Absence of long-term structural and functional cardiac abnormalities on multimodality imaging in a multi-ethnic group of COVID-19 survivors from the early stage of the pandemic
Lorenzo R Sewanan, Marco R Di Tullio, Andrew F Laine, Belinda D’Souza, Jay Leb, Alexander Mironov, Ahsan Khan, Dylan E Stanger, Elisa E Konofagou, Rochelle L Goldsmith, Sachin R Jambawalikar, Cole B Hirschfeld, Michelle Castillo, Kathleen J Durkin, Stephen Dashnaw

TL;DR
This study found no long-term heart damage in a diverse group of people who survived early-stage COVID-19.
Contribution
The study provides evidence that early-stage COVID-19 does not cause lasting cardiac abnormalities in a multi-ethnic survivor cohort.
Findings
No differences in echocardiographic measures of heart structure and function between survivors and controls.
CMR showed no significant differences in tissue structure or inflammation markers in survivors.
Results were consistent regardless of hospitalization status during initial infection.
Abstract
Many patients with coronavirus disease-2019 (COVID-19), particularly from the pandemic’s early phase, have been reported to have evidence of cardiac injury such as cardiac symptoms, troponinaemia, or imaging or ECG abnormalities during their acute course. Cardiac magnetic resonance (CMR) and transthoracic echocardiography (TTE) have been widely used to assess cardiac function and structure and characterize myocardial tissue during COVID-19 with report of numerous abnormalities. Overall, findings have varied, and long-term impact of COVID-19 on the heart needs further elucidation. We performed TTE and 3 T CMR in survivors of the initial stage of the pandemic without pre-existing cardiac disease and matched controls at long-term follow-up a median of 308 days after initial infection. Study population consisted of 40 COVID-19 survivors (50% female, 28% Black, and 48% Hispanic) and 12…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1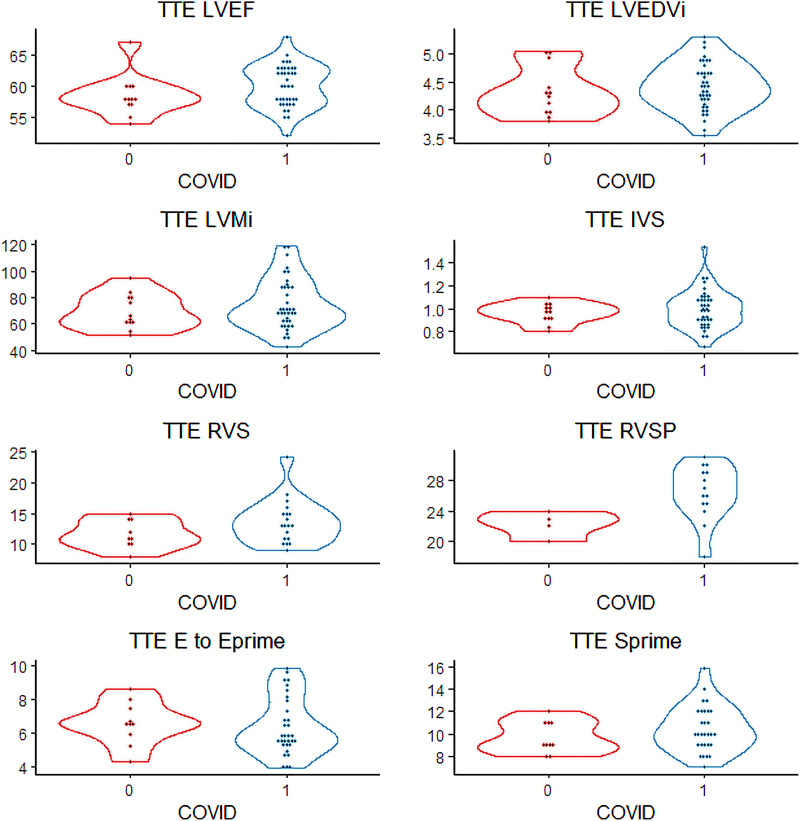 Figure 2
Figure 2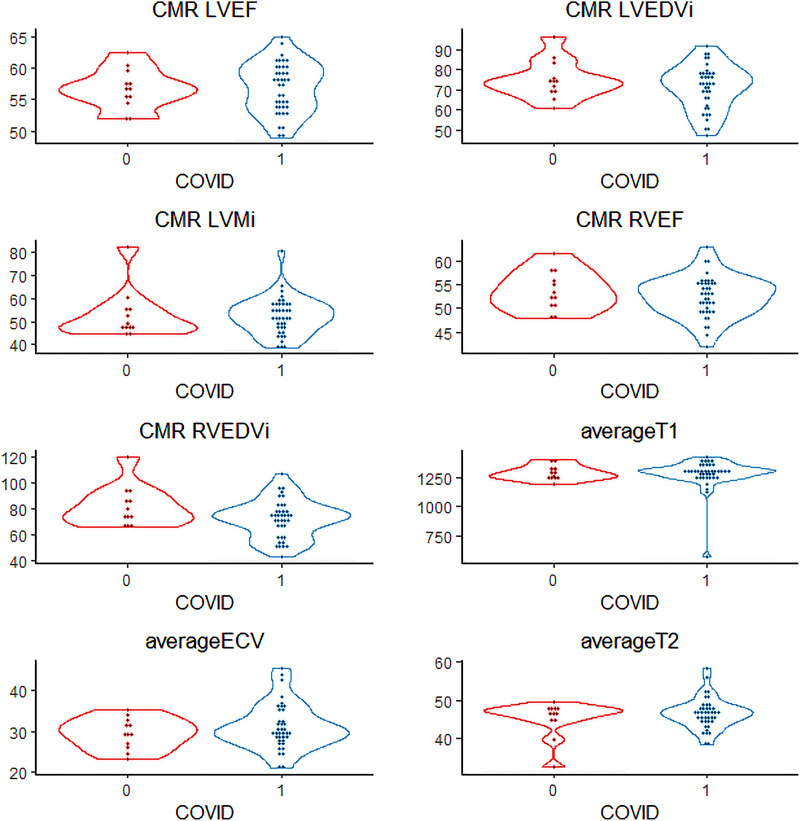 Figure 3
Figure 3| COVID-19 negative ( | COVID-19 positive ( | ||
|---|---|---|---|
| Time from diagnosis to scan (days) | N/A | 308 (225–391) | N/A |
| Baseline characteristics | |||
| Age (years) | 40 (27–55) | 46 (34–65) | 0.17 |
| Female | 6 (50%) | 20 (50%) | 1 |
| Body mass index | 26 (24–31) | 27 (24–32) | 0.59 |
| White | 7 (58%) | 18 (45%) | 0.32 |
| Black | 3 (25%) | 11 (28%) | 0.32 |
| Hispanic | 5 (42%) | 19 (48%) | 0.28 |
| High-sensitivity Troponin-T | 6.5 (5–14) | 5.5 (5–11) | 0.76 |
| D-Dimer | 0.15 (0–0.4) | 0.37 (0–0.6) | 0.07 |
| Past medical history | |||
| Atrial fibrillation | 0 (0%) | 0 (0%) | — |
