Critical appraisal of a non-invasive model to derive pulmonary capillary wedge pressure from cardiac magnetic resonance in heart failure patients: insights from a large Portuguese Observational Study
Sérgio Maltês, Mariana Sousa Paiva, Rita Reis Santos, Bruno M L Rocha, Gonçalo J L Cunha, Cláudia Silva, Sara Guerreiro, Pedro Freitas, João Abecasis, António M Ferreira

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
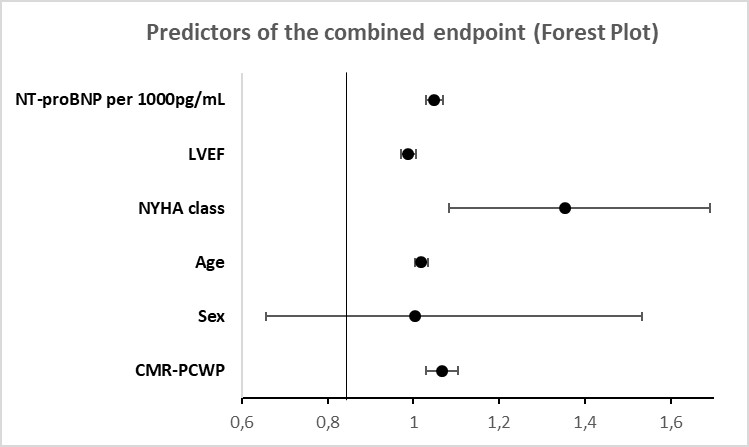 Figure 1
Figure 1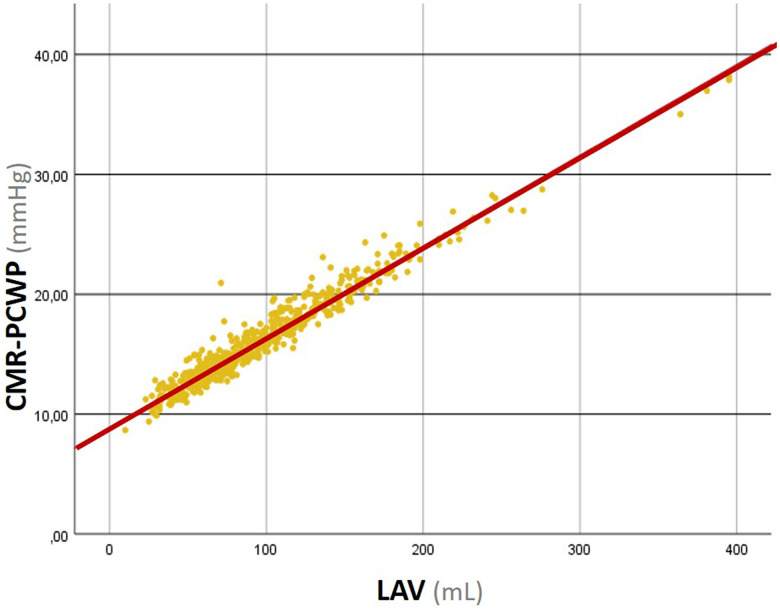 Figure 2
Figure 2 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Function and Risk Factors · Advanced MRI Techniques and Applications · Cardiac Imaging and Diagnostics
Increased left ventricular (LV) filling pressure (LVFP) is a hallmark of heart failure (HF), with significant prognostic implications.^1^ Currently, pulmonary capillary wedge pressure (PCWP), measured by right heart catheterization (RHC), remains the main metric for assessing LVFP. However, RHC is an invasive procedure, with limited availability and low but non-negligible risks. Transthoracic echocardiography has potential as an alternative, but diastolic dysfunction assessment can be challenging, relying on multiple echocardiographic parameters and operator expertise.
Cardiac magnetic resonance (CMR) is increasingly used to evaluate HF patients, but the haemodynamic information it provides is somewhat limited. Recently, Garg et al.^2^ proposed a physiological model to estimate PCWP from CMR data (CMR-PCWP). In a cohort of more than 800 patients referred for dyspnoea assessment [of whom only 7% had reduced or mid-range left ventricular ejection fraction (LVEF)], the authors were able to derive a model to estimate PCWP through CMR (CMR-PCWP) using two simple measurements: left ventricle mass (LVM) and left atrial volume (LAV). They found a correlation between CMR-PCWP and RHC-PCWP. Moreover, elevated CMR-PCWP had significant prognostic implications.
