Primary Low-Grade Peritoneal Serous Carcinoma in a Woman With Psammoma Bodies on Cervicovaginal Cytology
Eduardo Gonzalez-Bosquet, Marta Avella Marcos, Carlota Rovira
TL;DR
A 62-year-old woman with rare psammoma bodies in her cervicovaginal cytology was diagnosed with low-grade peritoneal serous carcinoma after thorough investigations.
Contribution
This case highlights the importance of ruling out malignancy when psammoma bodies are found in cervicovaginal cytology.
Findings
Psammoma bodies in cervicovaginal cytology were found to be associated with low-grade peritoneal serous carcinoma.
A complete gynecological examination and laparoscopic surgery were necessary to confirm the diagnosis.
Adjuvant chemotherapy with carboplatin and paclitaxel was administered following the diagnosis.
Abstract
Psammoma bodies in cervicovaginal cytology are a rare finding associated with malignant tumours. A 62-year-old woman was referred to our centre for cytology with nuclear atypia and psammomatous bodies suspicious of malignancy. A complete gynaecological examination was performed including colposcopy and ultrasound without significant changes. Hysteroscopy was performed to detect endometrial or endocervical malignancy, endometrial biopsy showed psammoma bodies and atrophic endometrium. Endocervical and cervical biopsies were negative for