Absolute Lymphocyte Count Predicts Bypass Surgery Outcomes in Patients with Chronic Limb-Threatening Ischemia
Satoshi Yamamoto, Takuya Hashimoto, Masaya Sano, Masaru Kimura, Osamu Sato, Juno Deguchi

TL;DR
Higher absolute lymphocyte counts are linked to better survival and limb salvage after bypass surgery in patients with severe leg ischemia.
Contribution
This study identifies absolute lymphocyte count as a novel predictor of outcomes in chronic limb-threatening ischemia bypass surgery.
Findings
Higher ALC groups showed significantly better survival rates (cut-off 1030/μL, p = 0.0009).
Limb salvage rates were significantly higher in higher ALC groups (cut-off 1260/μL, p = 0.0081).
ALC was independently associated with limb loss in multivariate analysis.
Abstract
Objectives: The aim of this study was to evaluate the relationship between absolute lymphocyte count (ALC) and outcomes of infrainguinal bypass surgery for chronic limb-threatening ischemia (CLTI). Methods: From 2004 to 2020, 209 limbs of 189 patients who underwent infrainguinal bypass surgery for CLTI and whose ALCs were available were included. Patients with survival >2 years and limb salvage >2 years were considered discriminant groups, and an ALC cut-off value was calculated. The relationship between preoperative ALC and outcomes was evaluated. Results: Survivorship of the higher ALC group was significantly higher than that of the lower ALC group (cut-off value 1030/μL, p = 0.0009). The limb salvage rate of the higher ALC group was significantly higher than that of the lower ALC group (cut-off value 1260/μL, p = 0.0081). In the dialysis patient group (103 limbs), the limb salvage…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
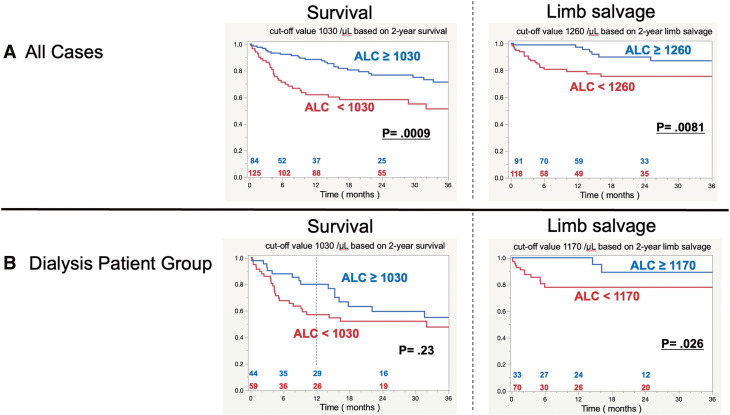 Figure 1
Figure 1| All | Dialysis patient group | Nondialysis patient group | p Value | |
|---|---|---|---|---|
| Age (years), mean ± SD | 72.7 ± 8.6 | 71.7 ± 7.7 | 73.7 ± 9.2 | 0.082 |
| Male/female | 156/53 | 81/22 | 75/31 | 0.21 |
| Body mass index (kg/m2) | 21.7 ± 3.5 | 21.7 ± 3.2 | 21.8 ± 3.7 | 0.85 |
| Smoking history | 155 (74%) | 76 (74%) | 79 (75%) | 1.0 |
| Current smoking | 55 (35%) | 19 (19%) | 36 (34%) | |
| Ex-smoking | 100 (65%) | 57 (55%) | 43 (41%) | |
| Comorbid diseases | ||||
| Hypertension, n (%) | 164 (78%) | 87 (84%) | 77 (73%) | 0.044 |
| Dyslipidemia, n (%) | 70 (33%) | 30 (29%) | 40 (38%) | 0.24 |
| Diabetes mellitus, n (%) | 157 (75%) | 89 (86%) | 68 (64%) | 0.0002 |
| Coronary artery disease, n (%) | 68 (33%) | 40 (39%) | 28 (26%) | 0.076 |
| Chronic heart failure, n (%) | 32 (15%) | 19 (18%) | 13 (12%) | 0.25 |
| Cerebrovascular disease, n (%) | 57 (27%) | 33 (32%) | 24 (23%) | 0.16 |
| Medications | ||||
| Anticoagulant drug use | 42 (33%) | 21 (20%) | 21 (20%) | 1.0 |
| Antiplatelet drug use | 175 (84%) | 93 (90%) | 82 (77%) | 0.014 |
| Statin use | 59 (28%) | 23 (22%) | 36 (34%) | 0.067 |
| Ambulatory status at registration | ||||
| Nonambulatory | 118 (56%) | 61 (59%) | 57 (54%) | 0.49 |
| WIfI classification | 0.47 | |||
| Grade 1 | 2 (1%) | 1 (1%) | 1 (1%) | |
| Grade 2 | 6 (3%) | 2 (2%) | 4 (4%) | |
| Grade 3 | 44 (21%) | 17 (16%) | 27 (25%) | |
| Grade 4 | 157 (75%) | 83 (81%) | 74 (70%) | |
