Huge pseudoaneurysm of the left ventricular outflow tract developed a few years after surgery for subvalvular mitral aneurysm: to plug or not to plug it is the question
Humberto Morais, Elsa Fernandes, Mauer A A Gonçalves

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
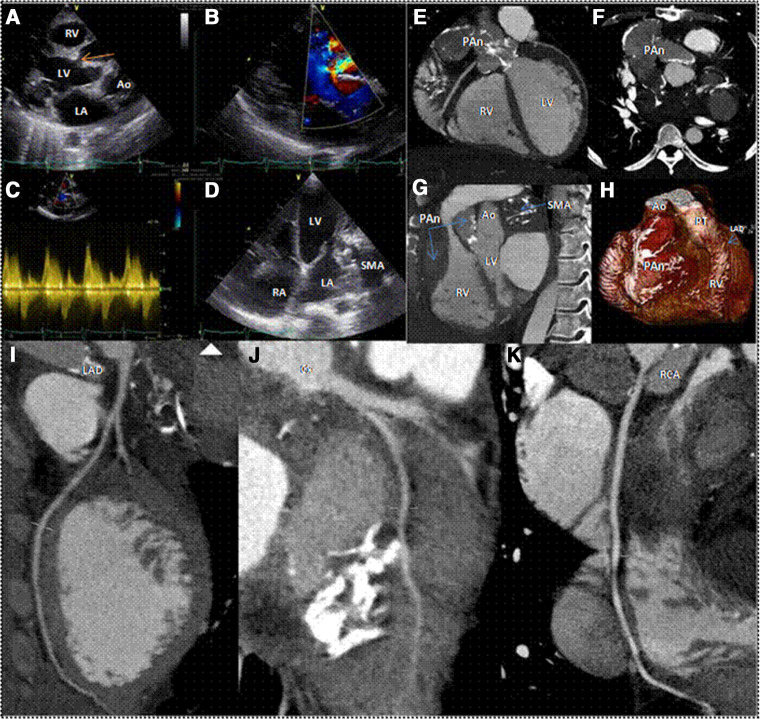 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Structural Anomalies and Repair · Infective Endocarditis Diagnosis and Management · Cardiac Valve Diseases and Treatments
A 36-year-old male patient presented with dyspnoea, fatigue, and pre-syncope episodes during moderate exertion. Relevant history included surgery for a subvalvular mitral aneurysm (SMA) performed 14 years earlier. Although surgery was done suspecting a type A aortic aneurysm, the diagnosis was not confirmed intraoperatively. Detailed surgical notes were not available. Physical examination revealed a systolic-bar murmur in the third left intercostal space. 2D-transthoracic echocardiography and Doppler study displayed a large structure linked to the left ventricle through a narrow neck (Panel A, arrow), showing a turbulent jet filling a pseudoaneurysm (Panel B) with a high gradient between the ventricle and the pseudoaneurysm (Panel C). An operated SMA aneurysm was also observed (Panel D).
A 64-slice gated CT (Panels E, F, and G, Supplementary data online, Movies S1, S2, and S3) with volume rendering (Panel H) confirmed the presence of SMA (Panel G) and also showed a massive pseudoaneurysm from the left ventricular outflow tract (LVOT), impacting the right atrioventricular groove and the ascending aorta, compressing the right ventricle (Panels G and H).
Both the LVOT pseudoaneurysm and SMA shape the atrioventricular groove without evident coronary artery compression (Panels I, J, and K). This image spotlight exemplifies the case of a patient with a long-standing LVOT pseudoaneurysm. LVOT pseudoaneurysms are rare, often post-infective endocarditis or cardiac surgery. Surgical repair is generally advised, but percutaneous closure (PC), when feasible, may be preferred in high-risk cases. However, due to PC unavailability and high surgical risk, the patient was managed conservatively with furosemide 40 mg twice a day; losartan 25 mg once a day, spironolactone 25 mg once a day, carvedilol 6.25 mg twice a day. He is currently in NYHA Class II.
Ao, aorta; Cx, circumflex artery; LA, left atrium; LAD, left anterior descending artery; LV, left ventricle; PAn, pseudoaneurysm; RCA, right coronary artery; RA, right atrium; RV, right ventricle.
Supplementary Material
qyae002_Supplementary_Data