Right Lower Pulmonary Vein Thrombi and Right Upper Pulmonary Vein Thrombi Connected on the Anterior Wall of the Left Atrium
Hidekazu Takeuchi

TL;DR
This study shows for the first time that blood clots in two pulmonary veins can connect on the left atrium's anterior wall using advanced imaging techniques.
Contribution
First direct demonstration of RUPV and RLPV thrombi connection on the LA anterior wall using TEE and 80-MDCT.
Findings
RUPV and RLPV thrombi invade the left atrium and reach its anterior wall.
The connection between RUPV and RLPV thrombi was directly visualized using TEE and 80-MDCT.
This connection was previously unknown and highlights a new anatomical interaction.
Abstract
The interaction between the right upper pulmonary vein (RUPV) and the right lower pulmonary vein (RLPV) is poorly understood. In this paper, using transesophageal echocardiography (TEE) and 80-slice multidetector computed tomography (80-MDCT), we report that the RUPV thrombi and the RLPV thrombi invade the left atrium (LA) and reach the anterior wall of the LA. To our knowledge, this is the first study to directly show the connection between the RUPV thrombi and the RLPV thrombi on the anterior wall of the LA using TEE and 80-MDCT.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1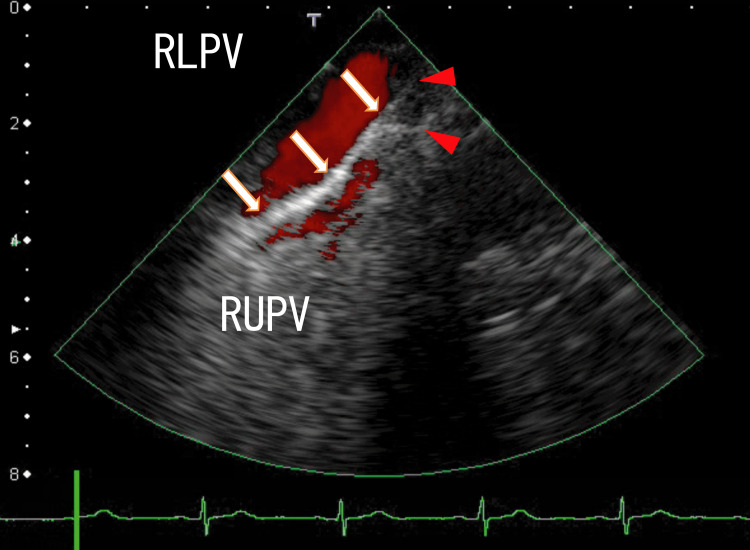 Figure 2
Figure 2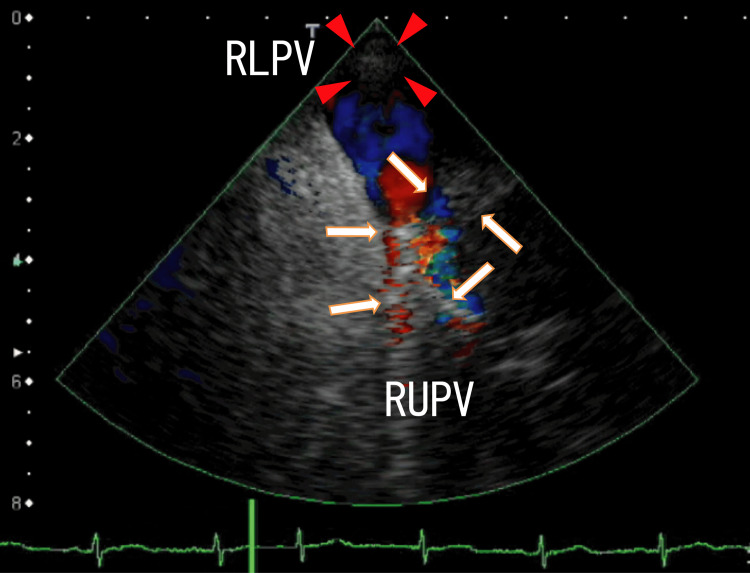 Figure 3
Figure 3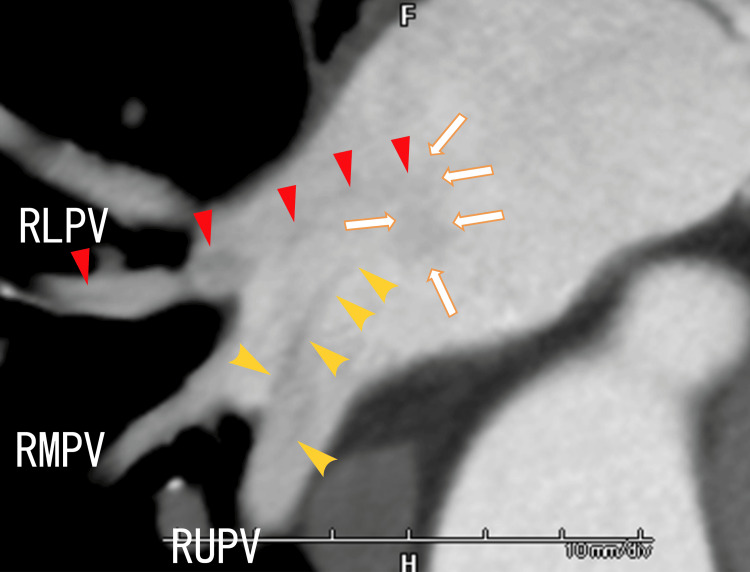 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac tumors and thrombi · Venous Thromboembolism Diagnosis and Management · Atrial Fibrillation Management and Outcomes
Introduction
Research on thrombi retrieved from patients with ischemic stroke (IS) and acute myocardial infarction (AMI) has shown that the retrieved thrombi are calcified in some patients [1-4], which means that the retrieved thrombi are old. The retrieved thrombi existed before the occurrence of the IS and AMI. We reported that pulmonary vein thrombi (PVTs) are common [5,6] and can cause IS and AMI through the emission of large particles [7,8]. Understanding the characteristics of PVTs is important for preventing IS and AMI. We reported several cases of PVTs using cardiac computed tomography (CT) and transesophageal echocardiography (TEE) [9-13]. PVTs can release several sizes of particles. Large particles can cause IS and AMI, and small particles such as neutrophil extracellular traps (NETs) can be associated with acute coronary syndrome [14], heart failure [15], and