| Chronic kidney disease | 0 (0%) | 0 (0%) | — |
| Chronic obstructive pulmonary disease | 0 (0%) | 0 (0%) | — |
| Coronary artery disease | 0 (0%) | 2 (5%) | — |
| Diabetes | 0 (0%) | 7 (18%) | 0.28 |
| Heart failure | 0 (0%) | 0 (0%) | — |
| Hypertension | 0 (0%) | 10 (25%) | 0.13 |
| Valvular disease | 0 (0%) | 0 (0%) | — |
| Prior myocardial infarction | 0 (0%) | 2 (5%) | 1 |
| COVID symptoms | |||
| Fever | N/A | 27 (68%) | N/A |
| Chest pain | N/A | 11 (28%) | N/A |
| Dyspnoea | N/A | 23 (57.5%) | N/A |
| Myocarditis | N/A | 1 (2.5%) | N/A |
| Hospitalized | N/A | 14 (35%) | N/A |
| Intubated | N/A | 7 (17.5%) | N/A |
| Post-COVID symptoms | |||
| Chest pain | N/A | 2 (5%) | N/A |
| Dyspnoea | N/A | 7 (17.5%) | N/A |
| Palpitations | N/A | 4 (10%) | N/A |
| COVID-19 negative ( | COVID-19 positive ( | ||
|---|---|---|---|
| LVEF (%) | 58 (57–60) | 60 (54–63) | 0.13 |
| LVEDd (cm) | 4.30 (4–4.5) | 4.40 (4.1–4.7) | 0.44 |
| LVESd (cm) | 3.14 (2.9–3.2) | 3.00 (2.9–3.3) | 0.87 |
| IVS (cm) | 0.98 (0.92–1.02) | 0.99 (0.9–1.1) | 0.70 |
| PW (cm) | 0.95 (0.87–1.03) | 0.94 (0.86–1.00) | 0.66 |
| LV mass index (g/m2) | 69.3 (61–80) | 64.4 (61–88) | 0.45 |
| WMA | 0 (0) | 0 (0) | — |
| LV S′ (cm/s) | 9.0 (9–11) | 10.0 (9–12) | 0.31 |
| LA diameter (cm) | 3.3 (3.2–3.8) | 3.4 (3.2–3.9) | 0.63 |
| 73 (68–77) | 71 (61–78) | 0.32 | |
| 61 (50–76) | 64 (51–71) | 0.95 | |
| 1.34 (1.01–1.51) | 1.14 (0.82–1.44) | 0.34 | |
| 11.5 (10–13) | 12.0 (10–15) | 0.92 | |
| 6.60 (6–7.2) | 5.78 (5.3–7.4) | 0.35 | |
| RV enlargement | 4 (33) | 4 (11) | 0.15 |
| RV S′ (cm/s) | 11 (11–14) | 13 (11–15) | 0.17 |
| RV dysfunction | 1 (8) | 0 (0) | 0.54 |
| RVSP (mmHg) | 22.5 (22–23) | 26.5 (25–29) | 0.03 |
| RA enlargement | 3 (25) | 1 (3) | 0.08 |
| Pericardial effusion | 1 (8.3) | 2 (5.1) | 1 |
| Non-hospitalized ( | Hospitalized ( | ||
|---|---|---|---|
| LVEF (%) | 60 (58–62) | 60 (57–63) | 0.62 |
| LVEDd (cm) | 4.35 (4.1–4.7) | 4.50 (4.2–4.6) | 0.73 |
| LVESd (cm) | 2.98 (2.84–3.29) | 3.19 (2.91–3.35) | 0.52 |
| IVS (cm) | 0.91 (0.84–1.06) | 1.06 (1.00–1.11) | 0.02 |
| PW (cm) | 0.90 (0.84–0.98) | 0.99 (0.91–1.10) | 0.04 |
| LV mass index (g/m2) | 68.7 (62–82) | 69.9 (62–92) | 0.79 |
| WMA | 0 (0) | 0 (0) | — |
| LV S′ (cm/s) | 10.0 (9–12) | 10.0 (8.5–11.5) | 0.33 |
| LA diameter (cm) | 3.26 (3.00–3.56) | 3.83 (3.77–4.06) | 0.002 |
| 73 (69–80) | 61 (55–70) | 0.007 | |
| 62 (51–66) | 70 (66–77) | 0.03 | |
| 1.29 (1.06–1.52) | 0.81 (0.78–1.02) | 0.002 | |
| 12.5 (10–15) | 11.0 (9.5–13.5) | 0.40 | |
| 5.78 (5.4–8.1) | 5.73 (5–6.3) | 0.47 | |
| RV enlargement | 2 (8) | 2 (15) | 0.88 |
| RV S′ (cm/s) | 14 (13–15) | 11 (10–13) | 0.07 |
| RV dysfunction | 0 (0) | 0 (0) | — |
