Groin pain aggravated in short term contracted by COVID-19 in THA patients: a case-crossover study
Hongjie Chen, Peng Lai, Haiming Lu, Jun Zhu, Weilin Sang, Cong Wang, Yiming Zhong, Libo Zhu, Jinzhong Ma

TL;DR
This study finds that patients who had hip replacement surgery and later contracted COVID-19 experienced worsened groin pain, with longer hospital stays linked to higher risk.
Contribution
The study is the first to investigate the link between postoperative groin pain aggravation in THA patients and short-term COVID-19 infection.
Findings
Patients with THA who contracted COVID-19 had a 9.5-fold increased risk of groin pain aggravation.
Longer hospital stays were independently associated with increased risk of pain aggravation (OR 1.26).
Abstract
The coronavirus disease 2019 (COVID-19) rapidly spreads worldwide and causes more suffering. The relation about the aggravation of inguinal pain and COVID-19 was unclear in patients with total hip arthroplasty (THA). This study aimed to evaluate the risk of groin pain aggravation in short-term THA patients after COVID-19. Between 2020 and 2022, 129 patients with THA who were affected COVID-19 were enrolled. A short-standardized questionnaire was administered during follow-up to inquire about the aggravation of groin ache before and after SARS-COV-2 affection. Furthermore, we evaluated the potential association between the presence of increased pain and various factors, including age, gender, body mass index, diagnosis, and length of hospital stay. The case-crossover study revealed an increased risk of inguinal soreness aggravation when comparing 8 weeks after COVID-19 with 12 weeks…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
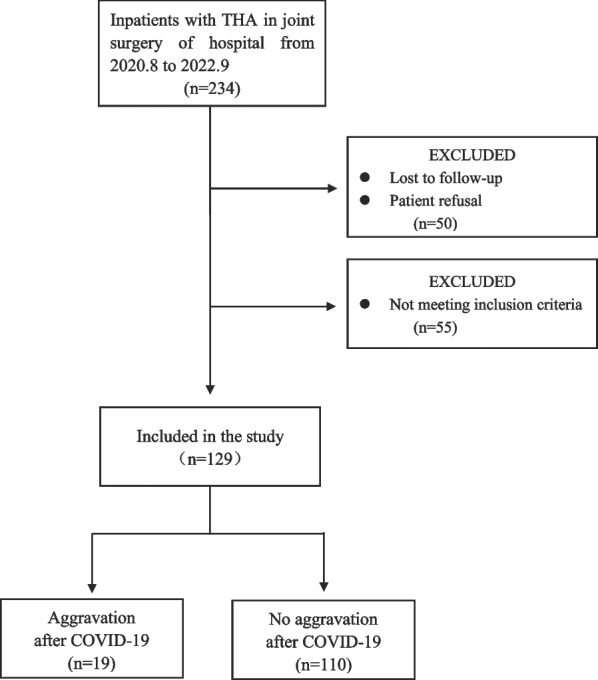 Figure 1
Figure 1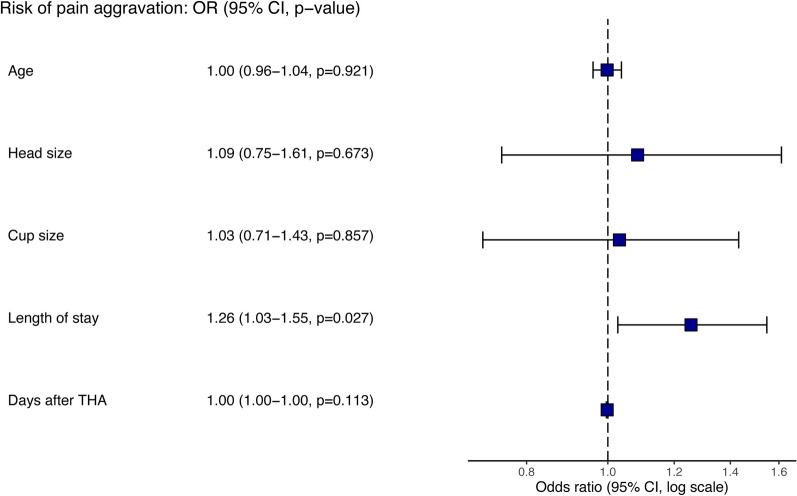 Figure 2
Figure 2- —Medical Engineering Cross Research Project of Shanghai Jiaotong University
- —National Natural Science Foundation of China
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOrthopedic Infections and Treatments · Orthopaedic implants and arthroplasty · Total Knee Arthroplasty Outcomes
Introduction
Total hip arthroplasty (THA) is a reliable procedure that effectively reduces pain, improves function, and enhances the quality of life for patients with advanced hip disease [1, 2]. Over the past 2–3 decades, the number of arthroplasty procedures has increased, and is projected to rise by 176% by 2040 and 659% by 2060 in THA procedures [3–5]. Although primary THA has been voted the most successful operation of the century, more than 10% of patients report postoperative dissatisfaction [6–8]. Postoperative pain is one of significant reasons for dissatisfaction, which affects up to 18.3% of patients at 3 months and 12.9% at 24 months of follow-up [9]. The most common causes include infection, aseptic loosening of the acetabular component, iliopsoas tendonitis, impingement, synovitis due to metal or polyethylene debris [10]. This pain can lead to immobility, contributing to various medical complications [11], such as venous thrombosis and pneumonia, with potentially serious health consequences.