| Contralateral limb status | ||||
| CLTI | 90 (43%) | 57 (55%) | 33 (31%) | 0.0005 |
| Laboratory data | ||||
| White blood cells (count/μL), mean ± SD | 8502 ± 3285 | 8430 ± 2908 | 8572 ± 3626 | 0.75 |
| Neutrophil (count/μL), mean ± SD | 6361 ± 3134 | 6482 ± 2709 | 6243 ± 3507 | 0.58 |
| Lymphocytes = ALC (count/μL), mean ± SD | 1282 ± 637 | 1017 ± 454 | 1539 ± 684 | <0.0001 |
| Hemoglobin (g/dL), mean ± SD | 10.63 ± 1.86 | 9.78 ± 1.34 | 11.46 ± 1.92 | <0.0001 |
| Serum albumin (g/dL), mean ± SD | 3.14 ± 0.59 | 3.00 ± 0.52 | 3.26 ± 0.62 | 0.0013 |
| C-reactive protein (mg/dL), mean ± SD (range, median) | 3.79 ± 4.89 (0–24.9, 1.6) | 4.5 ± 5.3 (0.0–24.9, 2.5) | 3.1 ± 4.3 (0.0−22.5, 1.2) | 0.033 |
| Total cholesterol (mg/dL), mean ± SD | 161.2 ± 44.6 (n = 198) | 144.9 ± 38.1 (n = 96) | 176.4 ± 45.0 (n = 102) | <0.0001 |
| Distal anastomosis site in infrainguinal arterial reconstruction | ||||
| Popliteal artery above the knee, n (%) | 34 (16%) | 17 (16%) | 17 (16%) | |
| Popliteal artery below the knee, n (%) | 32 (15%) | 15 (15%) | 17 (16%) | |
| Tibioperoneal trunk, n (%) | 6 (3%) | 1 (1%) | 5 (4%) | |
| Anterior tibial artery, n (%) | 34 (16%) | 17 (16%) | 17 (16%) | |
| Posterior tibial artery, n (%) | 39 (19%) | 18 (18%) | 21 (20%) | |
| Peroneal artery, n (%) | 16 (8%) | 6 (6%) | 10 (10%) | |
| Dorsal pedis artery, n (%) | 35 (17%) | 26 (25%) | 9 (8%) | |
| Plantar artery, n (%) | 13 (6%) | 3 (3%) | 10 (10%) | |
| Leading causes of death | All | Dialysis patient group | ||
|---|---|---|---|---|
| (n = 67) | (n = 46) | Within 1 year | From the first year on | |
| Cardiovascular event, n (%) | 19 (28%) | 12 (26%) | 7 (23%) | 5 (33%) |
| Heart failure | 15 | 10 | 7 | 3 |
| Myocardial infarction | 2 | 1 | 0 | 1 |
| Arrhythmia (VT/VF) | 2 | 1 | 0 | 1 |
| Cerebrovascular event, n (%) | 4 (6%) | 3 (7%) | 3 (10%) | 0 (0%) |
| Bleeding | 2 | 1 | 1 | 0 |
| Infarction | 2 | 2 | 2 | 0 |
| Respiratory event, n (%) | 6 (9%) | 3 (7%) | 1 (3%) | 2 (13%) |
| Pneumonia | 5 | 3 | 1 | 2 |
| Asthma | 1 | 0 | 0 | 0 |
| Renal failure, n (%) | 5 (7%) | 5 (11%) | 3 (10%) | 2 (13%) |
| Gastrointestinal event, n (%) | 2 (4%) | 2 (4%) | 2 (6%) | 0 (0%) |
| Bleeding | 1 | 1 | 1 | 0 |
| Peritonitis | 1 | 1 | 1 | 0 |
| Pancreatitis/cholangitis, n (%) | 1 | 0 | 0 | 0 |
| Malignant disease, n (%) | 5 (7%) | 1 (2%) | 1 (3%) | 0 |
| Sepsis, n (%) | 14 (21%) | 11 (24%) | 9 (29%) | 2 (13%) |
| Suicide, n (%) | 1 (1%) | 1 (2%) | 1 (3%) | 0 |
| Unknown, n (%) | 10 (15%) | 8 (17%) | 4 (13%) | 4 (27%) |
| Variable | Univariate analysis | Multivariate analysis | ||||
|---|---|---|---|---|---|---|
| p | HR | 95% CI | p | HR | 95% CI | |
| High age (≥80 years) | 0.046 | 1.82 | 1.01–3.26 | 0.020 | 2.10 | 1.123–3.90 |
| Male | 0.31 | 1.34 | 0.76–2.36 | |||
| Low body mass index (<18.5 kg/m2) | 0.23 | 1.40 | 0.81–2.43 | |||
| Hypertension | 0.11 | 1.72 | 0.88–3.37 | |||
| Dyslipidemia | 0.026 | 0.53 | 0.30–0.93 | 0.020 | 0.50 | 0.28–0.90 |
| Diabetes mellitus | 0.12 | 1.66 | 0.87–3.17 | |||
| Coronary artery disease | 0.0012 | 2.26 | 1.38–3.69 | 0.0002 | 2.68 | 1.59–4.54 |
| Chronic heart failure | 0.011 | 2.24 | 1.20–4.16 | 0.48 | 1.27 | 0.65–2.46 |
| Cerebrovascular disease | 0.13 | 1.50 | 0.88–2.54 | |||