| RVSP (mmHg) | 25.5 (24–27) | 30.0 (29.5–30.3) | 0.011 |
| RA enlargement | 1 (4) | 0 (0) | 1 |
| Pericardial effusion | 2 (7.7) | 0 (0) | 0.79 |
| COVID-19 negative ( | COVID-19 positive ( | ||
|---|---|---|---|
| LVEF (%) | 57 (55–58) | 58 (54–60) | 0.78 |
| LVEDV index | 74 (70–78) | 74 (63–78) | 0.28 |
| LV mass index | 49 (51–57) | 52 (48–57) | 0.77 |
| Wall motion abnormality | 0 (0) | 0 (0) | — |
| RVEF (%) | 53 (51–57) | 53 (50–55) | 0.35 |
| RVEDV index | 78 (72–88) | 74 (61–78) | 0.12 |
| Pericardial effusion | 0 (0) | 1 (3) | 1 |
| T1 (ms) | 1278 (1250–1325) | 1306 (1254–1327) | 0.56 |
| T2 (ms) | 47 (45–48) | 47 (45–48) | 0.90 |
| ECV | 29 (27–31) | 30 (28–34) | 0.44 |
| LGE | 0 (0) | 1 (3) | 1 |
| Non-hospitalized ( | Hospitalized ( | ||
|---|---|---|---|
| LVEF (%) | 59 (55–60) | 54 (53–58) | 0.12 |
| LVEDV index | 74 (65–78) | 70 (60–75) | 0.29 |
| LV mass index | 54.7 (47–58) | 51.0 (50–54) | 0.11 |
| Wall motion abnormality | 0 (0) | 0 (0) | — |
| RVEF (%) | 54.3 (51–55) | 51 (49–53) | 0.11 |
| RVEDV index | 75.5 (67–82) | 71.5 (58–76) | 0.20 |
| Pericardial effusion | 1 (4) | 0 (0) | 1 |
| T1 (ms) | 1306 (1250–1319) | 1305 (1267–1351) | 0.41 |
| T2 (ms) | 46.7 (45–49) | 45.8 (42–48) | 0.23 |
| ECV | 30.4 (29–36) | 28.2 (27–31) | 0.08 |
| LGE | 0 (0) | 1 (11) | 0.59 |
| Modality | Variable | COVID | Value | Average value |
|---|---|---|---|---|
| TTE | IVS (cm) | Case | 1.54 | 0.99 |
| TTE | LVEF (%) | Control | 67 | 58 |
| TTE | Control | 111 | 73 | |
| CMR | LVMi | Case | 80.6 | 52 |
| CMR | T1 (ms) | Case | 572 | 1306 |
| CMR | LVMi | Control | 82.3 | 49 |
| CMR | RVEDVi | Control | 119 | 78 |
| CMR | T2 (ms) | Control | 32.6 | 47 |
| CMR | T2 (ms) | Control | 39.9 | 47 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Disease and Adiposity · Cardiovascular Effects of Exercise · COVID-19 Clinical Research Studies
Introduction
The ongoing global coronavirus disease-2019 (COVID-19) pandemic causes a spectrum of disease, from asymptomatic and mild infections to severe multisystem failure. The SARS-CoV-2 respiratory virus is able to cause severe inflammatory phenomena that impact many organ systems beyond the lungs, including neurologic, cardiovascular, and renal manifestations. Many patients have been reported to present with or develop markers of cardiac injury such as troponinaemia, electrocardiographic changes, cardiovascular symptoms, and echocardiographic abnormalities during their acute course of disease.^1,2^ Such acute cardiac disease manifestations in the setting of COVID-19 range from myocarditis, pericarditis, Takutsubo cardiomyopathy, ischaemia, and arrhythmia in the setting of systemic inflammation.