To make matters worse, SARS-COV-2 infection may cause more disturbing for THA patients [12–14]. Notably, the prevalence of arthralgia or myalgia during the COVID-19 pandemic was reported to be 15.5% within the first 5 months [15], while new-onset chronic pain (> 3 months) affected 19.6% of COVID-19 patients [16]. SARS-COV-2, the virus responsible for COVID-19, primarily invades the respiratory system and triggers a systemic inflammatory response characterized by upregulated inflammatory cells and factors [17], which induces muscle and joint pain [18].
Studies have shown that THA patients have higher levels of inflammatory cells and cytokine in the periprosthetic tissues than normal [19], such as tissue damage from surgery and chronic inflammation from wear debris [20]. Thus, the inflammatory response following SARS-COV-2 infection may be the stronger or earlier to occur in the THA patients than the healthy [21], with a higher likelihood of pain occurring [22]. In turn, the inflammatory storm caused by SARS-COV-2 infection further inhibits the repair of periprosthetic tissues, adversely affecting THA patients [22]. Hence, the phenomenon is all the more worthy of our attention.
Previous studies have confirmed COVID-19 causes pain, such as arthralgia or myalgia, but whether it increases groin pain in short-term THA patients has not been explored. Therefore, this study aimed to investigate the association between COVID-19 and increased pain in inguinal area in THA patients. By addressing this research gap, we aim to provide valuable insights for clinical practice.
Methods
Patient selection
Patients who underwent primary THA between August 5, 2020, and September 23, 2022, were reviewed. All THAs were performed by the same surgeon group in the center with uncemented implants. In accordance with the standard, a rehabilitation physician will perform hip flexion and extension exercises as well as muscle strength restoration training for the patient 24 h after the operation. And after 72 h, the patient will be assisted to go down to the ground with the aid of a walker under the guidance of the rehabilitation physician. The following inclusion criteria were applied: (1) all patients tested negative for COVID-19 before THA, as confirmed by polymerase chain reaction (PCR) test and medical history; (2) patients had indications for hip arthroplasty other than malignancy (osteoarthritis, development dysplasia, and femoral neck fracture); (3) patients had no inflammatory disease or immunosuppression; (4) patients were infected with SARS-COV-2 after a 12-week recovery period after THA;
Data collection
Patient characteristics, including age, gender, height, weight, body mass index (BMI), the surgical approach for THA, length of stay for THA, comorbidities, complications and X-rays were collected from the electronic patient medical record system of hospital. A short-standardized questionnaire (supplymentary 1) was administered by specialized doctor via phone interview to gather information on the incidence of COVID-19 and the occurrence of groin ache aggravation. The treatment for COVID-19 (such as inhaled steroids or anti-virals drug) and treatment outcomes (weather become septic or admitted to ICU or die) were also recoreded. To rule out the effects of surgical trauma, we included the occurrence of aggravation of pain from 3 months after THA. The timing and duration of pain aggravation until it returned to baseline levels were recorded. COVID-19 was defined as a positive PCR test or antigen test for SARS-COV-2, and the date of COVID-19 positivity was defined as the day of a positive test. The COVID-19 tests are conducted by qualified institutions and subjects can query the results in the next day.