| Hemodialysis | <0.0001 | 2.84 | 1.69–4.78 | 0.0034 | 2.44 | 1.34–4.42 |
| Nonambulatory | 0.0061 | 2.04 | 1.23–3.39 | 0.23 | 1.40 | 0.80–2.46 |
| WIfI grade 4 | 0.13 | 1.66 | 0.87–3.17 | |||
| Contralateral limb status CLTI | 0.088 | 1.52 | 0.94–2.45 | |||
| Low ALC (<1030/μL) | 0.0012 | 2.23 | 1.37–3.62 | 0.50 | 1.21 | 0.69–2.11 |
| Low hemoglobin (<10 g/dL) | 0.0027 | 2.09 | 1.29–3.39 | 0.81 | 0.93 | 0.53–1.66 |
| Low serum albumin (<3.0 g/dL) | 0.0007 | 2.30 | 1.42–3.74 | 0.0075 | 2.12 | 1.22–3.67 |
| Variable | Univariate analysis | Multivariate analysis | ||||
|---|---|---|---|---|---|---|
| p | HR | 95% CI | p | HR | 95% CI | |
| High age (≥80 years) | 0.82 | 1.12 | 0.42–2.95 | |||
| Male | 0.53 | 1.27 | 0.37–1.68 | |||
| Low body mass index (<18.5 kg/m2) | 0.039 | 2.23 | 1.04–4.79 | 0.083 | 1.98 | 0.91–4.27 |
| Hypertension | 0.40 | 1.40 | 0.33–1.56 | |||
| Dyslipidemia | 0.48 | 1.33 | 0.34–1.65 | |||
| Diabetes mellitus | 0.88 | 1.07 | 0.46–2.50 | |||
| Coronary artery disease | 0.12 | 1.78 | 0.86–3.69 | |||
| Chronic heart failure | 0.42 | 1.50 | 0.57–3.95 | |||
| Cerebrovascular disease | 0.096 | 1.88 | 0.89–3.98 | |||
| Hemodialysis | 0.40 | 1.36 | 0.66–2.79 | |||
| Nonambulatory | 0.034 | 2.31 | 1.07–4.99 | 0.35 | 1.49 | 0.64–3.45 |
| WIfI grade 4 | 0.29 | 1.68 | 0.64–4.39 | |||
| Contralateral limb status CLTI | 0.065 | 1.98 | 0.96–4.09 | |||
| Low ALC (<1260/μL) | 0.011 | 2.87 | 1.27–6.48 | 0.044 | 2.38 | 1.03–5.55 |
| Low hemoglobin (<10 g/dL) | 0.029 | 2.23 | 1.09–4.58 | 0.52 | 1.31 | 0.57–2.98 |
| Low serum albumin (<3.0 g/dL) | 0.011 | 2.56 | 1.24–5.29 | 0.20 | 1.71 | 0.75–3.90 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Artery Disease Management · Cerebrovascular and Carotid Artery Diseases · Acute Ischemic Stroke Management
Introduction
In treating chronic limb-threatening ischemia (CLTI), it is important to consider patient life expectancy to determine the best treatment for limb salvage.1^–^3) Previous studies have proposed several models to predict life expectancy and limb salvage in the treatment of CLTI.4^–^8) However, a simple and practical predictive method has yet to be established, and there is room for improvement of extant prediction models for several reasons peculiar to CLTI: (1) the diversity of comorbid diseases and the complexity of pathological conditions; (2) two methods of revascularization for ischemia, bypass surgery, and endovascular treatment; (3) advances in endovascular treatment; and (4) institutional or national differences in backgrounds and treatment policy. In particular, patients undergoing hemodialysis tend to have the worst prognosis among patients with CLTI, and it is difficult to predict outcomes after revascularization in patients undergoing hemodialysis.9^,^10) In Japan, approximately 50% of patients undergoing hemodialysis need revascularization treatment for CLTI.11^,^12) It is still necessary to search for an accurate and straightforward indicator to improve predictive methods for CLTI prognosis.
