8908851 · doi ↗ · pubmed ↗
- 7Polack FP Thomas SJ Kitchin N Absalon J Gurtman A Lockhart S Safety and efficacy of the BNT 162b 2 m RNA Covid-19 vaccine N. Engl. J. Med.2020383260310.1056/NEJ Moa 203457733301246 PMC 7745181 · doi ↗ · pubmed ↗
- 8Baden LR El Sahly HM Essink B Kotloff K Frey S Novak R Efficacy and safety of the m RNA-1273 SARS-Co V-2 vaccine N. Engl. J. Med.202010.1056/NEJ Moa 203538933378609 PMC 7787219 · doi ↗ · pubmed ↗