Multi-modality cardiac imaging confirms quadricuspid aortic valve and excludes papillary fibroelastoma
Malgorzata Wamil, Marcos Goncalves

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
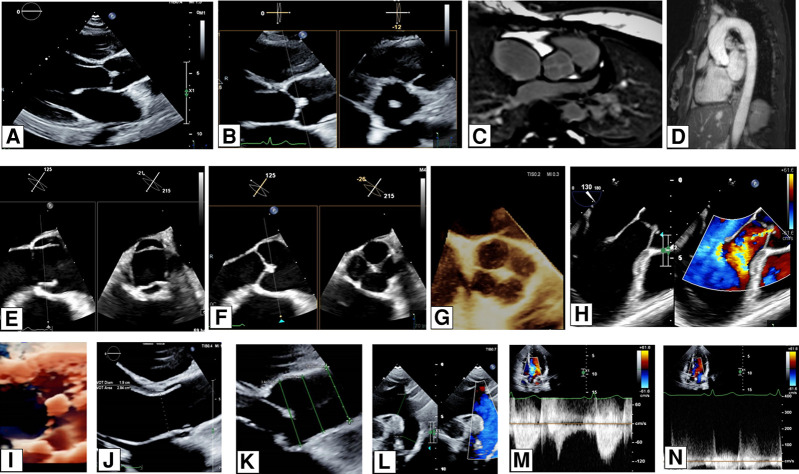 Figure 1
Figure 1 Figure 2
Figure 2- —Mayo Clinic International
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac tumors and thrombi · Cardiac Valve Diseases and Treatments · Infective Endocarditis Diagnosis and Management
A 26-year-old woman presented with a history of frequent sharp, left-sided chest pains, which were not associated with exercise. She had no significant past medical history. Her resting electrocardiogram (ECG) appeared normal, and the auscultation of her heart revealed no additional murmur. As part of her diagnostic workup, she underwent a transthoracic echocardiogram (TTE), which incidentally revealed a quadricuspid aortic valve (AV). It also raised suspicion of a mass attached to the cusps of the AV on the aortic side (Figure 1A and B) and suspected papillary fibroelastoma. To further investigate the anatomy of the AV, assess the ascending aorta, and characterize the suspected mass, cardiac magnetic resonance imaging (MRI) and a transoesophageal echocardiography (TOE) were performed. The TOE confirmed an X-shaped opening of the AV instead of the usual Y-shaped opening. The 3D TOE and CMR images clearly visualized the AV, showing a round opening. The valve was found to have four equal cusps, classifying it as a type A quadricuspid AV according to the Hurwitz and Roberts classification (Figure 1C–G). Doppler examination revealed a central jet of aortic regurgitation, which was quantified as mild based on various parameters (TTE colour Doppler and CMR phase contrast velocity AR regurgitation fraction 3%). Further imaging with CMR non-contrast aortogram confirmed no evidence of associated aortopathy (Figure 1D, H). Significantly, neither the TOE nor the CMR images identified any mass attached to the AV cusps (see Supplementary data online, Video S1). Instead, the thickening observed in the centre of cusp coaptation on the initial TTE images was confirmed to be consistent with the aberrant anatomy of the valve. This case highlights the valuable role of multi-modality cardiac imaging techniques in comprehensively assessing the anatomy and function of the AV. Considering those imaging techniques’ availability and cost, TTE will be used for annual follow-ups.
Supplementary Material
qyae025_Supplementary_Data