type 2 diabetes mellitus (T2DM) [16]. Additionally, we reported that in many patients, PVTs form a network of PVTs in the left atrium (LA) [17], which was estimated using 64-slice multidetector computed tomography (64-MDCT). However, we cannot comprehensively understand the connecting mechanisms using only 64-MDCT. To our knowledge, this is the first report to show the details of the connections between the right upper pulmonary vein (RUPV) thrombi and the right lower pulmonary vein (RLPV) thrombi on the anterior wall of the LA using both TEE and 80-MDCT.
Case presentation
The patient was a 69-year-old female with hypertension. The patient had no history of IS or chest pain. Physical examination revealed no abnormalities. Electrocardiography revealed a normal sinus rhythm and no ST-T changes. The serum D-dimer level was 0.7 μg/mL (normal: <1.0 μg/mL), the activity of protein S was 84% (normal: 74%-132%), and the activity of protein C was 107% (normal: 64%-135%). Her homocysteine level was 11.4 nmol/mL (normal: 5-15 nmol/mL). Her serum brain natriuretic peptide (BNP) level was 18.8 pg/mL (normal: <18.4 pg/mL). We evaluated the PVTs using TEE and 80-slice multidetector computed tomography (80-MDCT).
TEE images showed that the LA thrombi that extended from the RLPV thrombi reached the anterior wall of the LA (Figure 1 and Video 1).
Transesophageal echocardiography (TEE) images showing that the left atrium (LA) thrombi extending from the right lower pulmonary vein (RLPV) thrombi reached the anterior wall of the LA.The arrows indicate the LA thrombi, around which there may be some whitish thrombi. The arrowheads indicate possible walls of the LA. The LA walls had no clear margin; therefore, we hypothesized that there were some thrombi on the LA walls.LLPV, left lower pulmonary vein; LUPV, left upper pulmonary vein; RUPV, right upper pulmonary vein
The video representation of Figure 1.The LA thrombi extending from the RLPV thrombi periodically moved with the heartbeats. The anterior wall of the LA was not smooth, and there were some thrombi, including larger white parts on the anterior wall, which periodically moved with the heartbeats. The LA thrombi extending from the RLPV thrombi had small areas with white shadows, indicating that some of the thrombi were calcified.LA, left atrium; RLPV, right lower pulmonary vein
Additionally, TEE images showed that other LA thrombi are connected around the exit of the RUPV and the anterior wall of the LA (Figure 2 and Video 2).