malignancy. Cervicovaginal cytology and human papillomavirus (HPV) testing were repeated. The result was suggestive of adenocarcinoma and negative for HPV. Laparoscopic hysterectomy with bilateral salpingo-oophorectomy was indicated due to two cervicovaginal cytologies with suspicion of malignancy. Low-grade peritoneal serous carcinoma was diagnosed on…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
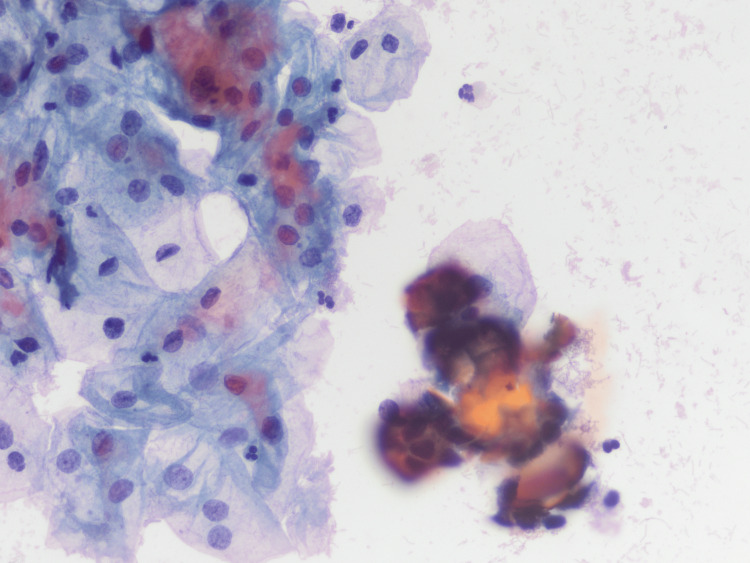 Figure 1
Figure 1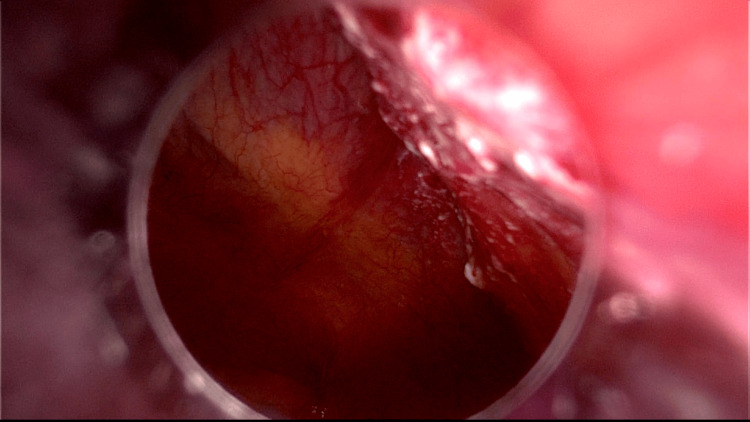 Figure 2
Figure 2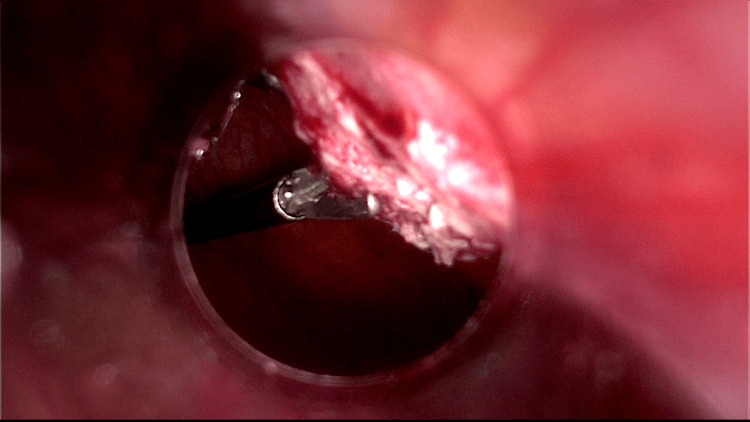 Figure 3
Figure 3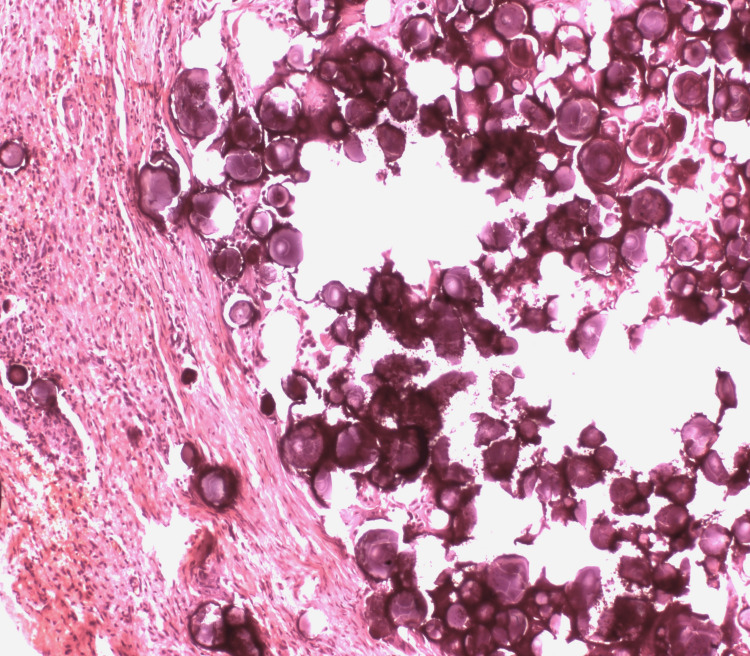 Figure 4
Figure 4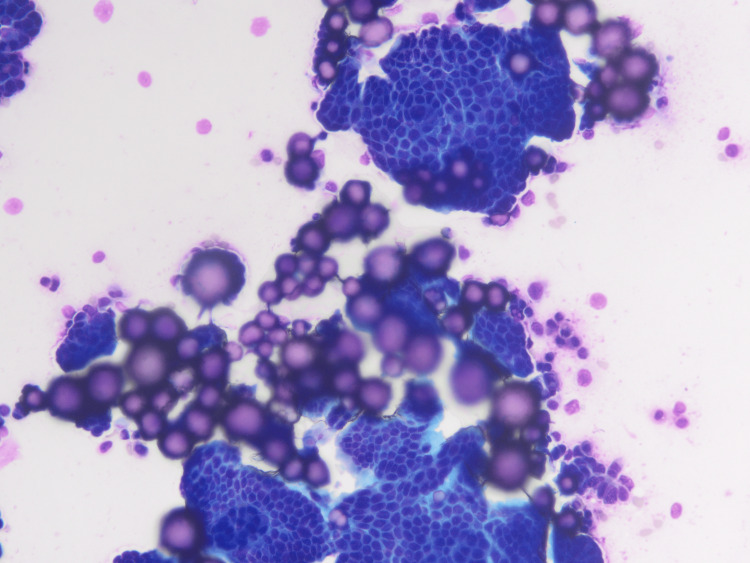 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAstronomy and Astrophysical Research · Particle Detector Development and Performance · Planetary Science and Exploration
Introduction
Primary peritoneal carcinoma (PPC) is a rare neoplasm that diffusely affects the peritoneal surface with minimal ovarian involvement [1-4]. PPC is indistinguishable from ovarian cancer and has similar clinical behaviour, patterns of spread, response to treatment and survival rates [5-7]. Most of the literature evaluating PPC has focused on patients with high-grade serous tumours [8]. Psammoma bodies in cervical smears are associated with malignancy, particularly ovarian cancer [9].