Poor nutritional status and hemodialysis are among the most common risk factors in predicting survival and limb prognosis in patients with CLTI.9) There is a strong correlation between nutritional status and immunological capacity.13) Factors to assess patient nutritional and immune status include serum albumin and body mass index, and multi-item nutritional evaluation measures, such as the Geriatric Nutritional Risk Index (GNRI) and controlling nutritional status (CONUT) score.9) Among these, absolute lymphocyte count (ALC) is supposed to be one of the most objective and simple indicators because it is little affected by short-term inflammation and preoperative treatment. In the treatment of CLTI, ALC is a statistically significant predictor of amputation-free survival, as described in the univariate analysis in the PREVENT III derivation set.14) However, few reports are available on ALC in the treatment of CLTI, and the usefulness of ALC remains to be clarified.
When considering a revascularization method for CLTI, it is important to predict the outcomes of bypass surgery and endovascular treatment. We previously reported that the CONUT score, calculated from ALC, serum albumin level, and total cholesterol level, may be predictors of survival and limb salvage in patients undergoing bypass surgery for CLTI.15) However, the serum albumin level fluctuates due to fluid infusion and hepatic function, and the total cholesterol level is affected by diet and medication. On the other hand, ALC is supposed to be stable, irrespective of those factors. In this study, we examined patients who underwent infrainguinal bypass surgery for CLTI in order to clarify the usefulness of ALC in predicting survival and limb salvage.
Subjects and Methods
Patients
From 2004 to 2020, 209 limbs of 189 patients who underwent infrainguinal bypass surgery for CLTI with tissue loss due to atherosclerosis obliterans and whose ALCs could be calculated were included in the study. Values of each measurement were the most recent values measured before the revascularization procedure was performed (in principle, within one week).
This study was conducted following ethical guidelines for medical research involving human subjects and was approved by the Institutional Review Board of Saitama Medical Center (approval no. 2008).
Surgical strategy
As a surgical strategy, if a patient was judged to be operable as per preoperative systemic evaluation, infrainguinal revascularization was performed for limb salvage. Preoperative, contrast-enhanced, computed tomography (CT), angiography, and ultrasonography were performed, and bypass surgery was considered to ensure in-line flow to the foot. Patients without an appropriate arterial anastomosis or an autologous vein graft for distal bypass were deemed ineligible for limb bypass. Patients with necrosis or infection extending above the heel were excluded because they were not eligible for limb salvage bypass surgery. In addition, patients subjected to incomplete revascularization were also excluded. In the postoperative period, graft patency was confirmed by palpation, Doppler auscultation, ultrasonography (duplex scan), or CT scans recommended at specific intervals: one week, one month, 3 and 6 months, one year, and every 6–12 months after that.
Endpoints
Relationships between preoperative ALC and patient background, clinical findings, survival rate, and limb salvage rate were retrospectively evaluated.