To determine whether those findings translate to HF with reduced ejection fraction, we conducted a retrospective cohort study of 578 consecutive patients with LVEF <50% who underwent CMR at our centre between 2015 and 2022 (mean age 63 ± 14 years, 72% male, mean LVEF 34 ± 10%, 45% ischaemic aetiology). Standard LVM and LAV measurements were used to calculate CMR-PCWP as per the proposed model. Overall, the mean CMR-PCWP was 16 ± 4 mmHg, with 298 patients (52%) showing values ≥15 mmHg. Patients with elevated CMR-PCWP were significantly older, had lower LVEF and right ventricle ejection fraction, higher ventricular volumes and higher lung water density values, a novel prognostic marker in HF.^3^ During a median follow-up of 25 (13–51) months, 69 deaths and 72 HF hospitalizations were observed. A multivariate Cox regression analysis was performed after univariate analysis to identify which variables predicted a combined endpoint of all-cause death or HF hospitalization. At multivariate analysis, CMR-PCWP proved to be an independent predictor of the combined endpoint [hazard ratio (HR) 1.067, 95% confidence interval (CI) 1.029–1.105, P < 0.001; adjusted for age, sex, New York Heart Association class, LVEF and NT-proBNP, supplementary data online, Figure S1]. However, we also found a very strong correlation between CMR-PCWP and LAV, with 95% of the variance of CMR-PCWP explained by LAV (R^2^ = 0.947, Figure 1). Furthermore, CMR-PCWP variance was only mildly determined by LVM (R^2^ = 0.178). While LVM showed a lower predictive power at multivariate analysis (HR 1.044 per 10 g, 95% CI 0.998–1.092, P = 0.061, χ^2^ 8094), both LAV and CMR-PCWP had a similar discriminative capability in predicting the combined endpoint (LAV—HR 1.047 per 10 mL, 95% CI 1.019–1.075, P = 0.001, χ^2^ 36 470; CMR-PCWP—HR 1.067, 95% CI 1.029–1.105, χ^2^ 38 951; C-statistic 0.67 vs. 0.67, P-value for comparison = 0.724). Moreover, the CMR-PCWP model did not improve LAV performance in predicting the combined endpoint (Net Reclassification Index 0.04, P-value 0.244).
Our findings suggest that in HF patients with LVEF <50%, the proposed CMR-PCWP model might be a mere surrogate of LAV. In our cohort, we were not able to find additional diagnostic or prognostic information on the CMR-PCWP model over other already established CMR measurements. However, it should be highlighted that the original purpose of the CMR-PCWP model (unexplained dyspnoea) is different from the setting where it was tested in our cohort.
Future studies must attempt to further refine the CMR-PCWP model and determine how it compares to other novel CMR-derived metrics in HF, such as pulmonary transit time and pulmonary blood volume analysis.^4,5^ As it stands, the search must continue for different CMR markers of diastolic dysfunction and increased LVFP in HF patients.
Supplementary Material
qyad017_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Pinamonti B, Di Lenarda A, Sinagra G, Camerini F. Restrictive left ventricular filling pattern in dilated cardiomyopathy assessed by Doppler echocardiography: clinical, echocardiographic and hemodynamic correlations and prognostic implications. Heart Muscle Disease Study Group. J Am Coll Cardiol 1993;22:808–15.8354816 10.1016/0735-1097(93)90195-7 · doi ↗ · pubmed ↗
- 2Garg P, Gosling R, Swoboda P, Jones R, Rothman A, Wild JM et al Cardiac magnetic resonance identifies raised left ventricular filling pressure: prognostic implications. Eur Heart J 2022;43:2511–22.35512290 10.1093/eurheartj/ehac 207PMC 9259376 · doi ↗ · pubmed ↗
- 3Rocha BML, Cunha GJL, Freitas P, Lopes PMD, Santos AC, Guerreiro S et al Measuring lung water adds prognostic value in heart failure patients undergoing cardiac magnetic resonance. Sci Rep 2021;11:20162.34635767 10.1038/s 41598-021-99816-6PMC 8505633 · doi ↗ · pubmed ↗
- 4Ricci F, Barison A, Todiere G, Mantini C, Cotroneo AR, Emdin M et al Prognostic value of pulmonary blood volume by first-pass contrast-enhanced CMR in heart failure outpatients: the PROVE-HF study. Eur Heart J Cardiovasc Imaging 2018;19:896–904.29045598 10.1093/ehjci/jex 214 · doi ↗ · pubmed ↗
- 5Houard L, Amzulescu MS, Colin G, Langet H, Militaru S, Rousseau MF et al Prognostic value of pulmonary transit time by cardiac magnetic resonance on mortality and heart failure hospitalization in patients with advanced heart failure and reduced ejection fraction. Circ Cardiovasc Imaging 2021;14:e 011680.33438438 10.1161/CIRCIMAGING.120.011680 · doi ↗ · pubmed ↗