^1–12^ Transthoracic echocardiography (TTE) has been widely used to assess cardiac function and structure during COVID-19 due to ease of access during acute illness and follow-up, with numerous reports of abnormalities. Cardiac magnetic resonance (CMR) has been particularly useful in complementing TTE for further assessment of tissue structure.^13–15^ Overall, findings are varied,^1,2,5–8,13–42^ and long-term impact of COVID-19 on myocardial structure and function needs further elucidation to characterize whether the myocardial inflammation is truly transient or could act as a substrate for development of long-term cardiac dysfunction and adverse remodelling. In our study, we performed transthoracic echocardiography (TTE) and CMR in COVID-19 patients and controls from the early phase of the pandemic at a long-term follow-up of at least 6 months post-infection, using an array of CMR techniques to comprehensively evaluate the myocardium, so as to fully appreciate potential deleterious consequences of COVID-19 on the heart.
Methods
In order to conduct this study, we recruited patients and controls from the general population of Columbia University Irving Medical Center (CUIMC)/New York-Presbyterian Hospital during the early months of 2021. Specifically, we recruited patients who had been seen at CUIMC who met the following inclusion criteria; convalescent COVID-19 patient (at least 4 weeks after symptoms and 2 weeks after hospital discharge if hospitalized), ability to give informed consent, willingness to undergo CMR and TTE, ability to perform 15 s breathe hold, and age 18 or older. These patients were not specifically planned to undergo cardiac testing and further cardiac imaging. Patients self-enrolled in the study after being contacted from a local database platform of subjects interested in clinical trial participation. We excluded patients who were pregnant, had chronic kidney disease stage 4 with estimated glomerular filtration ratio <30, incarcerated, known allergy to gadoterate, contraindication to CMR, known history of obstructive coronary artery disease with stenosis > 70% or fractional flow reserve <0.8, history of congestive heart failure prior to COVID-19, and severe valvular heart disease. We specifically aimed to enrol patients who did not have indications for cardiac magnetic resonance imaging (MRI) otherwise, in comparison to prior studies of unselected patients. For healthy controls, we ensure that they had no prior COVID, by asking to report prior COVID testing, medical records, and present proof of negative PCR/serology. The study protocol was approved by the institutional review board of our institution (IRB #AAAT0787). Informed consent was obtained from all patients.