We present the case of a woman who had psammoma bodies on her cervical smears and was diagnosed with primary low-grade peritoneal serous carcinoma.
Case presentation
A 62-year-old woman with a significant history of hypertension, type 2 diabetes mellitus and a BMI of 31. She was referred to our centre for cytology with nuclear atypia and psammomatous bodies (PB) suspicious of malignancy (Figure 1).
Gynaecologic pap: cervical cytology with glandular cells with low atypia and occasional calcification (PAPX400).
A complete gynaecological examination was performed including colposcopy and ultrasound. Colposcopy showed a type 3 transformation zone without any lesion in the cervix and vagina. The vaginal ultrasound did not reveal uterus or ovarian alterations, and the endometrium was 2 mm thick. A new cervical smear showed glandular changes suggestive of adenocarcinoma, and endocervical curettage and HPV testing were negative.
Hysteroscopy was performed to detect endometrial or endocervical malignancy, with negative results. Multiple endometrial, endocervical and cervical biopsies were performed. Endometrial biopsy showed psammoma bodies and atrophic endometrium, a benign endocervical polyp was removed, endocervical curettage revealed a low-grade intraepithelial lesion (LSIL), and cervical biopsy was negative (no atypia).
Cervicovaginal cytology and HPV testing were repeated a month after hysteroscopy. The cervical smear was suggestive of adenocarcinoma and the HPV result was negative for infection.
Due to two cervical smears suspected of malignancy, a laparoscopic hysterectomy with bilateral salpingo-oophorectomy was recommended in May 2022. The case was not presented in the tumour board because the risk of malignancy was thought to be low since all previously performed biopsies and imaging tests were negative. During surgery, a white area of 2-3 cm on the peritoneal surface near the umbilical trocar was noted on the examination of the abdominal cavity (Figure 2) and a biopsy was performed (Figure 3).
An abnormal white area on the peritoneal surface near the umbilical trocar can be seen through a laparoscopic view.
A laparoscopic view of the biopsy performed on peritoneum.
The pelvis had a green fluid that was aspirated for cytological examination. Despite being normal, the uterus and ovaries showed certain adhesions to both the fallopian tubes and the peritoneum. A hysterectomy was performed without any complications, and the uterus, ovaries and fallopian tubes were removed vaginally.
The postoperative period was uneventful and the patient was discharged two days after surgery. Histological examination showed proliferation of glandular epithelium with papillary structures and mild atypia, areas of fibrosis and multiple psammoma bodies on the surface of the uterus, ovaries, fallopian tubes and in the peritoneal biopsy without invasion, suggestive of low-grade peritoneal serous carcinoma (Figure 4).
Dense fibrous tissue containing psammomatous calcifications suggestive of low-grade peritoneal serous carcinoma (H&E).
Cytologic study of the peritoneal fluid shows atypical cells with psammoma bodies suggestive of malignancy (Figure 5).
Serous fluid cytopathology with highly cellular smears with mesothelial cells and numerous psammoma bodies (DQ and pap x400).
The case was presented to the tumour board and magnetic resonance imaging (MRI) was performed to rule out other pelvic lesions. Small images measuring 9 to 4 mm were observed in the pelvis MRI. Ca 125 and HE4 tumour markers were negative (17 U/mL and 55 pmol/L). A new laparoscopy was carried out and 4-mm nodules were resected. An omentectomy and several peritoneal biopsies were also performed, but no tumour lesions remained. Lymphadenectomy was not performed because no suspicious lymph nodes were observed on MRI.
Histological examination of all biopsies revealed a similar lesion to that found in the previous biopsies, suggesting a low-grade peritoneal serous carcinoma. The case was presented to the tumour board and classified as stage IIIC cancer due to the involvement of the omentum and peritoneal. It was recommended to receive six cycles of carboplatin and paclitaxel as adjuvant treatment. The treatment was finished in April 2023. The patient has been disease-free 19 months after diagnosis.
