Evaluation of double-chambered right ventricle flow using 4D flow MRI: right ventricular helical flow may not disappear even after surgical intervention
Hideharu Oka, Keita Ito, Sadahiro Nakagawa, Kunihiro Iwata, Kouichi Nakau

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
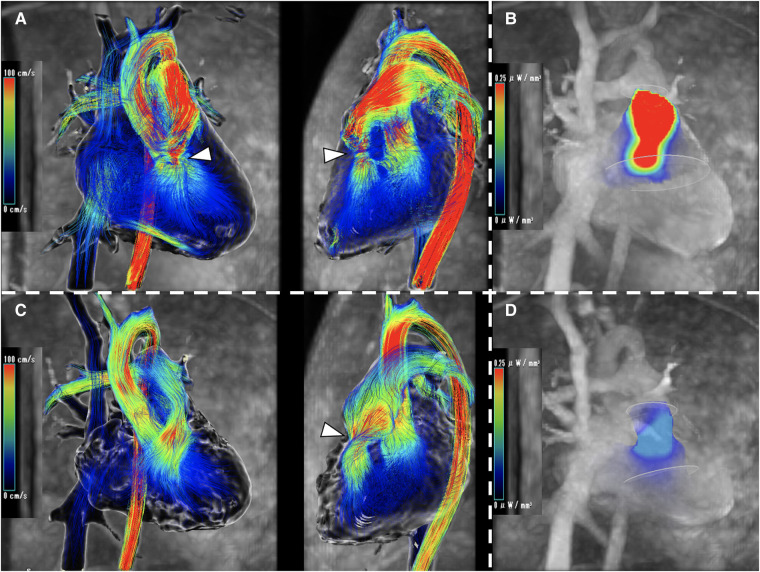 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Function and Risk Factors · Cardiac Valve Diseases and Treatments · Pulmonary Hypertension Research and Treatments
An 18-year-old male was diagnosed with a perimembranous ventricular septal defect (VSD) at birth and followed up. At 10 years old, the defect size was 3 mm, echocardiography showed right ventricular (RV) outflow obstruction (continuous wave 2 m/s), and he developed a double-chambered right ventricle (DCRV). At 18 years old, blood flow was 5 m/s by echocardiography and the pressure gradient (PG) was 37 mmHg by cardiac catheterization under sedation, and he wanted treatment. The thickened muscle bundle resection and VSD patch closure were done, and post-operative measurements with a Swan–Ganz catheter showed that the PG had disappeared. Echocardiography also showed that blood flow improved to 1.4 m/s, and the obstruction was sufficiently released. 4D flow MRI showed significant helical flow before surgery (Panel A, Supplementary data online, Video S1). The energy loss (EL, highest/mean value) was 7.54/1.87 mW (EL 0.57/0.16 mW in a healthy subject) (Panel B). Post-operatively, the helical flow was reduced but remained (Panel C, Supplementary data online, Video S2), and the EL was also lower at 1.45/0.42 mW, but higher than normal (Panel D). One month later, blood flow has accelerated to 2.3 m/s. The patient is being carefully monitored. The RV outflow obstruction is an ongoing process that may not depend only on PG, but cellular apoptosis and/or proliferation may be subjected to intracavitary blood vortices and surgery should look at imaging in pre-/post-surgical planning. In patients with DCRV, if the helical flow does not disappear after surgery, careful follow-up is needed to watch for recurrence.
Supplementary Material
qyad042_Supplementary_Data