We collected information on all subjects and patients including demographics, biometrics, presenting symptoms, any ongoing symptoms at time of testing, past medical history, and drew blood work for d-dimer, troponin, and haematocrit. We performed CMR in all recruited patients and TTE in all but one recruited patient due to the patient being lost to follow-up.
Transthoracic echocardiograms were performed using a commercially available system (iE 33, Philips, Andover, MA, USA) by an experienced cardiac sonographer or by a trained advanced imaging cardiology fellow blinded to the participant’s clinical information, following a standardized protocol. Tests were interpreted by a single experienced reader blinded to the subject’s clinical information. The dimensions of the cardiac chambers were measured according to the recommendations of the American Society of Echocardiography.^43^ Left ventricular ejection fraction (LVEF) was calculated using the modified biplane Simpson’s rule or visual estimation when appropriate. Left ventricular (LV) mass was calculated with a validated method and indexed for body surface area to generate LV mass index.^44^ LV diastolic function was assessed by combined spectral Doppler (E wave and A wave) and annular tissue Doppler (E′) evaluation; tissue Doppler S′ (systolic) annular velocities were measured as additional parameters of LV and right venticular (RV) systolic function. Echocardiographic variables of interest included indices of LV morphology, systolic and diastolic function; presence of valve disease; right ventricular dimension and function; left atrial and right atrial dimensions; presence of pericardial effusion.
We performed CMR using a 3T SIGNA™ Premier scanner (general electric [GE] HealthCare, Waukesha, WI, USA) with gadoterate meglumine (Clariscan, GE HealthCare) and using a 30-channel AIR Anterior coil and embedded Posterior coil (GE HealthCare). We performed functional assessment using a balanced Steady State Free Precession cine sequence for left ventricular and right ventricular (RV) function. Myocardial characterization was performed using T2-weighted imaging with double inversion recovery fast spin echo (FSE), T1 mapping using native modified Look Locker inversion (MOLLI-5(3)3) recovery sequence, gadolinium enhanced T1 mapping using MOLLI-4(1)3(1)2 and extracellular volume (ECV) fraction assessment, T2 mapping using a multi-echo FSE sequence, and late gadolinium enhancement (LGE) with phase-sensitive inversion recovery. CMR analysis was performed using cvi v5.11 (Circle Cardiovascular Imaging, Calgary). LGE was performed approximately 10 min after gadoterate injection. For extracellular volume measurements, post-contrast T1 mapping was performed >10 min after contrast injection based on Society for Cardiovascular Magnetic Resonance protocol recommendations.^45^
Each CMR study was read and processed independently by two trained expert cardiac radiologists with sub-specialization in cardiothoracic imaging and approximately 6 and 16 years each of experience independently reading studies. Parametric mapping was performed using regions of interest in the basal, mid-ventricular, and apical septa and averaged. ECV was calculated using the standard formula, specifically
CMR measurements included the following: left ventricular ejection fraction (LVEF), left ventricular end-diastolic volume index (LVEDVi), left ventricular mass index (LVMi), right ventricular ejection fraction (RVEF), right ventricular end diastolic volume index (RVEDVi), T1 mapping, T2 mapping, and extracellular volume fraction (ECV). In the final analysis, we averaged together quantitative variables except when the variables were more than 15% discrepant. When there were discrepant readings for qualitative and quantitative variables, we conducted an arbitration process in which a third independent reader with 16 years of experience met with the two original readers to decide upon a consensus read. In this way, final values for all variables across study population were determined.
Basic statistical analysis was carried out in R 1.4.1717. We performed univariate Student’s t-tests for continuous and χ^2^ tests for categorical variables. P < 0.05 was considered significant. Tests of normality were performed, and if data were distributed non-normally, the Kruskal–Wallis test was used for continuous variables. Rosner’s generalized extreme Studentized deviate test for outliers was performed with an alpha of 0.05 (allowable Type 1 error) and k of 3 (assumed number of outliers to assess for statistically significant outliers in the data set stratified by case and control). Violin plots were also generated for assessment of outliers and distribution, which show the data points within the outline of the distribution of the data displayed vertically on each axis.