TEE images showed that the LA thrombi extended from the right upper pulmonary vein (RUPV) and reached the anterior wall of the LA.The arrows indicate white LA thrombi, which are connected around the exit of the RUPV and the anterior wall of the LA. The arrowheads indicate the attachment regions of the LA wall, which are near the RLPV thrombus attachment regions.RLPV, right lower pulmonary vein; LA, left atrium; TEE, transesophageal echocardiography
The video representation of Figure 2.The LA thrombi extending from the RUPV thrombi periodically moved with the heartbeats. The LA thrombi had several small, darker thrombi, which are connected around the thrombi. The LA thrombi had no areas with white shadows. Small red areas sometimes appeared on the left side of the attachment regions, which indicated blood flow from the left upper pulmonary vein (LUPV).LA, left atrium; RUPV, right upper pulmonary vein
Moreover, TEE images showed that the thrombi in the RUPV had two branches: one from the right side and the other from the left side (Figure 3 and Video 3).
TEE images showing the RUPV thrombi.The arrows indicate the RUPV thrombi, which had two branches. One branch was directed to the left, and the other branch was directed to the right. The LA side of the RUPV thrombi was attached to the left side of the surrounding wall of the exit of the RUPV. In the RUPV, there was a mixture of red, blue, and yellow colors, indicating that there were disturbances in blood flow. The arrowheads indicate the LA thrombi situated around the exit of the RLPV.RLPV, right lower pulmonary vein; RUPV, right upper pulmonary vein; LA, left atrium; TEE, transesophageal echocardiography
Video representation of Figure 3.The thrombi in the RUPV did not periodically move substantially. The thrombi in the RUPV had no white shadows, but the thrombi had several small, darker thrombi connected to the thrombi. The LA thrombi situated around the exit of the RLPV periodically moved while breathing rather than the heartbeats.LA, left atrium; RUPV, right upper pulmonary vein; RLPV, right lower pulmonary vein
Oblique 80-MDCT revealed two LA thrombi extending from the RLPV and RUPV thrombi and attachment regions on the LA wall (Figure 4).
Oblique 80-slice multidetector computed tomography (80-MDCT) images showing thrombi in the right pulmonary veins and the LA.This angle was similar to the angle used for TEE. The yellow arrowheads indicate white LA thrombi extending from the RLPV thrombi, which resemble the white lines depicted using TEE. The red arrowheads indicate the LA thrombi extending from the RUPV thrombi, which resemble white lines with rough surfaces according to TEE. The arrows indicate the attachment areas of both the RUPV thrombi and the RLPV thrombi. There were two right middle pulmonary veins (RMPVs) between the RUPV and RLPV.RLPV, right lower pulmonary vein; RUPV, right upper pulmonary vein; LA, left atrium; TEE, transesophageal echocardiography
Two thrombi in the LA that extended from the RUPV and RLPV were rather clearly demonstrated using 80-MDCT. The RLPV and RUPV thrombi extended into the LA and reached the nearby region of the LA anterior wall, which was situated on the left-side anterior wall of the exit of the LUPV. The two thrombi looked to be combined on the LA wall, because they had other thrombi around them, which was depicted using both TEE and 80-MDCT (Figure 1, Figure 2, Figure 4, Video 1, and Video 2).
Discussion
To our knowledge, this is the first report to show the connection between the RLPV thrombi and the RUPV thrombi on the LA anterior wall using both TEE and 80-MDCT.
In our previous studies, the LA thrombi extending from the RLPV thrombi could not be depicted using 80-MDCT [9]; however, in the present case, 80-MDCT revealed that the LA thrombi extended from the RLPV and RUPV thrombi (Figure 4). Additionally, in the present case, 80-MDCT revealed large thrombi, which were depicted as weakly whitish thrombi formed around white linear thrombi using TEE. The cause of these differences when LA thrombi are depicted in 80-MDCT images is unknown.