Study design
In case cross-over study, the time of positive test was set as time zero and the study was divided in two times frames: 12 weeks before time zero to time zero (control period) and time zero to 8 weeks after time zero (risk period). The 8-week time window was chosen as a short period to observe immediate risks following infection [23]. When the patient was included, detailed questions about the pain was asked by standardized questionnaire and the occurrence of pain aggravation in COVID-19 positive patients was calculated in the two times frames. The final follow-up was conducted on May 1, 2023.
Statistical analysis
Statistical analyses were performed using the Statistical software (IBM, Armonk, NY). The McNemar test was used to investigate the differences in categorical variables (pain aggravation or not), and the chi-square test was applied to calculate the relative risk (RR) with 95% confidence intervals (95% CI) in the frequencies of pain aggravation by comparing the 8-week period after COVID-19 (risk period) with the 12-week period before COVID-19 (control period). Risk factors for increased pain in COVID-19 patients were evaluated using univariate analysis with the occurrence of pain aggravation as the dependent variable. For categorical variables, χ^2^ test was used. For continuous variables, the t-test is used for data that conforms to a normal distribution, and the non-parametric test is used for non-normally distributed data. In addition, age, head size, cup size, length of stay and days after THA were included in multivariate logistic regression models based on univariate analyses with p < 0.1 and clinical experience, and odds ratios (OR) and respective 95% confidence intervals (CI) were calculated using the R (version 4.3.0) with R Studio (version 2023.03.1 + 446). The cut-off for statistical significance was set at p < 0.05.
Results
Patient characteristics
The flow diagram was shown in Fig. 1. One hundred and twenty-nine patients were registered as positive for COVID-19 (Table 1) during the study period. Of those, 44 (34.1%) were men and the mean age was 63.7 years (standard deviation [SD], 13.8). The media of body mass index (BMI) were 23.9 kg/m^2^ (interquartile range [IQR], 21.9–26.9). And 119 THAs (92.2%) were performed using the direict anterior approach (DAA), with a median length of stay of 8 days (IQR,7–10). The 106 patients (82.2%) were treated only with symptomatic treatment (including physical cooling, NSAID or cough expectorant drugs), and the rest were combined with antiviral therapy (inclding ribavirin, molnupiravir, lopinavir, ritonavir, favipiravir, etc.). None had received treatment with hormones or immunosuppressants. None of the patients affected by COVID-19 experienced sepsis, ICU, or death. Characteristics of increased groin pain in short-term THA patients are shown in Table 2. For the two patients who experienced increased pain prior to infection, they suffered for 78 days and 238 days, respectively, and had not yet recovered. All patients with increased pain had no abnormality after X-ray review.Fig. 1. Flow diagramTable 1Baseline characteristics of the COVID-19 positive patientsCharacteristicsCOVID-19 positive patients(n = 129)Men, n, (%)44 (34.1%)Age, years, mean (SD)63.7 (13.8)Height, cm, median (SD)159.4 (8.3)Weight, kg, mean (SD)62.3 (12.2)BMI, kg/cm^2^, median [IQR]23.9 [21.9, 26.9]Clinical characteristicsHypertension, n, (%)37 (28.9%)Diabetes, n, (%)46 (35.7%)ASA score2 [1, 2]Diagnosis, n, (%)Degenerative joint disease79 (61.2%)DDH17(13.2%)Necrosis of the femoral head17(13.2%)Femoral neck fracture12 (9.3%)Others4 (3.1%)Approach, n, (%)DAA119 (92.2%)PLA10 (7.8%)Head size, cm, median [IQR]28 [28, 32]Cup size, cm, median [IQR]46 [46, 50]Length of stay, days, median [IQR]8 [7, 10]Follow-upDays after THA, days, median [IQR]578 [405, 808]Dislocation, n, (%)5 (3.9%)Periprosthetic fracture, n, (%)1 (0.8%)Treatment for COVID-19Symptomatic treatment106(82.2%)Symptomatic and antiviral treatment23(17.8%)COVID-19 Coronavirus disease 2019; BMI Body mass index; ASA American Society of Anesthesiologists; THA Total hip arthroplasty; DAA Direct anterior approach; PLA Posterolateral approach; IQR Interquartile range; SD Standard deviationTable 2Characteristics of increased groin pain in short-term THA patientsCharacteristicsPatients with increased groin painAfter COVID-19 (n = 19)Before COVID-19 (n = 2)Pain duration, days; median [IQR]21 [8–54]78、238Complete relief, n, (%)11(58%)/Partly relief, n, (%)3 (16%)/No relief, n, (%)5 (26%)2 (100%)COVID-19 Coronavirus disease 2019; THA Total hip arthroplasty; IQR Interquartile range