Statistical analysis
Data were presented as means and standard deviations (SDs). Student’s t-test or Chi-square/Fisher’s exact test was used for statistical analysis. Patients with survival of >2 years and limb salvage were considered discriminant groups. The Youden Index and the receiver operating characteristic curve were used to calculate the ALC cut-off value. Survival and limb salvage were compared. The Kaplan–Meier method was used to construct survival and limb salvage curves, and the difference between the two groups was determined using the log-rank test. Cox regression analysis was performed on the ALC and factors contributing to survival or limb salvage. The threshold for statistical significance was set at p <0.05. Similarly, outcomes were evaluated, and survival and limb salvage were compared in the dialysis patient group.
Results
Patient characteristics
Patient backgrounds are presented in Table 1. The mean ALC was 1282/μL (ALC reference values, 1500–3200/μL). Ninety-one patients with 103 affected limbs (49%) underwent hemodialysis. ALC was lower in the dialysis patient group than in the nondialysis patient group (mean ALC: 1017/μL vs. 1539/μL, p <0.0001), although there was no difference in the white blood cell and neutrophil counts between the two groups.
**:
Causes of death
The causes of death are presented in Table 2. Cardiovascular events were the most common cause of death, and sepsis was the second. Among dialysis patients, cardiovascular events were the most common cause of death, and chronic heart failure was frequent. However, sepsis was the most common cause of death within one year after bypass surgery.
**:
Analyses of ROC curves
For survival rate, an ALC value of 1030/μL was calculated as the cut-off [sensitivity 53%, specificity 74%, the area under the curve (AUC) 0.64]. A value of 1260/μL (sensitivity 76%, specificity 52%, AUC 0.65) was considered the cut-off value for limb salvage. In the dialysis patient group, 1030/μL (sensitivity 61%, specificity 56%, AUC 0.55) was considered the cut-off survival value. A value of 1170/μL (sensitivity 92%, specificity 48%, AUC 0.67) was considered the cut-off value for limb salvage.
Kaplan–Meier analysis
The survival rate of the higher ALC group was significantly higher than that of the lower ALC group (2-year survival rate: 76.6% vs. 58.2%, p = 0.0009) (Fig. 1A). The mean ± SD of ALC was 1445 ± 704/μL in the patients who survived more than 2 years and 1124 ± 554/μL in the patients who died within 2 years (p = 0.0063).
Fig. 1 Kaplan–Meier curves for overall survival and limb salvage. (A) All cases and (B) the dialysis patient group. ALC: absolute lymphocyte count (/μL)
Although there was no significant difference in primary and secondary graft patency between the higher and lower ALC groups (2-year graft patency rate: 63.9% vs. 63.6%, p = 0.73, and 76.8% vs. 75.8%, p = 0.73, respectively), limb salvage of the higher ALC group was significantly higher than that of the lower ALC group (2-year limb salvage rate: 89.8% vs. 75.5%, p = 0.0081) (Fig. 1A). The mean ± SD of ALC was 1416 ± 663/μL in patients who avoided major amputation for over 2 years and 1126 ± 628/μL in patients who underwent major amputation within 2 years (p = 0.032).
Among dialysis patients, the one-year survival rate was higher in the higher ALC group than in the lower ALC group. Still, no significant difference was observed between the two groups divided as per the cut-off value (1-year survival rate: 80.0% vs. 57.0%, and 2-year survival rate: 59.5% vs. 52.0%, p = 0.23) (Fig. 1B). The limb salvage rate of the higher ALC group was significantly higher than that of the lower ALC group (2-year limb salvage rate: 89.1% vs. 75.7%, p = 0.026) (Fig. 1B).
Statistical analyses with Cox methods
Univariate analysis revealed that at age 80 or over, dyslipidemia, coronary artery disease, chronic heart failure, hemodialysis, nonambulatory status, low ALC, low hemoglobin, and low serum albumin were all significantly correlated with mortality (Table 3). Multivariate analysis revealed that the factors independently associated with mortality in all cases were age 80 or over, which are dyslipidemia, coronary artery disease, hemodialysis, and low serum albumin.
**:
A univariate analysis revealed that low body mass index, nonambulatory status, low ALC, low hemoglobin, and low serum albumin were significantly correlated with limb loss in all cases (Table 4). Multivariate analysis revealed that the factor independently associated with limb loss in all cases was low ALC.