Results
We recruited a total of 52 participants for our study population, including 40 COVID-19 cases and 12 healthy controls (Table 1). Cases and controls were closely matched in age (median 46 vs. 40), sex (50% male), body mass index (median 27 vs. 26), and ethnicity (58% white, 25% Black) with 42% identifying as Hispanic ethnicity, without significant difference between these two subgroups. In general, these patients did not have substantial past medical history especially with regard to pre-existing cardiovascular disease. The presenting symptoms of the COVID patients were predominantly fever and dyspnoea although some also presented with chest pain. One patient self-identified themselves as having possible inflammation of the heart muscle, but this patient was not hospitalized for myocarditis, did not have imaging suggestive of this at the time of COVID, did not receive treatment for myocarditis, and has no proven diagnosis of myocarditis. Fourteen of the COVID-19 patients (35%) had illness requiring hospitalization, and seven (17.5%) of them had required intubation. At the time of presentation, a minority of patients had been experiencing ongoing chest pain, dyspnoea, and palpitations. No patient presented with acute coronary syndrome, acute aortic syndrome, venous thromboembolic phenomenon, or fulminant myocarditis. At time of study participation with imaging and blood work, a median of 308 days had passed from the onset of symptomatic COVID-19 (Table 1). At the time of scanning, no significant difference was detected in high sensitivity troponin T assay or d-dimer measurement between cases and controls with both being within normal limits for the standard lab ranges. At time of presentation for COVID, given that most patients were not specifically recruited from the hospital or for cardiac injury, specific biomarkers are not available in most of these patients (see Supplementary data online, Table S1). Furthermore, few patients received specific treatments for COVID such as remdesivir, steroids, and tocilizumab given the early time point in the pandemic prior to evidence of such therapies being widely available.
On TTE measurements of cardiac function and structure, there were no significant differences in LVEF, left ventricular end-diastolic diameter, LV mass, or LV wall motion abnormalities between COVID-19 cases and controls (Table 2). There was no significant difference in left atrial diameter or markers of LV diastolic function such as the E/E′ ratio, and no significant difference in RV size, right atrial size, and RV function. However, slightly increased right ventricular systolic pressure was noted in COVID-19 patients compared to controls (median 26.5 vs. 22.5 mmHg, P = 0.03). No patient was found to have significant valvular disease. Echocardiographic findings stratified by non-hospitalized vs. hospitalized patients, as a marker of COVID-19 severity, are summarized in Table 3. While LVEF, LVEDd, LV mass, and segmental wall motion abnormalities were similar and normal between the groups, we did find a slightly increased thickness of interventricular septum thickness (IVS) (median 1.06 vs. 0.91 cm, P = 0.019) and larger left atrium (LA) diameter (median 3.26 vs. 3.83 mmHg, P = 0.002) between COVID-19 patients and controls. In terms of measures of diastolic dysfunction, as overall lower E (median 61 vs. 73, P = 0.007) and higher A (70 vs. 62, P = 0.03) was noted in COVID-19 survivors, though the E/E′ ratio was not significantly different and within normal limits for both groups (5.73 vs. 5.78, P = 0.47). Similar to the controls compared to the COVID-19 patients, RVSP was higher in the hospitalized COVID-19 group (30 vs. 25 mmHg, P = 0.01) with otherwise no significant differences in right atrial (RA) size, RV dysfunction, or valve disease.
CMR was performed not only at myocardial macrostructure and function but also extract measures of tissue microstructure. In comparing COVID-19 patients to controls (Table 4), we found overall no significant differences; in particular LVEF, left ventricular end-diastolic index, right ventricular ejection fraction, and right ventricular end-diastolic volume index were similar and no wall motion abnormalities were noted. One patient in the COVID-19 positive group was noted to have a mild pericardial effusion. On assessment of tissue microstructure, there was no significant difference in median T1 (1278 vs. 1306 ms), T2 (47 vs. 47 ms), and ECV fraction (29 vs. 30) between COVID cases and controls. In only one case was LGE observed, which involved only 1 of 17 segments, specifically the mid-myocardial basal inferior wall (Figure 1). This patient initially presented with fever and dyspnoea, was hospitalized, and intubated for respiratory failure, with no initial acute cardiac concerns identified, though he remained symptomatic with shortness of breath at the time of the study, albeit without requirement for long-term oxygen therapy. There was no significant difference in these parameters between hospitalized and non-hospitalized cases (Table 5). We generated distribution plots of key TTE and CMR parameters (Figures 2 and 3) and formal statistical testing with Rosner’s tests for outliers (Table 6). We found few outliers in both cases and controls overall.
Late gadolinium in cardiac magnetic resonance imaging scan of COVID-19 patient. Late gadolinium in the basal inferior wall in the only patient in the cohort with enhancement at 10 months post-hospitalization and intubation for COVID-19 This scan was performed using a 3T GE SIGNA™ Premier scanner with late gadolinium enhancement with phase-sensitive inversion recovery, obtained 10 min after administration of gadoterate meglumine (Clariscan, GE Healthcare). Arrow points to LGE.