To our knowledge, this is the first report to show that on TEE, the RUPV thrombi diverged in the right and left directions (Figure 3). Similarly, using 64-MDCT, we previously reported that thrombi in small vessels became increasingly larger and came into the larger-diameter pulmonary vein near the LA [18]. Then, pulmonary vein thrombi extended into the LA and attached to the LA wall, which was detected using 64-MDCT and transthoracic echocardiography (TTE) [9,19]. In the present case, two narrow pulmonary vein thrombi combined into larger RUPV thrombi, which were first described in detail using TEE (Figure 3).
More closely, we noticed that the white RLPV thrombi had small white parts with white shadows, indicating that the LA thrombi extending from the RLPV thrombi had calcified parts; however, the white RUPV thrombi and the white LA thrombi extending from the RUPV had no parts with white shadows. To our knowledge, these findings are the first to be described. In our previous case report, we showed that the LA thrombi extending from the RLPV thrombi, which are located around the exit of the RUPV, had small particles with shadows [13]. The LA thrombi extending from the RUPV thrombi might have no parts with shadows. More studies are needed to clarify these mechanisms.
When pulmonary infection occurs, NETs are produced from neutrophils to kill pathogens. NETs form arterial thrombi in the pulmonary vein to prevent the spread of pathogens to all organs [20]. Then, the information about the pathogens was closed there locationally. When the same pathogen attacks the other side of the lung, antibodies cannot be produced quickly. All lungs should have information on invading pathogens. Leukocytes on PVTs might be connected to transmit pathogen information to the PVTs; therefore, PVTs need to make networks to respond quickly and correctly. Therefore, the RUPV thrombi and the RLPV thrombi combine to form a scaffold for leukocytes. PVTs are naturally related to infections because of their origin. When we think about infection including COVID-19, we need to examine leukocytes on PVTs. More research is required to clarify these relationships.
Conclusions
The RLPV and RUPV thrombi extended into the LA and reached the near regions on the anterior wall of the LA. They looked to be linked.
The white linear LA thrombi assessed using TEE were depicted as darker linear areas than the surrounding thrombi when they were depicted using 80-MDCT. We might pay attention to leukocytes on PVTs when we think of any infections.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Calcification and endothelialization of thrombi in acute stroke Ann Neurol Almekhlafi MA Hu WY Hill MD Auer RN 3443486420081857029810.1002/ana.21404 · doi ↗ · pubmed ↗
- 2Unusual histopathological findings in mechanically removed stroke thrombi - a multicenter experience Front Neurol Aspegren O Staessens S Vandelanotte S 8462931320223566505210.3389/fneur.2022.846293 PMC 9157388 · doi ↗ · pubmed ↗
- 3Non contrast enhanced volumetric histology of blood clots through high resolution propagation-based X-ray microtomography Sci Rep Saghamanesh S Dumitriu La Grange D Reymond P Wanke I Lövblad KO Neels A Zboray R 27781220223517776710.1038/s 41598-022-06623-8PMC 8854637 · doi ↗ · pubmed ↗
- 4Histopathologic analysis of retrieved cerebral thrombi in acute ischemic stroke patients with proximal anterior circulation occlusions amenable to endovascular thrombectomy J Neurol Sci Mak G Lu JQ Perera K 11761742920213446155110.1016/j.jns.2021.117617 · doi ↗ · pubmed ↗
- 5Retracted: poster no. 119 large arterial thrombi in the pulmonary vein are common in elderly subjects and may cause age-related disease by producing neutrophil extracellular traps Cardiovasc Res Takeuchi H 821182022
- 6Nearly all left atrial thrombi may be extended from pulmonary vein thrombi Int J Cardiol Heart Vasc Takeuchi H 9720152878563710.1016/j.ijcha.2015.01.013PMC 5497179 · doi ↗ · pubmed ↗
- 7Mechanical thrombectomy for acute ischemic stroke arising from thrombus of the left superior pulmonary vein stump after left pneumonectomy: a case report NMC Case Rep J Sonobe S Yoshida M Niizuma K Tominaga T 1720620193070115010.2176/nmccrj.cr.2018-0163 PMC 6350028 · doi ↗ · pubmed ↗
- 8Mechanical thrombectomy for acute ischemic stroke due to thrombus in the pulmonary vein stump after left pulmonary lobectomy: a case series Neurointervention Tsuji Y Yagi R Hiramatsu R Wanibuchi M 1681731720223617761010.5469/neuroint.2022.00367 PMC 9626613 · doi ↗ · pubmed ↗