**:
Discussion
One of the most significant differences between Japan and other countries is the high ratio of patients undergoing hemodialysis among patients with CLTI. In Japan, risk factors for all-cause mortality in patients undergoing revascularization for CLTI included old age, impaired mobility, low body mass index, renal failure, heart failure, and high WIfI (Wound, Ischemia, and foot Infection) grade, based on the SPINACH study.7) Miyata et al. proposed a risk prediction model for outcomes of revascularization for CLTI based on the JAPAN Critical Limb Ischemia Database (JCLIMB), and hemodialysis was a strong predictor of major amputation and mortality.8) Hemodialysis is a common, primary risk factor for mortality and limb loss. Still, risk factors in the dialysis group have yet to be fully clarified, whereas patients undergoing hemodialysis have different prognoses. Predictability of prognosis in patients undergoing hemodialysis is also essential for CLTI treatment strategy in Japan.
We searched for an accurate and simple indicator to predict the prognoses of patients, including those undergoing hemodialysis. ALC reflects immunological capacity and nutritional status over a certain period. Although neutrophil counts fluctuate considerably due to acute inflammation and infection, ALC is not susceptible to these factors in the short term. Multi-item nutritional evaluation measures are usually too complex for regular use in clinical practice, but ALC is readily available from routine blood tests. We think that ALC may be the simplest and most readily evaluated variable that reflects patient nutritional and immune status. We suggest that ALC is helpful in predicting the life prognosis of patients with chronic heart failure and malignant diseases.16^,^17) However, another item, such as serum albumin, has been adopted as representative of the nutrition index,9) and few reports are available on ALC in CLTI treatment. Therefore, we focused on ALC in this study.
ALC differed significantly between dialysis and nondialysis patient groups, and we investigated outcomes in all cases and in the dialysis patient group. The optimal cut-off value of ALC was unknown because it fluctuates according to the study population and endpoint. Patients with CLTI tend to have lower ALC than the general population because of their poor nutritional and immune status, and optimal cut-off values of ALC were assumed to differ. Thus, in this study, we found respective cut-off values of ALC on survival and limb salvage rates in each group.
The lower ALC group showed poorer survival and poorer limb salvage than the higher ALC group, and these results suggest that ALC helps predict life and limb prognosis after infrainguinal bypass surgery in patients with CLTI. However, hemodialysis was one of the factors independently associated with mortality, and it is difficult but essential to predict the life prognosis of patients undergoing hemodialysis. The one-year survival rate in the dialysis patient group was higher in the higher ALC group than in the lower ALC group. Sepsis and heart failure were the primary causes of death within one year after bypass surgery in the dialysis patient group.
ALC reflects a general immune state closely related to infection.18) Many studies have suggested that nutritional state is highly correlated with cardiovascular events, including heart failure,19^,^20) and ALC is suggested as a predictor of life prognosis of patients with chronic heart failure.16) Therefore, ALC may stratify the risk of sepsis and heart failure. Because patients undergoing hemodialysis had rather poor prognoses and 31 patients (30%) died within one year, we referred to the 1-year survival and limb salvage. In the dialysis patient group, ALC may be helpful in predicting prognosis within one year after surgery. There are few reports on the outcomes of bypass surgery for CLTI in the dialysis patient group. Accordingly, we think that the findings in the dialysis patient group are worth reporting. Further research is needed with an adequate number of dialysis patients. Regarding limb salvage, low ALC was the only factor independently associated with limb loss, and this result suggests that ALC may be a strong predictor of limb salvage after bypass surgery, independent of hemodialysis. Uncontrollable infection was the most frequent reason for major amputation. ALC can stratify the risk of limb-threatening infection even in the dialysis patient group.
This study had several limitations. First, it was carried out at a single center. Second, it was a retrospective study. There was also a selection bias. An optimal cutoff value of ALC has yet to be established, and finally, the sample size needs to be more robust for multivariate analysis in the dialysis patient group. The prevalence of dyslipidemia was low among patients with CLTI, as in other reports from Japan, and the proportion of patients who received statins was low.8^,^21) We think that the low proportion of statins may influence cardiovascular events and prognoses. We could not examine outcomes after endovascular treatment because there were few patients who underwent endovascular treatment alone. Thus, further research on endovascular treatment and bypass surgery groups is required to clarify ALC's usefulness in developing a CLTI strategy. However, ALC can potentially improve prognosis accuracy in treatment for CLTI because ALC accurately and sensitively reflects patient life- and limb-threatening conditions. ALC has not been regularly evaluated in the treatment of CLTI, but we think that it is worth adding to the analysis as a potential indicator in clinical use. We think that minimally invasive endovascular treatment, primary major amputation, or even nonsurgical treatment may be an option instead of bypass surgery for patients with low ALC because they are expected to have poor prognoses. On the contrary, we think that active bypass surgery is an appropriate option for patients with high ALC because they are expected to have good prognoses. We believe that a study like this one, but including a large number of patients undergoing hemodialysis, may improve the predictability of prognosis in treating CLTI.