Violin plots of transthoracic echocardiogram characteristics of COVID-19 patients vs. controls. Distribution of key echocardiographic characteristics between cases (1, blue) and controls (2, red) including LVEF, left ventricular ejection fraction; LVEDVi, left ventricular end diastolic volume index; LVMi, left ventricular mass index; IVS, interventricular septum thickness; RVS, right ventricular S; RVSP, right ventricular systolic pressure; E to E′, E to Eprime; S′, Sprime. These violin plots show data points within the outline of the distribution of the data plotted vertically.
Violin plots of cardiac magnetic resonance characteristics of COVID-19 patients vs. controls. Distribution of key CMR characteristics between cases (1, blue) and controls (2, red) including LVEF (left ventricular ejection fraction), LVEDVi (left ventricular end diastolic volume index), LVMi (left ventricular mass index), RVEF (right ventricular ejection fraction), RVEDVi (right ventricular end diastolic volume index), T1, T2, and extracellular volume fraction.
Discussion
In this cross-sectional study of a multi-ethnic cohort of patients recruited from the initial phase of the COVID-19 pandemic, comprehensive analysis of cardiac structure and function using multimodality imaging with transthoracic echocardiography and multi-sequence cardiac MRI reassuringly found no signs of clinically significant changes to the myocardium. Imaging was performed at least 6 months and on average 10 months after initial COVID-19 infection during the initial phase of the pandemic in patients who were not otherwise scheduled for TTE or CMR, allowing an examination of patients at a distinctly remote time point from initial presentation, one of the longest term studies in the literature at this time. Moreover, this study is unique in its inclusion of a multi-ethnic cohort, with a majority of participants being Hispanic and/or Black.
Our findings did suggest a slight but significant increase in pulmonary hypertension in COVID-19 patients, particularly those who were sicker. LA diameter and IVS thickness were also different, but it is unclear that these are clinically relevant. However, for these patients, it does not seem that these differences significantly impact RV and LV functions at this time interval of 10 months after initial illness.
In some ways, these findings are not expected given the previous literature, though findings have been varied. An important early study in the midst of the early pandemic by Puntmann et al.^5^ performed CMR prospectively in 100 patients including 33% hospitalized about 71 days after initial COVID infection. In this study of German patients, it was found that 78% of patients had ongoing myocardial inflammation independent of pre-existing condition, severity, and overall course of acute illness. Such findings in this and other studies^8,25,30,34^ at early time points after COVID-19 of weeks to months have raised concerns that ongoing myocardial inflammation and damage may have serious long-term complications for cardiovascular health of many COVID-19 patients. Such alarming early data motivated the need for ongoing longer term follow-up studies, such as the present study.
CMR has been used in just a few studies to characterize long-term myocardial consequences of COVID-19. Cassar et al.^16^ used CMR in combination with cardiopulmonary exercise testing to study COVID-19 patients who were admitted and had ongoing cardiopulmonary symptoms about 3–6 months after initial infection; in their cohort, they found little evidence of persistent myocardial abnormalities that correlated with patient symptoms. Hanneman et al.^24^ studied prospectively mostly mild COVID-19 patients about 2–4 months after initial infection using PET and CMR; in this cohort, they found that about 17% of patients had focal FDG-PET uptake that correlated with T1, T2, LGE on CMR with mildly worsened contractile function, and strain initially at 2 months which had subsequently resolved within 4 months at follow-up. Joy et al. performed a 6-month prospective case–control studies of health care workers who had predominantly asymptomatic and mild COVID, finding no abnormal markers of COVID infection on CMR.^22^ Li et al.^40^ published a prospective observational cohort at 5–6 months post-infection finding only one patient with LGE among 40 but identifying mildly elevated ECV and reduced global longitudinal strain in patients with moderate/severe COVID but not ongoing cardiac symptoms, demonstrating a subclinical manifestation of COVID-19. Tanacli et al.^46^ published a retrospective series of 32 patients with persistent cardiac symptoms about 5 months after initial COVID infection along with endomyocardial biopsy demonstrating that about 30% of these patients showed myocardial injury but only 9% meeting full Lake Louise criteria without any demonstrating true myocarditis on biopsy which was pursued in these patients.