Risk of groin pain aggravation in patients with THA after SARS-COV-2 infection
In the case-crossover design, two patients (1.6%) experienced pain aggravation during the 12-week control period before COVID-19. Both of them suffered more serious pain in inguinal area during the 8-week risk period after COVID-19. Additionally, 17 patients (13%) who did not have pain aggravation before COVID-19 developed pain aggravation during the 8-week risk period after COVID-19. Significant differences in the incidence of pain aggravation were observed between risk period and control period (χ^2^ = 15.059, p < 0.0001) (Table 3). In risk period, 19 of 129 patients (14.7%) who were compared with two of 129 patients (1.6%) in the control period felt more pain with a significantly increased risk (RR, 9.5; 95%CI, 2.259–39.954; p < 0.001) (Table 4).Table 3. Differences of pain aggravation between control period and risk period in COVID-19 positive patientsCase-crossover design8 weeks after COVID-19(risk period)12 weeks before COVID-19(control period)Aggravation(n)No aggravation(n)All(n)Aggravation, n, (%)202No aggravation, n, (%)17110127All(n)19110129The McNemar test was used to investigate the differences in pain aggravation (yes or no) by comparing the 12-week period prior to the COVID-19 with the 8-week period after COVID-19 (risk period)Table 4. Frequency of aggravation in groin pain before and after SARS-COV-2 infectionCase-crossover designAggravation/AllRelative risk(95%CI)12 weeks before COVID-19(control period)2/129(1.6%)Reference8 weeks after COVID-19(risk period)19/129(14.7%)9.5(2.259–39.954)CI Confidence interval; COVID-19 Coronavirus disease 2019
Risk factors for pain aggravation in patients after SARS-COV-2 infection
The demographic and clinical features of patients with and without pain aggravation after COVID-19 are presented in Table 5. Univariate analysis showed there was no significant difference in all factors listed in the table between the groups of aggravation and no aggravation of pain after SARS-COV-2 infection. However, multivariate logistic regression analyses of possible risk factors for pain aggravation after COVID-19 revealed that the length of stay was an independent factor significantly associated with increased risk (OR 1.26; 95%CI, 1.03–1.55, p = 0.027) (Fig. 2).Table 5. Comparison analysis of the factors on the aggravation of groin pain in patients with THA after COVID-19 positiveCharacteristicsAggravation after COVID-19(n = 19)No aggravation after COVID-19(n = 110)p valueMen, n, (%)8 (42%)37 (34%)0.428Age, years, mean (SD)62.4(12)63.9 (14)0.670Height, cm, median (SD)159.6(9.2)159.3(8.2)0.899Weight, kg, mean (SD)63.6(15.0)62.1(11.8)0.637BMI, kg/cm^2^, median [IQR]24.7 [22.4, 28.3]23.9 [21.9, 26.8]0.537Hypertension, n, (%)3 (16%)34 (31%)0.189Diabetes, n, (%)6 (32%)40 (36%)0.688ASA score, median [IQR]2 [1, 2]2 [1, 2]0.763Approach in THA0.663DAA, n, (%)18 (95%)101 (92%)PLA, n, (%)1 (5%)9 (8%)Length of stay, days, median [IQR]8 [8, 13]8 [7, 10]0.056Days after THA, days, median [IQR]482 [336, 634]613.5 [409, 813]0.097Head size, cm, median [IQR]32 [28, 32]28 [28, 32]0.196Cup size, cm, median [IQR]48[46,50]46[46,50]0.234Dislocation, n, (%)1 (5%)4 (4%)0.736Treatment1.000 Symptomatic treatment16(12.4%)90(69.8%)Symptomatic and antiviral treatment3(2.3%)20(15.5%)COVID-19 Coronavirus disease 2019; BMI Body mass index; ASA American Society of Anesthesiologists; DDH Developmental dysplasia of the hip; THA Total hip arthroplasty; DAA Direct anterior approach; PLA Posterolateral approachFig. 2Forest plot. Odds ratios (OR) and 95% confidence intervals (CI) of factors of aggravation of groin pain in THA patients with COVID-19. Abbreviation: THA, total hip arthroplasty
Discussion
The present retrospective study aimed to investigate the relationship between COVID-19 and the aggravation of inguinal ache in patients who underwent THA. The findings suggest that SARS-COV-2 infection increases the risk of groin pain during the eight weeks following infection. This indicates that the influence of COVID-19 on patients who underwent THA extends beyond the acute phase, as they continue to experience pain aggravation.