Discussion
It is uncommon to find psammoma bodies in cervical smears [9]. In a large study of 234,318 cervicovaginal smears, only seven smears contained psammoma bodies (prevalence 0.00003)[10]. Four of the seven were associated with cancer: two papillary serous carcinomas of the endometrium, one serous cystadenocarcinoma of the ovary and one papillary serous carcinoma of the peritoneum [10], the latter being similar to our case.
Other studies have found approximately 61-50% of cases of women with PB in cervicovaginal smears are associated with benign conditions, such as endosalpingiosis [9-11]. Other authors associate the presence of psammoma bodies with endometrial changes due to the use of a combined oral contraceptive agent [12]. Women with PB and benign conditions are younger (mean age 42.7 years), do not have symptoms suggestive of malignancy and do not have highly atypical or malignant appearing glandular cells [11]. Women with PB and underlying malignancy were older (mean age 56 years) and postmenopausal, in our case 62 years, and had highly atypical or malignant glandular cells, as in our case.
In our case, the presence of psammoma bodies in the endometrial biopsy suggests that these structures passed through the tube and endometrial cavity to the cervix.
We found few studies in the literature regarding low-grade serous PPC, Schmeler et al. described one of the largest series with 53 cases [8], most cases were diagnosed with stage III as in our case. HE4 and CA125 levels were not significantly elevated in low-grade PPC [13]. The primary treatment was surgical cytoreduction, which was achieved in 46 patients (86.8%) in Schmeler et al.’s series [8], an optimal surgical cytoreduction was also achieved in our case. Most patients (88%) received systemic therapy, with a combination of taxane and platinum [8-14], as in our case.
It is also noteworthy that 69.3% of women with low-grade PPC were overweight, as in our case, with BMI of 31, compared to women with low-grade serous ovarian cancer [15].
Conclusions
The finding of psammoma bodies in cervicovaginal cytology is a rare clinical situation and it is imperative to rule out malignancy especially when associated with glandular cells of highly atypical or malignant appearance. Ovarian, endometrial or primary peritoneal cancer must be excluded.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Low-grade serous ovarian cancer: State of the science Gynecol Oncol Slomovitz B Gourley C Carey MS 71572515620203196925210.1016/j.ygyno.2019.12.033 · doi ↗ · pubmed ↗
- 2The peritoneal cancer index as a predictor of complete cytoreduction at primary and interval cytoreductive surgery in advanced ovarian cancer Int J Gynecol Cancer Fagan PJ Gomes N Heath OM 175717633320233789087510.1136/ijgc-2022-004093 · doi ↗ · pubmed ↗
- 3Papillary serous carcinoma of the peritoneum Obstet Gynecol Fromm GL Gershenson DM Silva EG 8995751990 https://pubmed.ncbi.nlm.nih.gov/2296429/2296429 · pubmed ↗
- 4Ovarian involvement by serous surface papillary carcinoma Int J Gynecol Pathol Mulhollan TJ Silva EG Tornos C Guerrieri C Fromm GL Gershenson D 120126131994800573210.1097/00004347-199404000-00003 · doi ↗ · pubmed ↗
- 5Primary peritoneal papillary serous adenocarcinoma: Clinical and management aspects Gynecol Oncol Altaras MM Aviram R Cohen I Cordoba M Weiss E Beyth Y 23023640199010.1016/0090-8258(90)90283-q 2013445 · doi ↗ · pubmed ↗
- 6Papillary serous carcinoma of the peritoneal surface: Matched-case comparison with papillary serous ovarian carcinoma Gynecol Oncol Killackey MA Davis AR 171174511993827628910.1006/gyno.1993.1267 · doi ↗ · pubmed ↗
- 7Extraovarian peritoneal serous papillary carcinoma: A case-control retrospective comparison to papillary adenocarcinoma of the ovary Gynecol Oncol Bloss JD Liao SY Buller RE 347351501993840619910.1006/gyno.1993.1223 · doi ↗ · pubmed ↗
- 8Low-grade serous primary peritoneal carcinoma Gynecol Oncol Schmeler KM Sun CC Malpica A Deavers MT Bodurka DC Gershenson DM 48248612120112139730510.1016/j.ygyno.2011.02.017 · doi ↗ · pubmed ↗