We add to this literature by extending the time frame to over 10 months and including a multi-ethnic group of patients as seen here. Despite analysis of average tendencies and outliers, we do not detect specific differences in cases and controls at this time point. Overall, these data are reassuring that COVID-19 in a general population does not lead to significant cardiac damage and ongoing inflammation at this long-term follow-up. Significant differences may not have been found in our current study due to the longer time of follow-up after COVID infection and the focus on patients without presentation of acute cardiac illness. Given prior studies finding a high burden of findings in many patients during and soon after illness, it may be that there was transient myocardial involvement that had resolved at the time of this study, though longitudinal studies would be required to establish such findings.
We acknowledge limitations of this current study including a moderate sized cohort that may not be powered to detect subtle differences. However, it may be argued that subtle differences may not necessarily be of clinical significance. We also performed outlier analysis that would allow us to detect clinically significant deviations from the average tendency and found no significant outliers for COVID phenotypes. We also acknowledge that none of these patients presented with acute coronary syndrome, myocarditis, venous thromboembolism which have been reported as particularly serious cardiovascular complications that have been reported in acute COVID-19 infection and therefore represent a select group of patients with COVID-19. Our study population represented altogether a relatively young group of COVID-19 patients few comorbidities. While additional work should be done to investigate long-term cardiac outcomes in COVID-19 patients presenting with myocarditis, acute coronary syndromes and thromboembolism as well as those with post-acute sequelae of COVID-19, it is reassuring that in this cohort of patients from the early virulent phase of the pandemic when there were no vaccinations there is limited lasting damage to the heart from COVID-19.
Supplementary Material
qyad034_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Altay S. COVID-19 myocarditis cardiac magnetic resonance findings in symptomatic patients. Acta Radiol 2022;63:1475–80.34623175 10.1177/02841851211046502 PMC 9548510 · doi ↗ · pubmed ↗
- 2Lala A, Johnson KW, Januzzi JL, Russak AJ, Paranjpe I, Richter F et al Prevalence and impact of myocardial injury in patients hospitalized with COVID-19 infection. J Am Coll Cardiol 2020;4:533–46.10.1016/j.jacc.2020.06.007PMC 727972132517963 · doi ↗ · pubmed ↗
- 3Montero-Cabezas JM, Córdoba-Soriano JG, Díez-Delhoyo F, Abellán-Huerta J, Girgis H, Rama-Merchán JC et al Angiographic and clinical profile of patients with COVID-19 referred for coronary angiography during SARS-Co V-2 outbreak: results from a collaborative, European, multicenter registry. Angiology 2022;73:112–9.34318686 10.1177/00033197211028760 · doi ↗ · pubmed ↗
- 4Faridi KF, Hennessey KC, Shah N, Soufer A, Wang Y, Sugeng L et al Left ventricular systolic function and inpatient mortality in patients hospitalized with coronavirus disease 2019 (COVID-19). J Am Soc Echocardiogr 2020;33:1414–5.32951969 10.1016/j.echo.2020.08.016PMC 7442910 · doi ↗ · pubmed ↗
- 5Puntmann VO, Carerj ML, Wieters I, Fahim M, Arendt C, Hoffmann J et al Outcomes of cardiovascular magnetic resonance imaging in patients recently recovered from coronavirus disease 2019 (COVID-19). JAMA Cardiol 2020;5:1265–73.32730619 10.1001/jamacardio.2020.3557 PMC 7385689 · doi ↗ · pubmed ↗
- 6Brito D, Meester S, Yanamala N, Patel HB, Balcik BJ, Casaclang-Verzosa G et al High prevalence of pericardial involvement in college student athletes recovering from COVID-19. JACC Cardiovasc Imaging 2021;14:541–55.33223496 10.1016/j.jcmg.2020.10.023PMC 7641597 · doi ↗ · pubmed ↗
- 7Wang H, Li R, Zhou Z, Jiang H, Yan Z, Tao X et al Cardiac involvement in COVID-19 patients: mid-term follow up by cardiovascular magnetic resonance. J Cardiovasc Magn Reson 2021;23:14.33627143 10.1186/s 12968-021-00710-x PMC 7904320 · doi ↗ · pubmed ↗
- 8Wojtowicz D, Dorniak K, Ławrynowicz M, Rejszel-Baranowska J, Fijałkowska J, Kulawiak-Gałąska D et al Spectrum of lesions visualized in cardiac magnetic resonance imaging in COVID-19-related myocarditis: findings from a pilot study of the TRICITY-CMR trial. Cardiol J 2021;28:976–8.34708861 10.5603/CJ.a 2021.0139 PMC 8747819 · doi ↗ · pubmed ↗