Pain is often associated with viral illnesses and is believed to result from the acute cytokine response, typically resolving after fever subsides [24]. However, Hoong observed that COVID-19 related arthralgia appears to differ from generalized body aches and myalgia commonly seen in viral infections [25], as it does not align with the typical prodromal symptoms. In our study, although the 19 patients (14.7%) with pain aggravation account for a small percentage of the total 129 COVID-19 patients, we observed that these patients were usually older (with the mean age of 62.4 years), experienced prolonged symptoms (with the median pain duration of 21 days). In addition, pain occurred a few days before or after the onset of fever and respiratory symptoms, which differs from commonly viral infections.
In our case-crossover study, we found that groin soreness aggravation occurred shortly after a positive COVID-19 test in most of the 19 patients, suggesting a potential causal relationship. Afterwards, we observed a significant increase in the frequency of pain aggravation during the 8 weeks after COVID-19 when compared to the 12 weeks before COVID-19. In addition, the incidence of aggravation of inguinal pain within 8 weeks after SARS-COV-2 affection was almost 10 times higher than before. These results indicated that COVID-19 played a vital role in the aggravation of groin pain. However, Maezawa et al. demonstrated that patients with THA did not change significantly in hip pain before and after COVID-19 pandemic [26]. In Maezawa’s research, the division of group was based on the different phases of SARS-COV-2 epidemics in the population, and it is not certain that all subjects during the pandemic were infected with COVID-19. The two studies differ markedly in the time-point settings and infection status of subjects, thus the results are probably different.
For COVID-19 positive patients, the length of stay was associated with an increased risk of pain aggravation in the multivariate analyses. The evidence is overwhelming that the number of comorbidities, the American Society of Anesthesiologists (ASA) score > 2, and the presence of cardiac or pulmonary disease are related to the length of stay [27]. However, the common comorbidities in this study including diabetes (p = 0.688) and hypertension (p = 0.189) were not significantly different between aggravation group and no aggravation group, and the same for ASA score (p = 0.763). Moveover, risk factors [28] such as age [29], high BMI, frailty, anemia, and blood transfusions were involved with the length of stay while age (p = 0.670) and BMI (p = 0.537) did not differ significantly in our study. Thus, it can be hypothesized that frailty and poor health increase the length of stay, which account for this phenomenon, as frail patients face more severe challenges after SARS-COV-2 infection [30, 31].
It has been reported in the literature that different types of prosthesis have an effect on the incidence of pain, with dual-mobility prosthesis having the lowest incidence of pain, fixed-bearing (FB) prosthesis following, and hip resurfacing having the highest incidence of pain [32–34]. Furthermore, the larger femoral heads have previously been shown to present a higher likelihood of causing inguinal soreness than smaller femoral heads [32]. In our study, the patients were using FB prosthesis and we found that the size of the head (p = 0.196) and cup (p = 0.234) of the FB prosthesis had no effect on inguinal pain.
Factors that influenced pain after surgery also included preoperative anxiety/depression symptoms [35], preoperative pain intensity [36], preoperative sleep quality [37], and lower patient participation in pain management [38], with the exception of the duration of hip arthroplasty [39] and enhanced recovery after surgery (ERAS) [40]. While the effect of gender and ASA score on pain is controversial [35, 36, 41], and our study showed the gender (p = 0.428) and ASA score (p = 0.763) had no influence on soreness in the groin region.