Conclusion
ALC appears promising as a predictive indicator after bypass surgery in the treatment of CLTI. In particular, ALC is expected to help predict limb prognosis after bypass surgery in hemodialysis patients. ALC reflects the patient's nutritional and immune state and may stratify the risk of infection and heart failure, which are closely related to life- and limb-threatening conditions. ALC may help improve the predictability of prognosis in CLTI treatment.
Acknowledgments
We thank Dr. Yohei Kawasaki and Dr. Yuki Shiko at the Research Administration Center of Saitama Medical University for advising us on statistical analysis.
Disclosure Statement
All authors have no conflicts of interest.
Author Contributions
Study conception: SY, TH, and JD
Data collection: all authors
Analysis: SY and TH
Investigation: SY, TH, and JD
Manuscript preparation: SY and TH
Funding acquisition: None
Critical review and revision: all authors
Final approval of the article: all authors
Accountability for all aspects of the work: all authors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bradbury AW, Adam DJ, Bell J, et al. BASIL trial Participants. Bypass versus Angioplasty in Severe Ischaemia of the Leg (BASIL) trial: an intention-to-treat analysis of amputation-free and overall survival in patients randomized to a bypass surgery-first or a balloon angioplasty-first revascularization strategy. J Vasc Surg 2010; 51 Suppl: 5S–17S.20435258 10.1016/j.jvs.2010.01.073 · doi ↗ · pubmed ↗
- 2Rooke TW, Hirsch AT, Misra S, et al. Society for Cardiovascular Angiography and Interventions; Society of Interventional Radiology; Society for Vascular Medicine; Society for Vascular Surgery. 2011 ACCF/AHA focused update of the guideline for the management of patients with peripheral artery disease (updating the 2005 guideline): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2011; 58: 2020–45.21963765 10. · doi ↗ · pubmed ↗
- 3Tendera M, Aboyans V, Bartelink ML, et al. European Stroke Organisation; ESC Committee for Practice Guidelines. ESC Guidelines on the diagnosis and treatment of peripheral artery diseases: document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteries: The Task Force on the Diagnosis and Treatment of Peripheral Artery Diseases of the European Society of Cardiology (ESC). Eur Heart J 2011; 32: 2851–906.21873417 10.1093/eurhea · doi ↗ · pubmed ↗
- 4Simons JP, Goodney PP, Flahive J, et al. A comparative evaluation of risk-adjustment models for benchmarking amputation-free survival after lower extremity bypass. J Vasc Surg 2016; 63: 990–7.26603547 10.1016/j.jvs.2015.09.051PMC 5315434 · doi ↗ · pubmed ↗
- 5Arvela E, Söderström M, Korhonen M, et al. Finnvasc score and modified Prevent III score predict long-term outcome after infrainguinal surgical and endovascular revascularization for critical limb ischemia. J Vasc Surg 2010; 52: 1218–25.20709482 10.1016/j.jvs.2010.06.101 · doi ↗ · pubmed ↗
- 6Moxey PW, Brownrigg J, Kumar SS, et al. The BASIL survival prediction model in patients with peripheral arterial disease undergoing revascularization in a university hospital setting and comparison with the FINNVASC and modified PREVENT scores. J Vasc Surg 2013; 57: 1–7.23040797 10.1016/j.jvs.2012.04.074 · doi ↗ · pubmed ↗
- 7Azuma N, Takahara M, Kodama A, et al. Predictive model for mortality risk including the wound, ischemia, foot infection classification in patients undergoing revascularization for critical limb ischemia. Circ Cardiovasc Interv 2019; 12: e 008015.31771341 10.1161/CIRCINTERVENTIONS.119.008015 · doi ↗ · pubmed ↗
- 8Miyata T, Mii S, Kumamaru H, et al. Risk prediction model for early outcomes of revascularization for chronic limb-threatening ischaemia. Br J Surg 2021; 108: 941–50.33693591 10.1093/bjs/znab 036 · doi ↗ · pubmed ↗