In most patients with increased pain, it was observed that soreness in inguinal area persisted for more than a week. Among the 19 patients who experienced increased pain after COVID-19, 11 of them were completely relieved of pain after the acute phase, while 3 patients did not experience relief. Among the remaining 5 patients, 3 patients reported increased pain in response to weather changes. Although more than half of the 19 patients had a short duration of pain and returned to baseline levels without requiring hospitalization, it should not be ignored that eight patients (42%) continued to suffer from pain, which significantly impacted their daily lives for a period of 4 months or more. This finding aligns with the emerging syndrome of post-acute COVID-19, also known as “long COVID”, in which symptoms may remain for a long time after a relatively minor COVID-19 infection has recovered [42, 43]. Furthermore, as patients with THA experience the long-term impact or an extended course of COVID-19, clinicians must be cognizant of this in the diagnosis and management of patients with a history of COVID-19 who present with groin pain and adequately distinguish it from other diseases.
This study has some limitations. Inguinal pain aggravation was assessed via a “yes/no” scale, as it was easier for elderly patients to understand and answer simple questions, although a pain severity score can provide more details. Furthermore, the retrospective case-crossover design introduces the possibility of recall bias and reduces the accuracy of data collection. However, the design has inherent strengths, such as the close proximity of the retrospective control period and the fact that each patient serves as their own control [44]. These features help minimize potential confounding factors and enhance the efficiency of the study. To improve upon our study, future research should consider employing a more comprehensive assessment of pain severity to capture the nuanced nature of groin ache. Additionally, efforts should be made to include a larger number of COVID-19 positive patients to enhance the generalizability of the findings. Incorporating multi-center collaborations or longitudinal studies could overcome these limitations and provide a more comprehensive understanding of the relationship between COVID-19 and inguinal soreness in patients with THA.
Conclusions
The case-crossover study indicate that COVID-19 is associated with a significantly increased risk of aggravation of groin ache in THA patients during 8 weeks after COVID-19. Further research indicated that length of stay was associated with an increased risk of pain exacerbation. In summary, this study confirms the association between COVID-19 and the exacerbation of inguinal pain in THA patients. This study expands the current literature by investigating the risk of aggravation of groin pain in patients with THA after COVID-19, providing valuable insights into postoperative outcomes in this specific population.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file 1: Short-standardized questionnaire about groin pain.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mei XY Gong YJ Safir O Long-term outcomes of total hip arthroplasty in patients younger than 55 years: a systematic review of the contemporary literature Can J Surg 20196242492583134863210.1503/cjs.013118 PMC 6660275 · doi ↗ · pubmed ↗
- 2Mackenzie JRO'Connor GJ Marshall DA Functional outcomes for 2 years comparing hip resurfacing and total hip arthroplasty J Arthroplast 20122757507.e 210.1016/j.arth.2011.10.00422285258 · doi ↗ · pubmed ↗
- 3Shichman I Roof M Askew N Projections and epidemiology of primary hip and knee arthroplasty in medicare patients to 2040–2060 JB JS Open Access 202381 e 22.001123686490610.2106/JBJS.OA.22.00112 PMC 9974080 · doi ↗ · pubmed ↗
- 4Singh JA Epidemiology of knee and hip arthroplasty: a systematic review Open Orthop J 2011580852158427710.2174/1874325001105010080 PMC 3092498 · doi ↗ · pubmed ↗
- 5Rupp M Lau E Kurtz SM Projections of primary TKA and THA in germany From 2016 through 2040 Clin Orthop Relat Res 20204787162216333216805710.1097/CORR.0000000000001214 PMC 7310374 · doi ↗ · pubmed ↗
- 6Halawi MJ Jongbloed W Baron S Patient dissatisfaction after primary total joint arthroplasty: the patient perspective J Arthroplast 20193461093109610.1016/j.arth.2019.01.07530799270 · doi ↗ · pubmed ↗
- 7Learmonth ID Young C Rorabeck C The operation of the century: total hip replacement Lancet 20073709597150815191796435210.1016/S 0140-6736(07)60457-7 · doi ↗ · pubmed ↗
- 8Heath EL Ackerman IN Cashman K Patient-reported outcomes after hip and knee arthroplasty: results from a large national registry Bone Jt Open 2021264224323418279310.1302/2633-1462.26.BJO-2021-0053.R 1PMC 8244799 · doi ↗ · pubmed ↗